CLASSIFICATION AND DIAGNOSIS OF DIABETES MELLITUS
Faculty:
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson is an Associate Professor of Internal Medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson, PharmD, BCPS, is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy, where she is course director of the Parenteral Products and Basic Pharmaceutics Lab courses.
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and licensed pharmacist. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Abstract
Diabetes mellitus remains a major public health problem as a leading cause of death and micro- and macro-vascular morbidity. The management of diabetes continues to evolve as new research, technology, and treatments allow for enhanced patient care. It is vital for healthcare providers, including physicians, nurses, and pharmacists, to remain up to date with the newest diabetes care guidelines, which now incorporate inclusive language and a patient-first approach. This includes a strong understanding of both the classification and diagnosis of diabetes. This course will review the pathophysiology, classification, and diagnosis of diabetes mellitus in the context of the updated Standards of Care in Diabetes 2023 guidelines.
Accreditation Statements
In support of improving patient care, RxCe.com LLC is jointly accredited by the Accreditation CouncilTM for Continuing Medical Education (ACCME®), the Accreditation Council for Pharmacy Education (ACPE®), and the American Nurses Credentialing Center (ANCC®), to provide continuing education for the healthcare team.


This activity was planned by and for the healthcare team, and learners will receive 2 Interprofessional Continuing Education (IPCE) credits for learning and change.
Joint Universal Activity Number: The Joint Accreditation Universal Activity Numbers assigned to this activity are as follows:
Pharmacists: JA4008424-0000-26-043-H01-P
Pharmacy Technicians: JA4008424-0000-26-043-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit.
Credit Types:
IPCE Credits - 2 Credits
AAPA Category 1 Credit™️ - 2 Credits
AMA PRA Category 1 Credit™️ - 2 Credits
Pharmacy - 2 Credits
Type of Activity: Application
Media: Computer-Based Training (i.e., online courses)
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Activity Pre-Test, Post-Test, and Activity Evaluation.
Release Date: April 3, 2026 Expiration Date: April 3, 2029
Target Audience: This educational activity is for Physicians, Physician Assistants, Pharmacists, and Pharmacy Technicians
How to Earn Credit: From April 3, 2026, through April 3, 2029, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Take the “Educational Activity Pre-Test;”
Study the section entitled “Educational Activity;” and
Complete the Educational Activity Post-Test and Activity Evaluation. The Educational Activity Post-Test will be graded automatically. Following successful completion of the Educational Activity Post-Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
CME Credit: Credit for this course will be uploaded to CPE Monitor® for pharmacists. Physicians may receive AMA PRA Category 1 Credit™️ and use these credits toward Maintenance of Certification (MOC) requirements. Physician Assistants may earn AAPA Category 1 CME credit, reportable through PA Portfolio. All learners shall verify their individual licensing board’s specific requirements and eligibility criteria.
Statement of Need
Diabetes mellitus remains a prevalent, costly, and progressive chronic disease associated with substantial morbidity and mortality. Early identification and accurate classification are essential in preventing complications. Healthcare professionals must understand the underlying pathophysiology of diabetes, distinguish among the disease's categories, and apply appropriate diagnostic tests. Practice gaps persist in recognizing mechanisms of insulin deficiency and insulin resistance. Differentiating type 1, type 2, gestational, and other forms of diabetes is important. Approaches to selecting and interpreting fasting plasma glucose, oral glucose tolerance, random plasma glucose, and hemoglobin A1c results vary. Misclassification or delayed diagnosis can lead to missed opportunities for timely treatment, patient education, and prevention of complications. This activity aims to address these gaps by strengthening knowledge and improving confidence in the classification and diagnosis of diabetes mellitus aligned with current standards of care.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Describe the pathophysiology of diabetes mellitus
Compare and contrast categories of diabetes mellitus
Describe tests used to diagnose diabetes
Disclosures
The following individuals were involved in planning, developing, and/or authoring this activity: L. Austin Fredrickson, MD, FACP; Liz Fredrickson, PharmD, BCPS; and Pamela Sardo, PharmD, BS. None of the individuals involved in developing this activity has a conflict of interest or financial relationships related to the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity Pre-Test
Which of the following correctly describes Type 2 diabetes (T2DM)?
It is due to autoimmune β-cell destruction, usually leading to absolute insulin deficiency
It is due to a non-autoimmune progressive loss of adequate β-cell insulin secretion, frequently on the background of insulin resistance and metabolic syndrome
It is diabetes diagnosed in the second or third trimester of pregnancy that was not clearly overt diabetes prior to gestation
It is due to drugs or chemicals that induce diabetes
Which criteria does the American Diabetes Association cite as diagnostic for diabetes?
FPG ≥70 mg/dL
A1c ≥ 5.7%
Random plasma glucose >200 mg/dL in a patient with classic symptoms of hyperglycemia or a hyperglycemic crisis
Random plasma glucose >100 mg/dL
Patients with a BMI indicating overweight or obesity should be considered for testing for prediabetes or T2DM if they have
hyperthyroidism.
hypothyroidism.
hypertension.
hypotension.
