KIDNEY CONNECTION: INSIGHTS INTO CHRONIC KIDNEY DISEASE MANAGEMENT FOR THE INTERDISCIPLINARY HEALTHCARE TEAM
Faculty:
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson is an Associate Professor of Internal Medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson, PharmD, BCPS, is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy, where she is course director of the Parenteral Products and Basic Pharmaceutics Lab courses.
Kristina (Tia) Neu, RN
Kristina (Tia) Neu is a licensed Registered Nurse and author currently developing in-service training for healthcare professionals. She is a National Board-Certified Health & Wellness and Lifestyle Medicine Coach. Her work experience includes work in several areas of the healthcare profession, including psychiatric nursing, medical nursing, motivational health coaching, chronic case management, dental hygiene, cardiac technician, and surgical technician.
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and licensed pharmacist. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Abstract
Chronic kidney disease (CKD) affects nearly 15% of U.S. adults and remains a leading cause of morbidity, mortality, and healthcare costs. It is a progressive condition that significantly impacts patient outcomes and quality of life and is associated with a broad range of complications, including cardiovascular disease, electrolyte imbalance, anemia, and bone-mineral disorders. This interprofessional continuing education program provides an up-to-date overview of CKD detection, classification, and management in accordance with the 2024 Kidney Disease Improving Global Outcomes (KDIGO) guidelines. Learners will explore evidence-based strategies to slow disease progression, including pharmacologic interventions and team-based care approaches that optimize blood pressure, glycemia, and lipid control. Participants will also learn how to apply current guidelines, interpret key laboratory parameters such as eGFR and albumin-creatinine ratio, and contribute effectively to comprehensive, patient-centered renal care. This educational activity also highlights the roles of the healthcare team, reinforcing how collaborative care, patient education, and adherence support improve safety and outcomes in patients with CKD.
Accreditation Statements
In support of improving patient care, RxCe.com LLC is jointly accredited by the Accreditation CouncilTM for Continuing Medical Education (ACCME®), the Accreditation Council for Pharmacy Education (ACPE®), and the American Nurses Credentialing Center (ANCC®), to provide continuing education for the healthcare team.

This activity was planned by and for the healthcare team, and learners will receive 2 Interprofessional Continuing Education (IPCE) credits for learning and change.
Joint Universal Activity Number: The Joint Accreditation Universal Activity Numbers assigned to this activity are as follows:
Pharmacists: JA4008424-0000-26-009-H01-P
Pharmacy Technicians: JA4008424-0000-26-009-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit.
Credit Types:
IPCE Credits - 2 Credits
AAPA Category 1 Credit™️ - 2 Credits
AMA PRA Category 1 Credit™️ - 2 Credits
Pharmacy - 2 Credits
Type of Activity: Knowledge and Application
Media: Computer-Based Training (i.e., online courses)
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Course Test and course evaluation.
Release Date: January 26, 2026 Expiration Date: January 26, 2029
Target Audience: This educational activity is for Physicians, Physician Assistants, Pharmacists, and Pharmacy Technicians
How to Earn Credit: From January 26, 2026, through January 26, 2029, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Take the “Educational Activity Pre-Test;”
Study the section entitled “Educational Activity;” and
Complete the Educational Activity Post-Test and Activity Evaluation. The Educational Activity Post-Test will be graded automatically. Following successful completion of the Educational Activity Post-Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
CME Credit: Credit for this course will be uploaded to CPE Monitor® for pharmacists. Physicians may receive AMA PRA Category 1 Credit™️ and use these credits toward Maintenance of Certification (MOC) requirements. Physician Assistants may earn AAPA Category 1 CME credit, reportable through PA Portfolio. All learners shall verify their individual licensing board’s specific requirements and eligibility criteria.
