BURN CARE ESSENTIALS: A MULTIDISCIPLINARY APPROACH TO ASSESSMENT, TREATMENT, AND RECOVERY
Faculty:
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson is an Associate Professor of Internal Medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson, PharmD, BCPS, is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy, where she is course director of the Parenteral Products and Basic Pharmaceutics Lab courses.
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and licensed pharmacist. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Abstract
Burn injuries occur when the skin comes into contact with a damaging agent, including radiation, chemicals, high temperatures, electricity, or friction. Burn injuries are preventable, yet non-fatal burns remain among the leading causes of morbidity and mortality globally. These injuries, ranging from mild to severe, present unique challenges that necessitate a coordinated response from the healthcare team. The severity of burns is influenced by factors such as the duration and intensity of exposure and the burn's location on the body. This can lead to significant variability in burn-related morbidity and mortality. Prompt and effective treatment is essential to prevent complications and promote optimal healing. The management of burn injuries benefits significantly from applying the Interprofessional Education Collaborative (IPEC) competencies, which emphasize team-based care and collaboration. This continuing education activity will provide learners with a comprehensive review of the classification, pathophysiology, and management of burn injuries. Special attention will be given to the roles of the multidisciplinary care team to foster a deeper understanding of how interprofessional collaboration can enhance outcomes in burn care.
Accreditation Statements
In support of improving patient care, RxCe.com LLC is jointly accredited by the Accreditation CouncilTM for Continuing Medical Education (ACCME®), the Accreditation Council for Pharmacy Education (ACPE®), and the American Nurses Credentialing Center (ANCC®), to provide continuing education for the healthcare team.

Joint Universal Activity Number: The Joint Accreditation Universal Activity Numbers assigned to this activity are as follows:
Pharmacists: JA4008424-0000-26-152-H01-P
Pharmacy Technicians: JA4008424-0000-26-152-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit.
Credit Types:
Pharmacy - 2 Credits
Type of Activity: Application
Media: Computer-Based Training (i.e., online courses)
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Activity Pre-Test, Post-Test, and Activity Evaluation.
Release Date: July 1, 2026 Expiration Date: December 30, 2027
Target Audience: This educational activity is for Pharmacists and Pharmacy Technicians.
How to Earn Credit: From July 1, 2026, through December 30, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Take the “Educational Activity Pre-Test;”
Study the section entitled “Educational Activity;” and
Complete the Educational Activity Post-Test and Activity Evaluation. The Educational Activity Post-Test will be graded automatically. Following successful completion of the Educational Activity Post-Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
CE and CME Credits: Credits for this course will be uploaded to CPE Monitor® for pharmacists and pharmacy technicians.
Statement of Need
Burn injuries occur when the skin comes into contact with a damaging agent, including radiation, chemicals, high temperatures, electricity, or friction. These injuries, ranging from mild to severe, present unique challenges that necessitate a coordinated response from the healthcare team. This activity provides essential information to promote prompt and effective burn treatments.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Recall how to classify burn injuries
Compare and Contrast treatment strategies for minor burns
Recall complications of burn injuries
Describe effective communication strategies within the interprofessional healthcare team to ensure collaborative decision-making and coordinated care plans for burn injury management
Disclosures
The following individuals were involved in planning, developing, and/or authoring this activity: L. Austin Fredrickson, MD, FACP; Liz Fredrickson, PharmD, BCPS; and Pamela Sardo, PharmD, BS. None of the individuals involved in developing this activity has a conflict of interest or financial relationships related to the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity Pre-Test
Which of the following is classified as a partial-thickness burn that extends into the deeper dermis with a high risk of hypertrophic scarring?
Superficial partial-thickness burn
Deep partial-thickness burn
Superficial burn
Full-thickness burn
Which of the following best describes the classification of burns by depth?
Superficial, partial-thickness, and full-thickness
Minor, moderate, and severe
Acute, chronic, and systemic
First, second, and third degrees only
Hypovolemia in burn patients is primarily due to which of the following?