Educational Activity
Classifications and Diagnosis of Diabetes
Introduction
Diabetes mellitus is a global epidemic. It afflicts an increasing number of people each year. Early diagnosis and treatment of diabetes are crucial for reducing the risk of complications and improving overall health outcomes for populations and individual patients. It is vital for healthcare providers, including physicians, nurses, and pharmacists, to remain up to date with the newest diabetes care guidelines, which now incorporate inclusive language and a patient-first approach. This includes a firm understanding of the classification and diagnosis of diabetes. This course will review the pathophysiology, prevalence, classification, and diagnosis of diabetes mellitus in the context of the updated Standards of Care in Diabetes 2023 guidelines.
Prevalence and Etiology of Diabetes
Diabetes mellitus is a global epidemic affecting millions of people worldwide, with a prevalence that continues to increase yearly.1 Diabetes is a chronic disease that affects the body's ability to either produce or respond to insulin, resulting in hyperglycemia or high levels of glucose in the blood.1,2 Long-term hyperglycemia is a leading cause of cardiovascular disease, kidney failure, blindness, and lower limb amputations.2,3 Early diagnosis and treatment of diabetes are crucial in reducing the risk of developing complications and improving overall health outcomes in populations and individual patients.1,5
The prevalence of diabetes varies among countries.6 In general, low- and middle-income countries experience a more significant increase in diabetes prevalence than high-income countries.6
In the United States (US), an estimated 29.1 million people are diagnosed with diabetes.7 This represents approximately 12% of the population.7 Centers for Disease Control and Prevention (CDC) data list diabetes as the seventh leading cause of death in the US.8
The prevalence of diagnosed diabetes does not differ greatly between men and women.7 However, the percentage of adults with diabetes does increase with age.7 Rates of diabetes also differ by race and ethnicity. This data is presented in Table 1.7
Table 1
Diabetes by Race or Ethnicity7
| Race/ethnicity | Percentage |
|---|---|
| American Indian or Alaska Native, non-Hispanic | 16% |
| Black, non-Hispanic | 12.5% |
| Native Hawaiian or Other Pacific Islander, non-Hispanic | 11.7% |
| Asian, non-Hispanic | 9.2% |
| Hispanic | 10.3% |
| White, non-Hispanic | 8.5% |
The CDC estimates that 27.6% of diabetes cases are undiagnosed, and undiagnosed diabetes affects 4% of US adults.3 However, a 2022 study reviewed the trends of undiagnosed diabetes using definitions more consistent with those in clinical practice.3 They found the proportion of undiagnosed diabetes cases declined between 1988 and 2020 due to improvements in detection, and estimated undiagnosed diabetes affects 1-2% of adults in the US.3 The authors did note that undiagnosed diabetes is higher in specific subpopulations, including among Asian Americans, those who are overweight or obese, and those with low income or who are uninsured.3
In the US, Type 1 diabetes mellitus (T1DM) accounts for approximately 6.1% of all cases,7 and worldwide, these cases continue to increase for unknown reasons.1 Type 2 diabetes mellitus (T2DM), the most common form of the disease, accounts for about 93% of all diabetes cases in the US, with a prevalence in US adults of approximately 12%.7 The increase in cases of T2DM parallels the rise in obesity cases throughout the US.1
Prediabetes is a condition in which blood glucose levels are not high enough to meet the diagnostic criteria of diabetes.1 Prediabetes is common, with over a third of US adults having prediabetes. Eight out of 10 patients with prediabetes are unaware they have it.9
Another form of diabetes, gestational diabetes mellitus or GDM, has also seen an increased prevalence.1,10 It is estimated to occur in 5 to 9% ~10% of pregnancies,10 and up to 50% of women who develop GDM will later develop T2DM.11,12
There are several other, less common, types of DM. They include maturity-onset diabetes of the young (MODY) and neonatal diabetes.1
Ethnic Disparities in Diabetes Prevalence
Several racial and ethnic disparities in diabetes exist.13 Racial and ethnic minority groups have higher rates of diabetes compared to the general population, and this disparity may be attributed to several factors, including genetic predisposition, cultural differences, socioeconomic status, and healthcare access.13 Minority populations often face challenges in accessing healthcare services, receiving timely diagnoses, and adhering to their treatment regimens. This can lead to poorer diabetes control, an increased risk of complications, and higher mortality rates.13 It is crucial for clinicians to understand the importance of recognizing and addressing these disparities to promote and achieve health equity and optimize the care of all patients.13
Prevalence and Public Health Impact
In the US, the public health impact of diabetes is significant, considering both the large economic burden and the negative impact on morbidity and mortality. Addressing the diabetes epidemic requires a multifaceted approach that includes prevention efforts, effective management of the disease, and addressing the disparities in diabetes prevalence and outcomes among different populations. Healthcare providers across many disciplines, including physicians, pharmacists, and nurses, play a crucial role in managing diabetes by working collaboratively to provide patient education, counseling, and medication management. Additionally, healthcare professionals can work with community organizations to develop and implement diabetes prevention and management programs that address the unique needs of the diverse populations that they serve.