Statement of Need
Chronic kidney disease (CKD) affects an estimated 700 million people globally and is the 11th leading cause of death worldwide. Kidney replacement therapy is expected to be needed in 5.4 million people by 2030. Cardiovascular disease remains the primary cause of mortality in individuals presenting with CKD. Despite the 2024 KDIGO CKD guidelines emphasizing an interprofessional approach to care in patients with CKD, gaps in risk stratification, evidence-based interventions, and other significant practice gaps persist among interdisciplinary teams. Deficiencies in early detection and accurate CKD staging remain a contributing factor for suboptimal patient care. This activity aims to provide guidance on optimizing pharmacotherapy, managing complications, and implementing collaborative, patient-centered care to enhance team-based CKD management and patient outcomes.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Identify the latest diagnostic tools, biomarkers, and imaging techniques for early and accurate detection of chronic kidney disease (CKD)
Identify the different stages or classifications of CKD
Recall therapeutic management strategies for patients with CKD
Describe components of comprehensive care plans for patients with CKD and diabetes and patients with CKD and heart disease
Disclosures
The following individuals were involved in planning, developing, and/or authoring this activity: The following individuals were involved in developing this activity: Austin Fredrickson, MD, FACP; Liz Fredrickson, PharmD, BCPS; Kristina (Tia) Neu, RN; and Pamela M. Sardo, PharmD, BS. None of the individuals involved in developing this activity has a conflict of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity Pre-Test
Which statement describes the role of renal ultrasound in evaluating suspected CKD?
Assess kidney size, structure, and obstruction
To measure real-time GFR
Solely to determine the need for dialysis
To measure quantities of urine crystals
Which of the following medication classes is first-line for albuminuric CKD?
RAS inhibitors (ACEi/ARB)
Thiazide diuretics
Beta-blockers
DPP-4 inhibitors
Which combination reflects lifestyle components of a comprehensive CKD plan?
0 g/kg/day of protein intake, maintain a vegan diet, and bed rest
High protein diet, intense exercise despite comorbidities
0.8 g/kg/day protein intake, <2 g/day sodium intake
>20 g/day sodium intake, daily NSAID use
Educational Activity
Kidney Connection: Insights into Chronic Kidney Disease Management for the Interdisciplinary Healthcare Team
Introduction
Chronic kidney disease (CKD) affects an estimated 700 million individuals globally and contributes substantially to morbidity, mortality, and healthcare utilization.1 Chronic kidney disease is a progressive condition that often coexists with diabetes, hypertension, cardiovascular disease (CVD), and heart failure, and its management requires a coordinated, multidisciplinary approach centered around early detection, risk stratification, and evidence-based interventions.1 The 2024 Kidney Disease Improving Global Outcomes (KDIGO) CKD Guideline provides a detailed framework for the evaluation and management of CKD, incorporating new evidence from large randomized controlled trials (RCTs) and contemporary systematic reviews.1
This interprofessional continuing education program provides an up-to-date overview of CKD detection, classification, and management in accordance with the 2024 Kidney Disease Improving Global Outcomes (KDIGO) guidelines. Learners will explore evidence-based strategies to slow disease progression, including pharmacologic interventions and team-based care approaches that optimize blood pressure, glycemia, and lipid control. Participants will also learn how to apply current guidelines, interpret key laboratory parameters such as eGFR and albumin-creatinine ratio, and contribute effectively to comprehensive, patient-centered renal care. This educational activity also highlights the roles of the healthcare team, reinforcing how collaborative care, patient education, and adherence support improve safety and outcomes in patients with CKD.
Epidemiology
Chronic kidney disease is a major global public health challenge. Based on Global Burden of Disease (GBD) data, CKD is now the 11th leading cause of death worldwide and continues to rise in prevalence.1 An estimated 5.4 million people will require kidney replacement therapy (KRT) by 2030, and this is driven in part by aging populations and an ever-increasing prevalence of diabetes and hypertension.1
Chronic kidney disease disproportionately impacts individuals from lower socioeconomic backgrounds and racial or ethnic minority groups.1 Cardiovascular disease remains the leading cause of death among individuals with CKD, with mortality risk escalating as eGFR declines and albuminuria increases.1 Early recognition and intervention are therefore critical to reducing both kidney-specific and cardiovascular complications.