Poor nutritional intake
Direct fluid loss and fluid shifts to interstitial spaces
Increased metabolic rate
Decreased cardiac output
Educational Activity
Burn Care Essentials: A Multidisciplinary Approach to Assessment, Treatment, and Recovery
Introduction
Burn injuries can range from mild to severe and present unique challenges that necessitate a coordinated healthcare team response. Prompt and effective treatment is essential to prevent complications and promote optimal healing outcomes. The management of burn injuries benefits significantly from the application of the Interprofessional Education Collaborative (IPEC) competencies, which emphasize team-based care and collaboration. By leveraging the IPEC competencies—values and ethics, roles and responsibilities, interprofessional communication, and teamwork— healthcare professionals can ensure a high-quality, patient-centered approach to burn care. This continuing education activity will provide learners with a comprehensive review of the classification, pathophysiology, and management of burn injuries. Special attention will be given to the roles of the multidisciplinary care team to deepen understanding of how interprofessional collaboration can enhance outcomes in burn care.
Overview of Burn Injuries
Burn injuries occur when the skin comes into contact with a damaging agent, including radiation, chemicals, high temperatures, electricity, or friction. Burn injuries are preventable, yet non-fatal burns remain among the leading causes of morbidity and mortality globally.1,2 These injuries, which can range from mild to severe, present unique challenges that necessitate a coordinated healthcare team response.1 The severity of burns is influenced by factors such as the duration and intensity of heat exposure and the burn's location on the body.1 This can lead to significant variability in burn-related morbidity and mortality.1 Prompt and effective treatment is essential to prevent complications and promote optimal healing outcomes. While minor burns are often managed on an outpatient basis, severe burns typically require intensive, interdisciplinary treatment due to their potential for long-term physical, psychological, and social impacts.1
Classification of Burn Injuries
Burns can be distinguished by several characteristics, including their etiology (discussed in detail below), depth, and the percentage of body surface area affected.1,2 Superficial burns are limited to the epidermis, or outermost layer of the skin, and were previously noted as first-degree burns.2 Partial-thickness burns can be deep or superficial and involve the dermis.2 These were previously noted as second-degree burns.2 Superficial partial-thickness burns involve the superficial dermis. Deep partial-thickness burns extend to the deeper dermis and take longer to heal.2 Finally, full-thickness (third-degree) burns extend to the fat layer underlying the dermis.2 The classification of burn injuries is detailed further in Table 1 and illustrated in Figure 1.
Table 1
Classification of Burn Injuries1,2
| Classification | Depth | Characteristics | Healing Time | Risk of Scarring | Treatment |
|---|---|---|---|---|---|
| Partial-Thickness Burn | Epidermis | Appendage structures intact, superficial damage | 10–14 days | Low | May heal without surgical intervention |
| Deep Partial-Thickness Burn | Deeper layers of the dermis, greater appendage damage | Damage to deeper dermal layers, fewer intact structures | 3–6 weeks | High (hypertrophic scarring possible) | May require specialized wound care |
| Full-Thickness Burn | All layers of skin (epidermis, dermis, and subcutaneous tissues) | Complete destruction of skin layers | Varies (requires surgical intervention) | Very High | Typically requires surgery (e.g., skin grafting) |
Figure 1
Classification of Burn Injuries by Depth (with older degree nomenclature used)3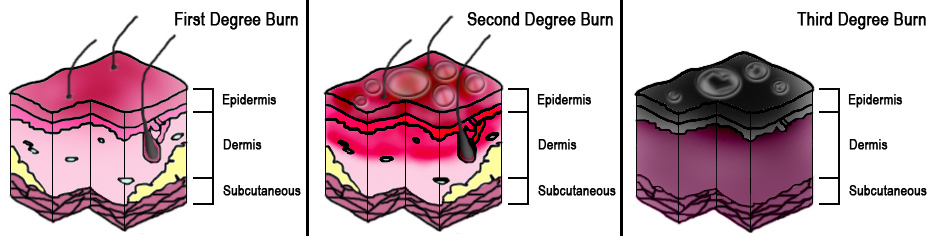
Burn Injury Epidemiology and Etiology
Epidemiology
Burn injuries represent a significant public health issue worldwide, and addressing them requires the coordinated efforts of interprofessional care teams. They account for substantial morbidity and mortality globally. Interprofessional teams, including epidemiologists, public health officials, and clinical care providers, can collaborate to analyze burn injury patterns and target high-risk populations.