Economic Burden
Diabetes has a significant economic impact on the healthcare system and individuals with the disease. In 2022, the estimated cost of diagnosed diabetes in the United States was $412.9 billion, including $306.6 billion in direct medical costs and $106.3 billion in reduced productivity due to illness-related absenteeism and presenteeism.14 Individuals with diabetes have medical expenses that are approximately 2.3 times higher than those without diabetes, and the cost of managing the disease increases as complications develop.14 The financial burden of diabetes also extends to families, who may experience reduced income due to the need for caregivers to aid family members with diabetes, as well as treat the subsequent comorbidities that stem from the disease.14
Pathophysiology of Diabetes
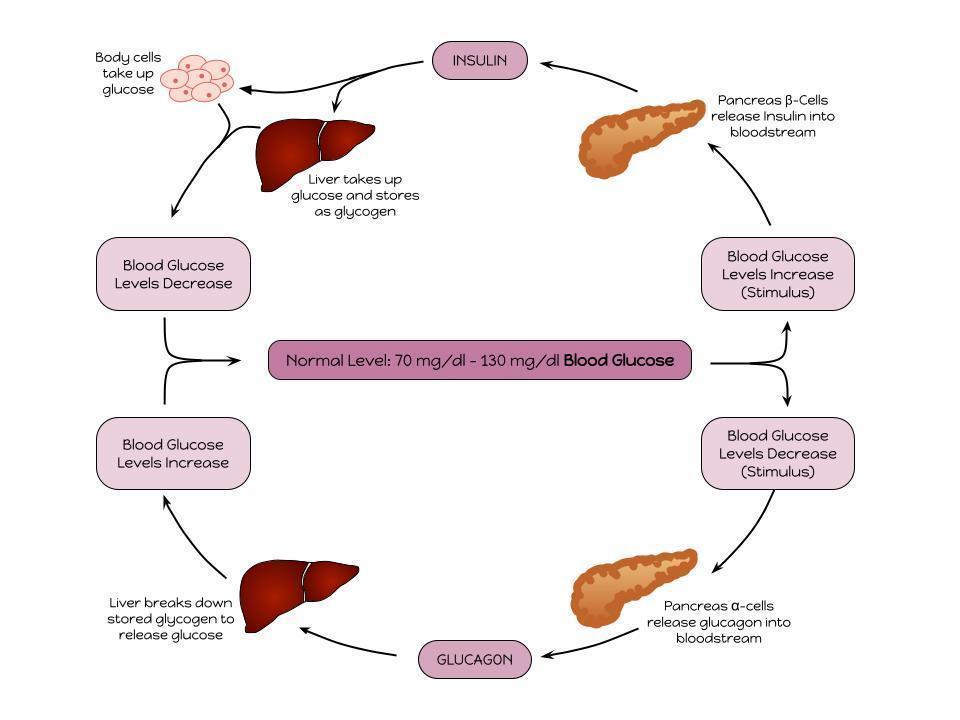
Diabetes is a chronic, heterogeneous metabolic disorder whose underlying etiology involves many different mechanisms.1,2,4,5 The hallmark of diabetes mellitus is hyperglycemia, or elevated plasma glucose levels, resulting from defects in insulin secretion, insulin action, or both.2,4,5 In healthy individuals, the intake of carbohydrates increases blood glucose levels and stimulates incretin hormone release from the gut and insulin release from β-cells in the pancreas.1 High insulin levels then suppress glucose production by the liver, suppress glucagon release, and trigger peripheral tissues to take up glucose.1 Insulin also has an anti-lipolytic effect, which reduces levels of free fatty acids (FFA) in the plasma.1 See the illustration of the interaction between insulin and glucagon in the figure below.15
Insulin and Glucagon
Pathophysiology of Type 1 Diabetes Mellitus
Type 1 diabetes mellitus, historically referred to as insulin-dependent diabetes mellitus (IDDM), is an autoimmune disorder in which the body's immune system attacks and destroys insulin-producing β-cells in the pancreas.4,5 The IDDM nomenclature has been updated to T1DM, as patients with T2DM may also depend on insulin but have different underlying pathophysiology and consequences to undertreatment. The destruction of β-cells in T1DM results in an absolute deficiency of insulin, which is required to transport glucose from the bloodstream into cells for energy production.4,5 Without sufficient insulin, glucose accumulates in the bloodstream, leading to hyperglycemia.4,5 The pathogenesis of T1DM involves genetic and environmental factors, with a strong association with certain HLA haplotypes.4,5 The onset of T1DM typically occurs in childhood or adolescence, and the disease is often diagnosed based on the presence of hyperglycemia, ketosis, and the presence of autoantibodies against β-cells.4,5
Pathophysiology of Type 2 Diabetes Mellitus
Type 2 diabetes mellitus, also historically known as non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes, is a metabolic disorder characterized by insulin resistance and relative insulin deficiency via β-cell dysfunction.4,5 Like IDDM, the other terms of NIDDM and adult-onset diabetes are outdated, as they are descriptors of conditions and not the underlying disease itself, as patients are now developing T2DM in childhood, or require insulin as described above. In T2DM, Insulin resistance results from disrupted cellular pathways, leading to muscle, liver, and adipose tissue cells becoming less sensitive to insulin.4,5 This insulin resistance ultimately results in decreased glucose uptake and utilization.4,5 A decrease in insulin sensitivity initially causes the β-cells to attempt to compensate by increasing insulin secretion.4,5 Over time, the resulting hyperinsulinemia cannot compensate for decreased insulin sensitivity, and β-cell dysfunction also occurs.4,5 Unlike T1DM, T2DM usually progresses more slowly over time and is typically diagnosed later in life.10 Patients will often remain asymptomatic despite elevated glucose levels, which may contribute to undiagnosed cases.4,5