Etiology
Chronic kidney disease arises from a wide spectrum of underlying conditions. The causes of CKD are diverse and vary across regions, populations, and age groups. Determining the underlying etiology is essential because it guides therapeutic choices, informs prognosis, and aligns with the KDIGO 2024 “C-G-A” classification, which emphasizes cause (C) as a primary component of CKD staging.1
Diabetes mellitus is the leading etiology, accounting for 30–50% of all CKD cases worldwide.1 Hypertension is the second most common, followed by glomerular diseases such as IgA nephropathy and focal segmental glomerulosclerosis, hereditary kidney diseases including autosomal dominant polycystic kidney disease, and tubulointerstitial diseases from nephrotoxins or obstruction.1 Additional contributors include cardiovascular disease, repeated episodes of acute kidney injury (AKI), and environmental exposures. CKD etiology should be identified whenever possible, as it influences monitoring strategies, treatment decisions, and prognosis.1
Sociodemographic factors, such as advanced age, lower income, limited healthcare access, and structural inequities, further increase CKD risk and contribute to disparities in disease detection and outcomes.1 Environmental and occupational exposures, including heat stress, heavy metals (e.g., cadmium, lead), and agricultural toxins, have also emerged as significant causes in certain regions across the globe.1
Healthcare team members should be familiar with the causes and risk factors of CKD. Accurately determining the cause is vital for selecting treatment modalities.2 These are summarized in Table 1 and discussed in detail below.2
Table 1
CKD Risk Factors2
| Clinical Risk Factors |
|---|
| Diabetes |
| Hypertension |
| Autoimmune diseases |
| Systemic infections (e.g., HIV, hepatitis B virus, hepatitis C virus) |
| Nephrotoxic medications (e.g., nonsteroidal anti-inflammatory drugs, herbal remedies, lithium) |
| Recurrent urinary tract infections |
| Kidney stones |
| Urinary tract obstruction |
| Malignancy |
| Obesity |
| Reduced kidney mass (e.g., nephrectomy, low birth weight) |
| History of acute kidney injury |
| Smoking |
| Intravenous drug use (e.g., heroin, cocaine) |
| Family history of kidney disease |
| Sociodemographic Risk Factors |
| Age >60 years |
| Nonwhite race |
| Low-income |
| Genetic Risk Factors |
| APOL1 risk alleles |
| Sickle cell trait and disease |
| Polycystic kidney disease |
| Alport syndrome |
| Congenital anomalies of the kidney and urinary tract |
| Other familial causes |
Pathophysiology
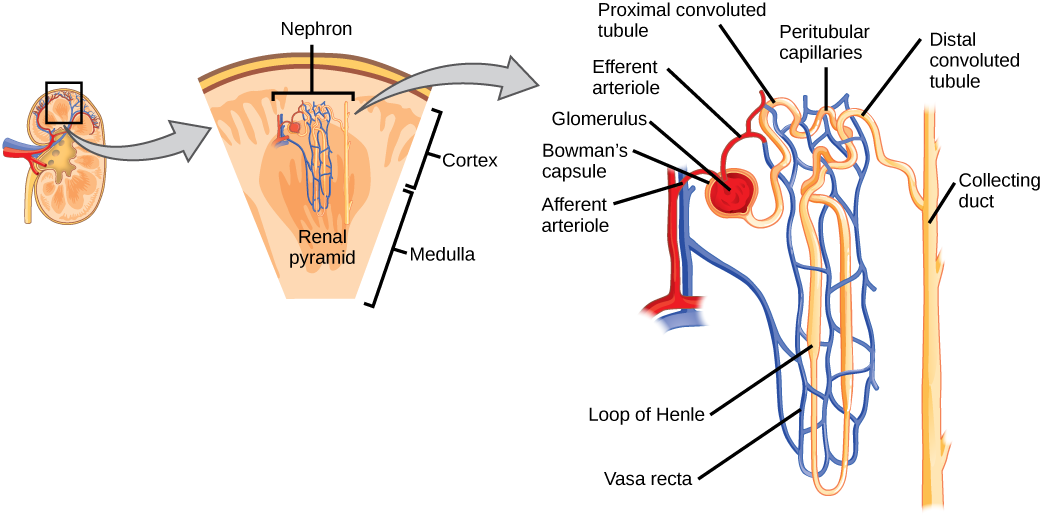
Understanding the pathophysiological mechanisms of CKD is essential for effective management.3 As mentioned above, CKD is a progressive condition characterized by the gradual loss of kidney function.3 Renal fibrosis is a common pathological indicator across various CKD conditions and represents the kidney's attempt to heal itself after chronic injuries, resulting in glomerulosclerosis, tubular atrophy, and interstitial fibrosis.3 The figure below visually depicts a nephron to guide this discussion of CKD pathophysiology.4
Nephron

Glomerulosclerosis is inflammation and damage to the glomerulus.3 This damage is caused by endothelial damage and the proliferation of smooth-muscle and mesangial cells, which are cells responsible for the glomerular injury response.3 Simply explained, glomerulosclerosis is sclerosis (hardening/scarring) of the glomerulus, which is the initial filtering portion of the nephron.3 Factors like hypertension, dyslipidemia, and smoking increase the risk of progressive glomerulosclerosis.3 Inflammatory responses, initiated by activated endothelial cells in response to hypertension, lead to mesangial cell proliferation. Eventually, mesangial expansion occurs, which is an early sign of glomerulosclerosis.3