In the United States, data from the American Burn Association (ABA) and the Centers for Disease Control and Prevention (CDC) highlight the scope of the issue. The American Burn Association (ABA) is a member-based organization that seeks to improve the lives of individuals affected by burn injuries.4 In 2021, the CDC reported 398,000 fire- or burn-related injuries and 252,000 injuries from hot objects or substances.4 The ABA estimated there is one fire-related death in the United States (US) every 2 hours and 17 minutes, and the World Health Organization estimates that burns cause 180,000 deaths every year and remain a significant global public health problem.4,5 Burn injury demographics pertinent to the US are presented in Table 2.4
Table 2
Demographics of Burns Injuries4
| Category | Statistics |
|---|---|
| Burn Admissions | 29,165 admissions/year (88.5 per million people/year) |
| Inpatient Mortality | 2.7% overall (795 deaths) |
| Admissions by Burn Severity | 52.4% for minor burns (15,280 cases) 0.36% mortality rate |
4.4% for extensive burns with surgery and ventilation (1,290 cases) 17.8% mortality rate | |
32% for deep burns with surgery, no prolonged ventilation (9,340 cases) 2.6% mortality rate | |
| Hospitals Handling Burn Cases | 94 hospitals with ≥100 burn admissions/year |
| Seasonality of Burn Admissions | 37.5% of admissions occur May-August |
| Geographic Distribution | Most admissions: South Atlantic (26.0%) |
| Fewest admissions: New England (3.0%) | |
| Demographics | Gender: 33.3% Female, 66% Male |
| Ethnicity: 57.1% White non-Hispanic, 19.6% Black non-Hispanic, 14.5% Hispanic, 2.6% Asian/Pacific Islander, 0.8% Native American | |
| Age Distribution | Children (under 18): Median age 3 years Adults: Median age 49 years |
Risk Factors
Understanding the risk factors for burns enables an interprofessional care team to create targeted prevention and management strategies and mitigate these risks. Certain groups are more vulnerable to burn injuries due to a range of factors related to gender, age, regional disparities, socioeconomic status, and other specific conditions. Females have slightly higher burn-related death rates than males. Males are more likely than females to receive burns globally.5 This increased risk is primarily due to open-fire cooking and the use of unsafe cookstoves that can ignite loose clothing.4 The use of open flames for heating and lighting further contributes to this risk, as does exposure to self-directed or interpersonal violence.5
Age is another significant factor, particularly for children. Young children, especially those under five, are highly vulnerable to burn injuries, which rank as the fifth most common cause of non-fatal childhood injuries.5 A substantial portion of these injuries stems from a lack of adult supervision and instances of child maltreatment.5
Socioeconomic factors and social drivers of health (SDOH) are critical to understanding burn risk, and addressing these challenges requires an interprofessional, patient-centered approach. Individuals in low- and middle-income countries face greater hazards, but poverty, overcrowding, and other SDOH also contribute significantly to burn risks in any setting. By leveraging a team-based approach, interprofessional care teams can develop strategies to mitigate these risks and improve outcomes for vulnerable populations.5 As an example, social workers and public health professionals can collaborate to provide access to safer cooking alternatives and home safety equipment. Nurses and health educators can deliver culturally appropriate safety education tailored to the unique needs of these communities.