Pathophysiology of Gestational Diabetes Mellitus (GDM)
GDM is diagnosed either during or right after pregnancy and is the occurrence of glucose intolerance or the development of diabetes during pregnancy.4,5 GDM should not be confused with pre-existing cases of diabetes in patients with diabetes who then become pregnant.4,5 During the late second or third trimester of a pregnancy, blood glucose levels tend to increase. If they reach levels consistent with diabetes, GDM is diagnosed.4,5 Risk factors for GDM include age, obesity, having a previous pregnancy with large babies, and a previous history of GDM.4,5
Person-First Language in Diabetes
Historically, patients with diabetes were referred to as diabetics. Recent guidelines and medical societies have emphasized using language that prioritizes the patient and not the disease.16 By labeling patients as diabetic, much like counterparts of alcoholic, addict, or epileptic, the disease takes precedence in language over the human being seeking medical attention.17 To that end, the current preferred terminology is to describe patients with diabetes exactly that way (a person with diabetes) and not as diabetic, which can be a difficult transition.16
Classifications of Diabetes
According to the American Diabetes Association (ADA) Standards of Care in Diabetes—2023, diabetes is classified into 4 general categories (Table 2).4 The classification system is important for the appropriate diagnosis, management, and prevention of diabetes and its complications.
Table 2
Classification of Diabetes
| 1. Type 1 diabetes (due to autoimmune β-cell destruction, usually leading to absolute insulin deficiency, including latent autoimmune diabetes of adulthood) |
|---|
| 2. Type 2 diabetes (due to a non-autoimmune progressive loss of adequate β-cell insulin secretion, frequently on the background of insulin resistance and metabolic syndrome) |
| 3. Specific types of diabetes due to other causes, e.g., monogenic diabetes syndromes (such as neonatal diabetes and maturity-onset diabetes of the young), diseases of the exocrine pancreas (such as cystic fibrosis and pancreatitis), and drug- or chemical-induced diabetes (such as with glucocorticoid use, in the treatment of HIV/AIDS, or after organ transplantation) |
| 4. Gestational diabetes mellitus (diabetes diagnosed in the second or third trimester of pregnancy that was not clearly overt diabetes prior to gestation) |
The classification of diabetes is important for several reasons. First, it allows for appropriate diagnosis and treatment of the disease. Each type of diabetes has a distinct pathophysiology and requires different approaches to management.4 For example, T1DM requires insulin treatment for survival, whereas T2DM can often be managed initially with lifestyle modifications, oral medications, or newer injectable treatments. Second, classification of diabetes enables accurate estimation of disease prevalence and incidence rates, which are key to public health planning and resource allocation, given the increasing prevalence and impact of this epidemic disease. It is important for clinicians to recognize the complexity of diagnosing diabetes and the risk of misdiagnosis; hyperglycemia occurs in multiple conditions other than diabetes, so a firm understanding of the characteristics of each of the following diagnostic tests is key.4
Diagnostic Testing for Prediabetes and Diabetes Mellitus
Diagnostic Tests
The diagnosis of diabetes is based on the measurement of plasma glucose levels. Per the ADA, there are four diagnostic criteria for diabetes. These include a fasting plasma glucose (FPG) level, an oral glucose tolerance test (OGTT), a random plasma glucose, and a hemoglobin A1c (A1C).4 All three tests are considered equally appropriate as diagnostic screening tools.4 However, detection rates vary for these tests based on the populations and individuals being screened.4 Further, these same screening tests can be used to diagnose prediabetes.