Glomerular filtration rate and proteinuria are strongly related to tubular atrophy, interstitial fibrosis, and scarring.3 Tubular epithelial cells produce inflammatory substances and attract inflammatory cells into the renal interstitium.3 This process triggers interactions with interstitial myofibroblasts.3 Injured tubular epithelial cells lose their ability to regenerate as fibrosis worsens, which leads to tubular atrophy and either dysfunctional or non-functional glomeruli.3
Additionally, the kidneys undergo changes in interstitial capillary permeability in CKD, allowing plasma proteins to enter the renal interstitium and triggering inflammation.3 Reduced interstitial capillary surface area leads to kidney hypoxia, affecting collagen degradation, which is essential in healthy kidneys.3 Deposition of collagens, basement membrane proteins, proteoglycans, and glycoproteins occurs in the damaged kidney. The extent of fibrotic interstitium correlates with renal function and long-term prognosis.3
Defining Chronic Kidney Disease
Chronic kidney disease is defined as abnormalities of kidney structure or function lasting three months or longer that have implications for health.1 CKD is common among adults, especially individuals with diabetes, hypertension, obesity, and cardiovascular disease. Chronic kidney disease is associated with substantial morbidity, mortality, and healthcare utilization.1
The KDIGO 2024 guideline retains the core definition but emphasizes three key components of CKD assessment:1
Cause (C)
GFR category (G)
Albuminuria category (A)
This expanded “C-G-A” classification helps clinicians better stratify disease severity, risk of progression, and need for referral.1 Chronic kidney disease is diagnosed when one or more of the following are present for ≥3 months:1
Estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m²
Albuminuria ≥30 mg per 24 hours or urine albumin–creatinine ratio (ACR) ≥30 mg/g
Urine sediment abnormalities (e.g., hematuria of glomerular origin)
Electrolyte or tubular disorders
Structural abnormalities detected by imaging
History of kidney transplantation
GFR Categories (G1–G5)
Glomerular filtration rate categories (G1–G5) reflect overall kidney function and are central to CKD staging.1
G1: ≥90 mL/min/1.73 m² (normal/high)
G2: 60–89 mL/min/1.73 m² (mildly decreased)
G3a: 45–59 mL/min/1.73 m² (mildly to moderately decreased)
G3b: 30–44 mL/min/1.73 m² (moderately to severely decreased)
G4: 15–29 mL/min/1.73 m² (severely decreased)
G5: <15 mL/min/1.73 m² (kidney failure)
Patients in G1 or G2 only meet CKD criteria when another marker of kidney damage is present (e.g., albuminuria, hematuria, structural abnormalities).1
Albuminuria Categories (A1–A3)
Albuminuria is a strong predictor of kidney disease progression and cardiovascular risk. Albuminuria categories are as follows:1
A1: <30 mg/g (normal–mildly increased)
A2: 30–300 mg/g (moderately increased)
A3: >300 mg/g (severely increased)
Both GFR and albuminuria are assessed together to predict progression risk and determine monitoring frequency.1
Active Learning Activity
Review each case below and classify the following:
CKD GFR category (G1–G5)
CKD albuminuria category (A1–A3)
KDIGO heat-map risk level (low, moderately increased, high, very high)
Case 1
A 54-year-old woman with hypertension.
eGFR: 78 mL/min/1.73 m²
UACR: 65 mg/g
BP: 142/84
Meds: amlodipine
Case 2
A 69-year-old man with Type 2 Diabetes Mellitus (T2DM).
eGFR: 42 mL/min/1.73 m²
UACR: 520 mg/g
A1c: 7.8%
Meds: metformin
Case 3
A 74-year-old woman with heart failure and obesity.