Other risk factors include occupational hazards that increase exposure to fire, young girls’ involvement in cooking and child-rearing tasks, and certain underlying medical conditions, such as epilepsy, peripheral neuropathy, and various physical and cognitive disabilities.5 Alcohol abuse and smoking also elevate the risk, as does easy access to harmful chemicals used in assaults, like acid.5 Physicians and rehabilitation specialists can tailor treatment plans that account for these individual vulnerabilities, and nurses can assist patients and caregivers in recognizing and mitigating risks specific to these conditions. Pharmacists can help the team by adjusting medication regimens to reduce side effects that may contribute to falls or accidents.
Understanding these risk factors is essential for effective prevention efforts, especially for vulnerable populations. Safety education, improved supervision, and targeted public awareness initiatives can help reduce the incidence of burns and their associated mortality and morbidity worldwide.
Etiology
The etiology of burns influences treatment decisions, and care teams must integrate their expertise to manage these injuries effectively. The management of burn injuries necessitates a robust, interprofessional approach rooted in the IPEC competencies—Values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teams/Teamwork. By collaboratively addressing epidemiological patterns, risk factors, and diverse etiologies, healthcare teams can enhance prevention, treatment, and recovery for individuals affected by burns.
Burn injuries can arise from several causes, including thermal, electrical, chemical, and radiation exposures, and these factors play a role in determining the severity of the injury.1 Understanding the causes of burns can assist care team members in determining appropriate treatment strategies and recognizing potential complications that may arise.
Thermal Injuries
Thermal burn injuries are caused by contact with an external heat source, such as a flame or hot liquid.2 The temperature and duration of exposure determine the severity of thermal injuries.1 Types of thermal injuries include the following:
Scalds: These are injuries caused by contact with hot liquids and are the most common type of burn injury.1 These types of burns often cause partial-thickness burns.1
Dry Heat Injuries: These injuries result from direct contact with flames or radiant heat.1 These types of burns typically result in partial or full-thickness burns.1
Contact Burns: These injuries result from prolonged contact with hot objects.1 These types of burns are typically deep.1
For example, during the treatment of a thermal burn, the physician may assess the depth of the injury, while the nurse educates the patient on wound care and demonstrates the dressing technique. The pharmacist ensures appropriate pain management and adjusts fluid resuscitation based on the patient’s condition. Effective communication tools like SBAR (Situation, Background, Assessment, Recommendation) streamline these interactions, ensuring seamless care and enhancing interprofessional collaboration.
Electrical Injuries
The generation of heat and subsequent electroporation of cell membranes results in electrical burns.2 A minority of burn injuries are the result of electrical injuries, and numerous variables play into their severity.1 These include voltage, current type, contact duration, and the pathway of current through the patient’s body.1 Low-voltage injuries can cause localized burns, while high-voltage exposures lead to extensive tissue damage, cardiac arrhythmias, and even limb loss.1 Burns may also result from an electrical arc, causing partial-thickness burns on exposed skin.1
Chemical Injuries
Chemical burns also account for a minority of burn injuries (approximately 3%).1 These types of burns involve tissue damage that results from chemical reactions, and they may involve strong acids, strong alkalis (such as lye), phenols, phosphorus, or products like paint thinners.1,2 Factors impacting these types of burns include the concentration, amount, duration of contact, and mechanism of action of the implicated chemical.1
Radiation Injuries
Radiation burns are caused by prolonged exposure to ultraviolet (UV) radiation from sources such as the sun and tanning beds.2 Alpha particles cause significant damage if ingested or inhaled, but cannot penetrate the skin.1 Beta particles cause superficial burns similar to sunburns.1 Gamma rays can penetrate deep into the body, damaging internal tissues and causing systemic issues like Acute Radiation Syndrome.1
Pathophysiology of Burns