Fasting Plasma Glucose (FPG)
Fasting plasma glucose (FPG) measures the level of glucose in the blood after at least 8 hours without caloric intake.4 The normal range for fasting plasma glucose is between 70 and 99 mg/dL.4 A result of 100 to 125 mg/dL indicates prediabetes, while a result of 126 mg/dL or higher is diagnostic for diabetes.4 Unless the patient has unequivocal hyperglycemia, a diagnosis requires two abnormal FPG tests from either the same sample or two separate test samples.4
The FPG test is reliable and easy to perform, but certain factors can affect its accuracy. For example, stress, illness, medications, and physical activity can all affect blood glucose levels, leading to false results.4 That is why it is important to follow the proper preparation guidelines for the FPG test, which include avoiding food and beverages (except water) for at least 8 hours prior to the test and avoiding strenuous exercise and stressful situations during this time.4
Two-hour Plasma Glucose during Oral Glucose Tolerance Test (OGTT)
The Oral Glucose Tolerance Test (OGTT) is a diagnostic test used to evaluate the body's ability to metabolize glucose. During an OGTT, the patient will fast for at least 8 hours and then ingest a glucose load equivalent to 75 grams of anhydrous glucose dissolved in water.4 Blood glucose levels are then measured two hours after the glucose drink.4 Fasting and carbohydrate restriction have the potential to falsely elevate glucose levels with the OGTT.4 Because of this, it is recommended that patients eat a balanced diet that contains at least 150 grams of carbohydrates for the three days prior to this test.4
The OGTT is generally safe and well-tolerated, but some patients may experience side effects such as nausea, vomiting, and dizziness due to the high glucose load. It is important for patients to follow the fasting requirements before the test to ensure accurate results.
Per the ADA, the concordance between the FPG and the 2h PG test is imperfect. When compared to both the FPG and A1C cut points, the 2-hour plasma glucose test values result in a greater number of prediabetes and diabetes diagnoses.4 If a patient has a discordance between their A1C and glucose values, the 2-hour PG is more accurate.4
Random Plasma Glucose
In patients with classic symptoms of hyperglycemia or experiencing a hyperglycemic crisis, a random plasma glucose level of>200 mg/dL (11.1 mmol/L) can be used to diagnose diabetes.4 Unlike the fasting plasma glucose test and the oral glucose tolerance test, this test does not require the patient to fast prior to the test.4 A random plasma glucose level cannot be used to diagnose prediabetes.4
Hemoglobin A1c (A1C)
A hemoglobin A1c (A1C) level is another way to diagnose diabetes and prediabetes.4 (See Tables 3 and 4 below.) An A1C level provides an overall picture of a patient’s average blood glucose levels over the past 2-3 months.4 An A1C measures the percentage of hemoglobin in the blood that has glucose attached to it.4 Hemoglobin is the protein in red blood cells that carries oxygen throughout the body.4 When glucose levels are high in the blood, some of it attaches to hemoglobin and remains there for the life of the red blood cell, which is approximately 2-3 months.4
Various factors may affect hemoglobin glycation independently of glycemia and, therefore, the interpretation of A1C. These include hemodialysis, pregnancy, HIV treatment, age, race, ethnicity, genetic background, and hemoglobinopathies.4 While A1C can be used to screen children and adolescents for diabetes and prediabetes, the initial studies recommending A1C testing included only adults.4 Additionally, the presence of hemoglobin variants should be considered, as these have the potential to interfere with A1C measurements.4 A1C levels for African American patients who are heterozygous for the hemoglobin variant HbS may have a 0.3% lower A1C when compared to those without the trait.4 The X-linked glucose 6-phosphate dehydrogenase G202A is associated with a ~0.7-0.8% lower A1C. Even without consideration of variants, African American patients may have A1C levels lower than non-Hispanic white patients despite similar fasting and post-prandial glucose levels.4 Finally, the measurement of A1C levels is not as reliable in the following conditions and states: postpartum, HIV treatment with certain protease inhibitors and nucleoside reverse transcriptase inhibitors, and in iron-deficiency anemia.4
Using A1C to diagnose diabetes offers several advantages over the FPG and OGTT. These include patient convenience (fasting is not required), greater preanalytical stability, and fewer day-to-day perturbations during periods of stress, illness, or changes in nutrition.4 However, obtaining an A1C is associated with a higher cost, and A1C testing does have a lower sensitivity at the designated cut point.4 Using a threshold of ≥6.5% (see Table 4 below), the A1C test will diagnose only 30% of diabetes cases collectively using A1C, FPG, or the 2-hour plasma glucose.