eGFR: 28 mL/min/1.73 m²
UACR: 18 mg/g
BP: 128/70
Meds: carvedilol, furosemide
Clinical Presentation
Chronic kidney disease may progress silently in the early stages.3 Many patients with CKD remain asymptomatic until the disease has advanced significantly, or it is uncovered through routine laboratory testing.3 As CKD progresses, patients may develop non-specific symptoms that may be overlooked or attributed to other medical conditions.3 These can include fatigue, weakness, poor appetite, and weight loss.2 As uremic retention products accumulate in the body, patients can experience signs and symptoms within most organ systems.3 These are detailed in Table 2.3
Table 2
Signs and Symptoms of CKD3
| Sign/Symptom | Description |
|---|---|
| Appearance | Pallor secondary to anemia |
| Hypertension | Primary or secondary affect |
| Shortness of breath | Due to fluid overload, anemia, or cardiomyopathy |
| Kidney issues | Kidney abnormalities are dependent on the cause |
| Itching and cramps | Itching due to deregulation of the immune response; cramps caused by neuronal irritation |
| Cognitive changes | Language and attention are affected in particular |
| Gastrointestinal symptoms | Anorexia, vomiting, taste disturbance |
| Change in urine output | Polyuria; oliguria; nocturia; anuria |
| Hematuria | Results from immune injury to glomeruli |
| Proteinuria | Due to tubular damage |
| Peripheral edema | Due to sodium retention or nephrotic syndrome |
Diagnosis
Clinical Evaluation
Early diagnosis of CKD improves long-term outcomes and reduces cardiovascular and renal complications. A comprehensive clinical evaluation should begin with a detailed history, with attention to risk factors such as diabetes, hypertension, cardiovascular disease, nephrotoxin exposure, family history of kidney disease, and prior acute kidney injury.3 Physical examination may reveal hypertension, volume overload (e.g., edema, elevated jugular venous pressure), anemia-related pallor, or signs of underlying systemic disease (e.g., rash, vasculitic lesions).3
Guidelines for CKD Screening
Current guidelines recommend screening for CKD in the following cohorts.1
Adults ≥60 years,
Patients with diabetes or hypertension,
Individuals with cardiovascular disease,
Patients with a history of AKI,
Individuals with a family history of kidney disease, and
High-risk populations, including those with APOL1 risk alleles
KDIGO 2024 continues to emphasize that early and accurate classification requires both assessment of kidney function (eGFR) and markers of kidney damage (primarily albuminuria).1
KDIGO recommends targeted testing and not universal screening in individuals with risk factors, including diabetes, hypertension, CVD, family history of kidney disease, autoimmune diseases, or prior AKI episodes.1 The two essential tests for detecting CKD are:
Serum creatinine to estimate GFR (eGFR)
Urine albumin-creatinine ratio (UACR)
Both markers should be measured at least twice over a period of ≥3 months to confirm chronicity.1 Additional laboratory or imaging tests may be needed to identify etiology or evaluate complications.1 In individuals with abnormal testing, risk stratification should follow the KDIGO GFR (G) and albuminuria (A) categories to guide monitoring and management.1
Table 3
Diagnostic Tests for CKD1
| Test | Purpose / Description | Clinical Notes & Practice Points |
|---|---|---|
| Estimated GFR (eGFR) |
|
|
| Urine Albumin-Creatinine Ratio (UACR) |
|
|
| Imaging |
|
|
| Kidney Biopsy |
|
|
Management of Chronic Kidney Disease
Effective management of chronic kidney disease focuses on slowing disease progression, optimizing cardiovascular health, alleviating symptoms, and preventing or treating complications. Modern management emphasizes a comprehensive, multidisciplinary approach that incorporates lifestyle changes, pharmacotherapy, and proactive monitoring.