Table 3 presents criteria for the diagnosis of prediabetes, and Table 4 presents criteria for the diagnosis of diabetes.4
Table 3
Criteria for the diagnosis of prediabetes*4
| FPG 100 mg/dL (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (IFG) |
|---|
| OR |
| 2-h PG during 75-g OGTT 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0 mmol/L) (IGT) |
| OR |
| A1C 5.7–6.4% (39–47 mmol/mol) |
IFG -impaired fasting glucose
OGTT -oral glucose tolerance test
2 h PG -2 h plasma glucose
*For all 3 tests, the risk is continuous, extending below the lower limit of the range and becoming disproportionately greater at the higher end of the range
Table 4
Criteria for the Diagnosis of Diabetes4
| FPG ≥126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 h.* |
|---|
| OR |
| 2-h PG ≥200 mg/dL (11.1 mmol/L) during OGTT. The test should be performed as described by WHO, using a glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water.* |
| OR |
| A1C ≥6.5% (48 mmol/mol). The test should be performed in a laboratory using a method that is NGSP-certified and standardized to the DCCT assay.* |
| OR |
| Random plasma glucose ≥200 mg/dL (11.1 mmol/L). In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis |
*In the absence of unequivocal hyperglycemia, diagnosis requires 2 abnormal test results from the same results from the same sample or in 2 separate test samples.
2 h PG - 2-hour plasma glucose
DCCT - Diabetes Control and Complications Trial
Per ADA guidelines, the A1C test should be performed using an NGSP-certified method. When the NGSP began in 1996, it was originally called the “National Glycohemoglobin Standardization Program.”4 As this program grew and became international in scope, the official name was shortened to the acronym. The NGSP-certified method utilized should be standardized to the Diabetes Control and Complications Trial (DCCT) reference assay.4 In doing so, missed diagnoses and misdiagnoses can be avoided.4
Screening for and Diagnosing Type 1 Diabetes
Screening for Type 1 Diabetes
Numerous studies suggest that measuring islet autoantibodies in relatives of patients with T1DM can help identify those at risk of developing T1DM.4 One study attempted to ascertain the risk of progressing to T1DM from the time of seroconversion to autoantibody positivity in patients in Finland, Germany, and the United States.4 Five hundred and eighty-five children developed more than two autoantibodies; of those, 70% developed T1DM within ten years, and 84% within fifteen years.4 Overall, the risk of T1DM increases as the number of autoantibodies detected increases.4 Currently, widespread clinical screening of asymptomatic and low-risk individuals is not recommended.4
Diagnosing Type 1 Diabetes
The presentation and diagnosis of T1DM may vary by patient. Historically, children and adolescents presented with diabetes ketoacidosis, and the rates of DKA have increased over the past two decades within the US.4 Some patients may have modestly increased fasting plasma glucose levels that can then rapidly progress to DKA with the occurrence of stress.4 In contrast, some adult patients may retain enough β-cell function to prevent the occurrence of DKA for months and even years.4 Once diagnosed, they may have little to no plasma C-peptide.4
Autoimmune markers associated with T1DM include islet cell autoantibodies and autoantibodies to glutamic acid decarboxylase (GAD65), insulin, tyrosine phosphatases islet antigen (IA-2) and IA-2beta, and zinc transporter 8.4 In Stage 1 of T1DM, patients have at least two of these autoimmune markers present.4
Several genetic factors contribute to β-cell destruction in T1DM, and environmental factors may also play a role. Various syndromes associated with T1DM include the following: immune dysregulation, polyendocrinopathy, enteropathy, and X-linked syndrome.4
Type 1 diabetes mellitus can develop following the use of immunotherapies.4 These types of immune-related adverse events occur in less than one percent of patients on such therapies.4 It is more likely in patients with high-risk HLA-DR4.4
Confirming the Diagnosis
The ADA guidelines state that two abnormal screening test results are necessary to confirm a diagnosis of diabetes unless there is a very clear clinical diagnosis, such as in the case of a hyperglycemic crisis.4 These two results may come from the same sample or two separate test samples.4 If a second test sample is obtained, it is recommended that the second test be performed quickly after the first.4 This second test can be the same as the initial test or a different test.4 If both tests are at or above the diagnostic threshold, for example, an A1C level of 7.0% and 6.8%, a diabetes diagnosis can be confirmed.4 However, if these two tests have conflicting results, the test that is above the diagnostic cutoff should be repeated, and the possibility of A1C assay interference should be considered.4 It is also possible that a test that resulted in an abnormal value (one above the diagnostic threshold) may produce a value below the threshold when repeated.
Screening for and Diagnosing Prediabetes and Type 2 Diabetes
The criteria for screening adults, children, and adolescents for prediabetes are in Tables 5 and 6, respectively.
Table 5
Criteria for Screening Adult Patients for Prediabetes
and Type 2 Diabetes4
| 1. Testing should be considered in adults with overweight or obesity (BMI ≥25 kg/m2 or ≥23 kg/m2 in Asian American individuals) who have one or more of the following risk factors: |
|---|
| • First-degree relative with diabetes |
| • High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander) |
| • History of CVD |
| • Hypertension (≥130/80 mmHg or on therapy for hypertension) |
| • HDL cholesterol level <35 mg/dL (0.90 mmol/L) and/or a triglyceride level >250 mg/dL (2.82 mmol/L) |
| • Individuals with polycystic ovary syndrome |
| • Physical inactivity |
| • Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans) |
| 2. People with prediabetes (A1C ≥5.7% [39 mmol/mol], IGT, or IFG) should be tested yearly. |
| 3. People who were diagnosed with GDM should have lifelong testing at least every 3 years. |
4. For all other people, testing should begin at age 35 years.
|
| 5. If results are normal, testing should be repeated at a minimum of 3-year intervals, with consideration of more frequent testing depending on initial results and risk status. |
| 6. People with HIV |
CVD - cardiovascular disease; GDM- gestational diabetes mellitus
IFG -impaired fasting glucose; IGT -impaired glucose tolerance
Table 6
Criteria for Screening Asymptomatic Pediatric and Adolescent Patients for Prediabetes and Diabetes4
| Screening should be considered in youth* who are overweight (≥85th percentile) or obese (≥95th percentile) and who have one or more additional risk factors based on the strength of their association with diabetes: |
|---|
|
|
|
|
*After the onset of puberty or after 10 years of age, whichever occurs earlier
Prediabetes
The ADA suggests prediabetes should be viewed as a risk factor for progressing to diabetes and cardiovascular disease.4 Prediabetes is associated with hypertension, dyslipidemia (high triglycerides and/or low HDL cholesterol), and obesity.4 Many studies have found a strong association between A1C levels and the subsequent diagnosis of diabetes.3 For example, patients with an A1C between 5.5% and 6.0% had a 5-year incidence between 9% and 25%.4 For those with an A1C between 6.0-6.5%, this 5-year risk is 25% to 50%.4 The ADA has a screening tool for determining the appropriateness of screening for prediabetes.4
Type 2 Diabetes Mellitus
Unlike in T1DM, autoimmune destruction of β-cells does not occur, and DKA rarely occurs.4 Due to the gradual development of hyperglycemia, it may be years before T2DM is properly diagnosed.4 Risk factors for the development of T2DM include age, obesity, and a lack of physical activity. Patients with polycystic ovarian syndrome or a history of gestational diabetes mellitus (GDM) are more likely to develop T2DM.4 If adult patients do not have the traditional risk factors for T2DM, islet autoantibody testing can be done to exclude a T1DM diagnosis.4
Screening Asymptomatic Adults
Healthcare professionals are encouraged to utilize validated screening tools for prediabetes and T2DM. The pre-symptomatic phase prior to the diagnosis of T2DM can be long, and the longer the duration of hyperglycemia, the stronger the risk of adverse outcomes.4 Screening is also beneficial in that identifying prediabetes allows for interventions to prevent the progression of diabetes. In doing so, there is a much lower risk of developing long-term complications such as retinopathy.4 An appropriate screening test interval is not clear. It is currently recommended to screen every three years, as this reduces the number of false-positive tests and allows false-negative tests to be redone before any complications develop.4 Higher-risk individuals may benefit from shorter intervals between screenings.4
Patient Case
A 42-year-old female presents to the primary care clinic with symptoms of fatigue, increased thirst, and urinary frequency over several months. She reports a 9-pound unintentional weight loss. Her body mass index is 31 kg/m2. She informs the physician that her mother and older brother have diabetes. Point-of-care glucose is 238 mg/dL. Her HbA1c is 7.2%.
Patient Case: Pause and Ponder What are the next steps in the appointment? |
|---|
The primary care physician must determine the most likely diagnosis, distinguish it from other forms of diabetes, and confirm it. After the physician shares the findings, the patient asks if they have type 1 or type 2 diabetes.
Patient Case: Pause and Ponder What features suggest possible insulin resistance and T2DM? How would you explain the pathophysiology and classification in plain language to the patient? |
|---|
Patient Counseling
Every patient with diabetes is unique and benefits from an individualized and patient-centered approach. The ADA recommends that all people with diabetes participate in diabetes self-management education.4 Diagnosis is a critical time to evaluate the need for diabetes self-management education and support, which certified diabetes educators can provide. Still, it can also be supported by other health professionals, including pharmacists, pharmacy technicians, physicians, and nurses.4 In addition to learning about diabetes and its management, all healthcare team members can relay several important concepts. Patients can be advised the following:
To ask questions at any time. The answers can be very important.
To use reputable sources for medical information about diabetes, including those from their treating healthcare team and the American Diabetes Association.
To avoid becoming stressed about potential misinformation they may encounter from internet sources or laypeople.
To not compare their diabetes tests and management to those of their friends or family, as each patient's situation is unique.
Patients may also need to know some basic facts about diabetes. These include the following:
Compare the different types of diabetes and note that each person’s course is unique.
Some medications can induce or worsen diabetes.
Diet and lifestyle optimization are the foundation of diabetes management.
It is critical to display compassion when communicating with patients, especially when they may be overwhelmed by the implications of their diabetes. Allow time for patients to consider what is being discussed and use teach-back to ensure patient comprehension.
Summary
Diabetes is a prevalent and serious public health issue within the United States. The early and correct diagnosis and management of diabetes are essential to prevent the development and progression of complications associated with the disease. Several diagnostic tests are available for diagnosing diabetes, including fasting plasma glucose, the oral glucose tolerance test, random plasma glucose, and hemoglobin A1C. It is important to consider the patient's clinical presentation and risk factors in interpreting the results of these tests. In addition, screening for diabetes in patients at increased risk can help identify cases early and prevent complications.