Lifestyle Changes
Lifestyle modification is a cornerstone of CKD management and remains essential across all stages of the disease.1 Nutrition plays a particularly important role. KDIGO recommends a dietary protein intake of approximately 0.8 g/kg/day for most adults with CKD, while lower-protein diets in the range of 0.55–0.60 g/kg/day may be considered for individuals at high risk of progression who can successfully adhere to the intervention.1 Sodium restriction to less than 2 g per day is beneficial for blood pressure control and for reducing proteinuria.1 Additional lifestyle measures, including regular physical activity, achieving or maintaining a healthy weight, smoking cessation, moderating alcohol consumption, and avoiding NSAIDs or other nephrotoxic substances, are strongly encouraged.1 Collaboration with a renal dietitian has been shown to improve self-management, promote adherence to dietary recommendations, and foster overall health literacy related to CKD.1
Reducing Cardiovascular Risk in CKD
Cardiovascular risk management remains central to CKD care, as cardiovascular disease is the leading cause of death in this population.1 Treatment strategies typically include optimizing blood pressure control, with RAS inhibition preferred when albuminuria is present, alongside lipid-lowering therapy with statins, individualized antiplatelet therapy, appropriate glycemic management using agents such as SGLT2 inhibitors, GLP-1 receptor agonists, and metformin when suitable, and continued emphasis on lifestyle interventions.1 RAS inhibitors, including ACE inhibitors and ARBs, form a foundational (first-line) therapy for albuminuric CKD.1 KDIGO guidance emphasizes titrating these medications to maximally tolerated doses because clinical trials demonstrating benefit used full therapeutic dosages.1 Following initiation, blood pressure, serum creatinine, and potassium should be reassessed within two to four weeks.1 Hyperkalemia should be managed proactively, and RAS inhibition should not be discontinued unless absolutely necessary.1
Continuation is recommended unless serum creatinine rises more than 30% within four weeks.1 Discontinuation should be reserved for patients with symptomatic hypotension, uncontrolled hyperkalemia, or those with uremic symptoms at very low eGFR levels. Avoiding premature discontinuation preserves substantial renal and cardiovascular benefit.1
In November 2024, the FDA added a new class-wide warning for all GLP-1 receptor agonists regarding the increased risk of pulmonary aspiration during procedures requiring deep sedation or general anesthesia.5 This risk is thought to stem from delayed gastric emptying associated with GLP-1 RAs, which may increase residual gastric volume despite routine fasting.5 Current recommendations include holding daily GLP-1 RAs on the day of surgery and withholding weekly formulations for 7 days prior to sedation. Clinicians should assess aspiration risk preoperatively and collaborate closely with anesthesia teams when caring for patients receiving GLP-1 RA therapy.
SGLT-2 Inhibitors
SGLT2 inhibitors have transformed the landscape of CKD therapy. Initially developed for glycemic control, they demonstrated significant reductions in cardiovascular death and heart failure hospitalization, along with notable secondary benefits on kidney disease progression.6 Their kidney-protective actions stem from restoration of tubuloglomerular feedback, which lowers intraglomerular pressure, reduction of inflammation, modest blood pressure lowering, improvements in metabolic parameters, and reductions in albuminuria.6
Several landmark trials established their benefits.6 In the CREDENCE trial, canagliflozin resulted in a 30% reduction in a composite kidney outcome among patients with type 2 diabetes and CKD.7 DAPA-CKD demonstrated a 39% reduction in kidney disease progression or death, regardless of diabetes status.8 EMPA-KIDNEY further showed that empagliflozin reduced the risk of CKD progression or cardiovascular death by 28%.9 Current KDIGO recommendations support the use of SGLT2 inhibitors in individuals with type 2 diabetes and CKD with an eGFR above 20 mL/min/1.73 m², as well as in those without diabetes when UACR is at least 200 mg/g or in the presence of heart failure.1 They should generally be continued even when eGFR falls below 20, unless contraindications develop.1
GLP-1 Receptor Agonists
GLP-1 receptor agonists also provide important benefits in CKD, not only by improving glycemic control and promoting weight loss but also through cardiovascular and emerging renal effects.6 Their kidney-protective mechanisms are thought to involve reduced inflammation, improved metabolic control, and favorable cardiovascular changes.6 In FLOW-CKD, semaglutide reduced the primary composite kidney outcome by 24% in individuals with type 2 diabetes and CKD, though this effect was not observed in participants already receiving SGLT2 inhibitors.10 Additional evidence from SUSTAIN, PIONEER, LEADER, and AWARD-7 consistently showed that GLP-1 receptor agonists slow eGFR decline, reduce albuminuria, and limit progression to macroalbuminuria.5
Tirzepatide, evaluated in SURPASS-4, was associated with a slower decline in eGFR and a reduced incidence of kidney outcomes compared to insulin.11 GLP-1 receptor agonists are therefore recommended for individuals with type 2 diabetes and CKD who are not meeting glycemic targets despite metformin and SGLT2 inhibitor therapy, or for those who cannot use these first-line agents.6
Finerenone
Finerenone, a selective non-steroidal mineralocorticoid receptor antagonist, has emerged as a valuable therapeutic option for patients with CKD and type 2 diabetes.6 By reducing inflammation and fibrosis within both cardiac and renal tissues, finerenone produced clinically meaningful renal benefits in the FIDELIO-DKD and FIGARO-DKD trials.6 Across these studies, finerenone reduced major kidney outcomes by approximately 18%, with particularly strong effects observed in those with high levels of albuminuria.6 These findings were reinforced by pooled analyses. Hyperkalemia remains the principal safety concern and necessitates careful monitoring after therapy initiation.6 Finerenone is recommended for patients with type 2 diabetes, an eGFR of at least 25 mL/min/1.73 m², a UACR of at least 30 mg/g, and a baseline serum potassium level below 5.0 mEq/L.1
Sacubitril/valsartan
Sacubitril/valsartan offers dual angiotensin receptor blockade and neprilysin inhibition and is widely used in heart failure management.6 Its renal effects are mixed. In PARAGON-HF, sacubitril/valsartan significantly reduced renal composite outcomes in individuals with HFpEF.12 In contrast, PARADIGM-HF showed no significant effect on major kidney outcomes when compared to enalapril.13 Although not considered a dedicated kidney-protective therapy, sacubitril/valsartan may provide renal benefits in select heart failure populations while offering well-established cardiovascular advantages.6
Medication Considerations
Pharmacists can assist the care team in identifying nephrotoxins and counseling patients to avoid medications deemed nephrotoxic, meaning they can harm the kidneys. There are numerous medications considered nephrotoxins. Some of these include the following.3
Non-steroidal Anti-Inflammatory Drugs (NSAIDs): NSAIDs should be avoided in CKD, especially if the patient is also taking ACE inhibitors (ACE-I) or Angiotensin Receptor Blockers (ARB) therapy.3
Herbal products: Herbal medications are particularly concerning because they are not regulated by the Food and Drug Administration (FDA). Some products, such as those containing aristolochic acid or anthraquinones, can lead to serious issues, including acute tubular necrosis and nephrolithiasis.3
Phosphate-based bowel preparations: These preparations, including both oral and enema forms, can cause acute phosphate nephropathy.3
Proton pump inhibitors (PPIs): Proton pump inhibitors have been linked to acute interstitial nephritis and CKD in some cases.3 It is important for healthcare providers to work with patients to determine if their need for continued PPI use is warranted during primary care visits.
In addition to avoiding nephrotoxic medications, clinicians should ensure that every medication taken is dose-adjusted for renal function, if necessary. Several commonly prescribed medications, including antibiotics, direct oral anticoagulants, gabapentin, pregabalin, oral hypoglycemic agents, insulin, chemotherapeutic drugs, and opiates, often need dose reductions in CKD patients to prevent adverse drug events.3
It is advisable to limit the use of medications with low expected benefits in CKD patients due to their increased risk of side effects. Gadolinium-based contrast agents should be avoided in individuals with acute kidney injury, eGFR less than 30 mL/min/1.73 m2, or end-stage kidney disease due to the risk of nephrogenic systemic fibrosis, a painful condition causing skin and organ fibrosis.8 Newer formulations of gadolinium are less likely to cause this condition, but it's best to avoid gadolinium when possible.3 If necessary, patients should be informed about the potential risk, and consultation with a nephrologist for postexposure hemodialysis may be considered.
Managing CKD Complications
Management of CKD complications requires ongoing laboratory assessment and individualized therapy.1 Anemia evaluation involves monitoring hemoglobin, ferritin, and transferrin saturation, with treatment typically including iron supplementation and, when indicated, erythropoiesis-stimulating agents.1 For CKD-mineral and bone disorder, calcium, phosphorus, and parathyroid hormone levels should be routinely assessed, with therapy tailored using phosphate binders, vitamin D analogs, or calcimimetics.1 Electrolyte disturbances such as metabolic acidosis, hyperkalemia, and hyponatremia are common and require targeted interventions to prevent clinical deterioration.1
Monitoring CKD
Per KDIGO, eGFR, and albuminuria should be monitored at least once annually.1 High-risk patients should be monitored twice per year or more.8 Very high-risk patients should be monitored at least 3 times per year.8 An individualized approach to CKD is recommended. Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus and should be avoided in pregnancy. If a pharmacy technician notices a prescription or over-the-counter purchase of prenatal vitamins with an ACE inhibitor or ARB prescription, the pharmacist should be notified. CKD is complex, and an unmet medical need to optimize outcomes remains. In a non-diabetic African American population with a GFR of 20–65 mL/ min/1.73 m2 randomized to control BP with follow-up of 3+ years, only patients with baseline proteinuria>1 g/day demonstrated slowing of CKD with intensive blood pressure control.1
A Collaborative Care Approach
Pause and Ponder:
How can your clinic better incorporate dietitians, pharmacists, or telehealth tools to support self-management?