It is vital that healthcare professionals, including physicians, nurses, and pharmacists, remain up to date with the newest diabetes care guidelines, which now incorporate inclusive language and a patient-first approach. This includes a firm understanding of the classification and diagnosis of diabetes.
References
Trujillo J, Haines S. Diabetes Mellitus. In: DiPiro JT, Yee GC, Posey L, Haines ST, Nolin TD, Ellingrod V. eds. Pharmacotherapy: A Pathophysiologic Approach, 11e. McGraw Hill; 2020. https://accesspharmacy.mhmedical.com/content.aspx?bookid=2577§ionid=228901946. Accessed June 22, 2023.
Banday MZ, Sameer AS, Nissar S. Pathophysiology of diabetes: An overview. Avicenna J Med. 2020;10(4):174-188. Published 2020 Oct 13. doi:10.4103/ajm.ajm_53_20
Fang M, Wang D, Coresh J, Selvin E. Undiagnosed Diabetes in U.S. Adults: Prevalence and Trends. Diabetes Care. 2022;45(9):1994-2002. doi:10.2337/dc22-0242
ElSayed NA, Aleppo G, Aroda VR, et al. Erratum. 2. Classification and diagnosis of diabetes: Standards of Care in Diabetes-2023. Diabetes Care 2023;46(Suppl. 1):S19-S40. Diabetes Care. 2023;46(5):1106. doi:10.2337/dc23-er05
ElSayed NA, Aleppo G, Aroda VR, et al. Introduction and Methodology: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S1-S4. doi:10.2337/dc23-Sint
World Health Organization. Diabetes. WHO. November 14, 2024. Accessed April 2, 2026. https://www.who.int/news-room/fact-sheets/detail/diabetes
Centers for Disease Control and Prevention. National Diabetes Statistics Report. CDC. January 21, 2026. Accessed April 2, 2026. https://gis.cdc.gov/grasp/diabetes/diabetesatlas-statsreport.html
Centers for Disease Control and Prevention. National Center for Health Statistics. Leading Causes of Death. CDC. Last Reviewed: February 5, 2026. Accessed April 2, 2026. https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
Centers for Disease Control and Prevention. Diabetes. Prediabetes: Could It Be You? CDC. February 17, 2026. Accessed April 2, 2026. https://www.cdc.gov/diabetes/communication-resources/prediabetes-statistics.html#:~:text=What%20to%20know,Last%20updated:%20February%2017%2C%202026
Centers for Disease Control and Prevention. Diabetes. Gestational Diabetes. CDC. May 15, 2024. Accessed April 2, 2026. https://www.cdc.gov/diabetes/about/gestational-diabetes.html
Bengtson AM, Ramos SZ, Savitz DA, Werner EF. Risk Factors for Progression From Gestational Diabetes to Postpartum Type 2 Diabetes: A Review. Clin Obstet Gynecol. 2021;64(1):234-243. doi:10.1097/GRF.0000000000000585
Diaz-Santana MV, O'Brien KM, Park YM, Sandler DP, Weinberg CR. Persistence of Risk for Type 2 Diabetes After Gestational Diabetes Mellitus. Diabetes Care. 2022;45(4):864-870. doi:10.2337/dc21-1430
Mikhail N, Wali S, Brown AF. Ethnic Disparities in Diabetes. Endocrinol Metab Clin North Am. 2021;50(3):475-490. doi:10.1016/j.ecl.2021.05.006
Emily D. Parker, Janice Lin, Troy Mahoney, Nwanneamaka Ume, Grace Yang, Robert A. Gabbay, Nuha A. ElSayed, Raveendhara R. Bannuru; Economic Costs of Diabetes in the U.S. in 2022. Diabetes Care. 2024;47(1):26–43. doi.org/10.2337/dci23-0085
Wikimedia Commons. The regulation of glucose levels through Homeostasis. Glucose Homeostasis for Wikipedia.jpg. Wikimedia Commons. 2023. https://commons.wikimedia.org/wiki/File:Glucose_Homeostasis_for_Wikipedia.jpg. Accessed June 17, 2023.
Dickinson JK, Guzman SJ, Maryniuk MD, et al. The Use of Language in Diabetes Care and Education. Diabetes Care. 2017;40(12):1790-1799. doi:10.2337/dci17-0041
DISCLAIMER
The information provided in this course is general in nature, and it is designed solely to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals must consult their employer, healthcare facility, hospital, or other organization for guidelines, protocols, and procedures to follow. The information provided in this course does not replace those guidelines, protocols, and procedures, but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses is constantly changing. Any person taking this course understands that such a person must make an independent review of medication information before any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course or course material.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
RxCe.com
© RxCe.com LLC 2025: All rights reserved.