Effective CKD care relies heavily on coordinated, multidisciplinary management.1 Nephrologists, primary care clinicians, pharmacists, renal dietitians, social workers, and mental health professionals each contribute essential expertise that improves outcomes, enhances medication safety, and supports patient self-management.1 Education programs for CKD should address foundational knowledge of the disease, management strategies, and available kidney failure treatment options.1 Materials must be culturally appropriate, written in plain language, and delivered through a multidisciplinary approach. Including caregivers in the educational process improves adherence and shared decision-making.1
Shared decision-making is essential when implementing kidney-protective pharmacotherapy, especially given the increasing number of effective options. Discussions should address the following:
Clinical benefits: slowing CKD progression, reducing cardiovascular risk, and lowering albuminuria.
Risks and monitoring: transient eGFR changes with SGLT2 inhibitors, GI symptoms with GLP-1 RAs, hyperkalemia risk with finerenone, and the rare risk of euglycemic DKA.
Treatment priorities: ensuring that guideline-preferred sequencing aligns with patient-specific comorbidities.
Cost and access: insurance coverage, affordability, prior authorizations, and generics vs brand-only therapies.
Patient values: route of administration (oral vs. injectable), weight goals, glucose control needs, and willingness to follow up with labs.
Engaging patients in selecting therapies improves adherence, satisfaction, and long-term clinical outcomes.
Telehealth has become an increasingly important component of CKD management. Remote monitoring tools enable patients to track blood pressure, weight, and symptoms, while virtual visits and educational modules enhance continuity of care between in-person appointments.1 Telehealth facilitates timely medication adjustments, early detection of complications, and broader access to subspecialty care, particularly for individuals in rural or underserved areas.1
Summary
Chronic kidney disease is an increasingly prevalent condition that poses significant challenges for patients and healthcare providers. The growing burden of CKD underscores the urgency of equipping healthcare professionals with the most up-to-date knowledge and strategies for effectively managing this condition. Recent advancements within nephrology and a growing body of knowledge have provided valuable insights into the early detection, risk stratification, and therapeutic interventions for CKD. Pharmacists can best care for their patients by having a comprehensive understanding of CKD, including its underlying causes, diagnostic approaches, and treatment options. Pharmacy technicians may perform medication reconciliation and medication management services.
References
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.
Grams ME, Chow EK, Segev DL, Coresh J. Lifetime incidence of CKD stages 3–5 in the United States. Am J Kidney Dis. 2013;62(2):245–252. doi:10.1053/j.ajkd.2013.03.009
Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389(10075):1238-1252. doi:10.1016/S0140-6736(16)32064-5
WikiCommons. Nephron. Accessed January 20, 2026. https://commons.wikimedia.org/wiki/Category:Nephron#/media/File:Figure_41_03_03.png
Gallagher A. FDA Adds Delayed Gastric Emptying as Adverse Event on Semaglutide Label. November 14, 2024. Accessed January 20, 2026. https://www.pharmacytimes.com/view/fda-adds-delayed-gastric-emptying-as-adverse-event-on-semaglutide-label
Ammar A, Edwin SB, Whitney R, Lipari M, Giuliano C. Updates in chronic kidney disease management: A systematic review. Pharmacotherapy. 2025; doi:10.1002/phar.70014
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi:10.1056/NEJMoa1811744
Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–1446. doi:10.1056/NEJMoa2024816
The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117–127. doi:10.1056/NEJMoa2204233
Mann JFE, Husain M, Idorn T, et al. Semaglutide and renal outcomes in patients with type 2 diabetes and chronic kidney disease (FLOW). N Engl J Med. 2024;390:xxx–xxx.
Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4). Lancet. 2021;398(10313):1811–1824. doi:10.1016/S0140-6736(21)02188-7
Solomon SD, McMurray JJV, Anand IS, et al. Angiotensin–neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381(17):1609–1620. doi:10.1056/NEJMoa1908655
McMurray JJV, Packer M, Desai AS, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
DISCLAIMER
The information provided in this course is general in nature, and it is designed solely to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals must consult their employer, healthcare facility, hospital, or other organization for guidelines, protocols, and procedures to follow. The information provided in this course does not replace those guidelines, protocols, and procedures, but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses is constantly changing. Any person taking this course understands that such a person must make an independent review of medication information before any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course or course material.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
RxCe.com
© RxCe.com LLC 2025: All rights reserved.