Burns can result in local and systemic effects in patients.1 The care team should recognize both types of effects to anticipate possible outcomes and devise treatment strategies. The skin plays an important role in mitigating the spread of burn damage, but this ultimately depends on the temperature and duration of exposure to the causative agent.1,2 Heat from burns causes protein denaturation, leading to coagulative necrosis in the affected tissue.2 The sites of burns have been divided into three zones, which are detailed in Table 3.1
Table 3
Zones of Cutaneous Burn Injuries1
| Zone | Description |
|---|---|
| Zone of Coagulation | The area of maximal damage where irreversible tissue necrosis occurs at the time of injury |
| Zone of Stasis | Surrounds the coagulation zone and is moderately damaged Damage results in impaired tissue perfusion, and the zone may recover or progress to necrosis depending on the wound environment |
| Zone of Hyperemia | Contains dilated vessels caused by inflammation and is characterized by increased blood flow to healthy tissues Minimal risk of necrosis unless there is severe sepsis or prolonged hypoperfusion |
The systemic effects of burns can be notable, especially when more than 30% of the total body surface area (TBSA) is affected.1 A primary consequence is burn shock, which is characterized by circulatory dysfunction, edema, and microcirculatory damage.1,2 Even with adequate fluid resuscitation, burn shock remains irreversible and often results in multiple organ failure. 1,2 Burns also trigger extensive edema formation, which occurs in two phases: a rapid increase in tissue water content within the first hour and a slower, gradual increase over the next 12–24 hours.1,2 The severity of edema is influenced by fluid resuscitation efforts, with increased blood flow and capillary pressure further exacerbating tissue swelling.1,2
At the cellular level, burns cause membrane depolarization in various tissues, including skeletal muscle, cardiac cells, and the liver. 1,2 This results in sodium and water accumulation within cells, contributing to cell dysfunction and edema.1,2 These injuries also induce a profound hypermetabolic response, which varies depending on the size of the burn.1,2 In patients with burns covering more than 40% of TBSA, the metabolic rate can more than double, driven by increased secretion of hormones like catecholamines, cortisol, and inflammatory cytokines such as IL-1 and IL-6.1,2
Finally, burns disrupt glucose metabolism, leading to persistent hyperglycemia and insulin resistance.1,2 The heart and kidneys are particularly vulnerable, with burn injuries reducing cardiac output and glomerular filtration rates, potentially causing renal failure if not properly managed. Endocrine disturbances, particularly in the hypothalamic-pituitary axis, further complicate recovery by affecting hormones such as thyroid hormone, growth hormone (GH), and insulin-like growth factor (IGF-1).1,2 Overall, the systemic effects of burns involve complex metabolic, hormonal, and inflammatory dysregulation, which pose significant challenges to recovery and rehabilitation, necessitating comprehensive management and monitoring of multiple organ systems.1,2 Table 4 summarizes the complications of burns at local and systemic levels.2
Table 4
Summary of Complications2
| Type | Complication | Description |
|---|---|---|
| Systemic | Hypovolemia |
|
| Infection |
| |
| Metabolic Abnormalities |
| |
| Hypothermia |
| |
| Ileus |
| |
| Local | Eschar |
|
| Scarring and Contractures |
|
Assessment of Burns
Burn assessment requires the combined expertise of an interprofessional team to evaluate depth, extent, and complications. Clear communication, shared decision-making, and role delineation are crucial. Burn assessment involves clinically assessing the depth and extent of the burn.1,2 In some cases, imaging and laboratory testing may be required.1,2 Interprofessional communication and teamwork are critical in recognizing these signs and determining the need for further intervention. A burn infection may be evident by the following signs:6
Wound exudate
Impaired wound healing
Feeding intolerance
Decreased platelet count
Increased serum glucose
Estimating the percentage of total body surface area (TBSA) involved is crucial in managing burn injuries.2 Three common methods for quickly approximating the affected area are the rule of nines, Lund and Browder charts, and the palm method.2 While the rule of nines provides a faster assessment, the Lund and Browder charts are more accurate, especially in children, as they adjust for age-related differences in body surface area.2 The palm method uses the patient’s palm to estimate smaller, scattered burns, with the palm (excluding fingers) representing about 0.5% TBSA and the full palm (including fingers) representing 1% TBSA.2 However, the palm method can overestimate surface area in cases of large burns. Figure 2 illustrates the differences between the rule of nines and Lund-Browder charts. Table 5 details the burn depth assessment.7
Figure 2
Estimating Percent TBSA8
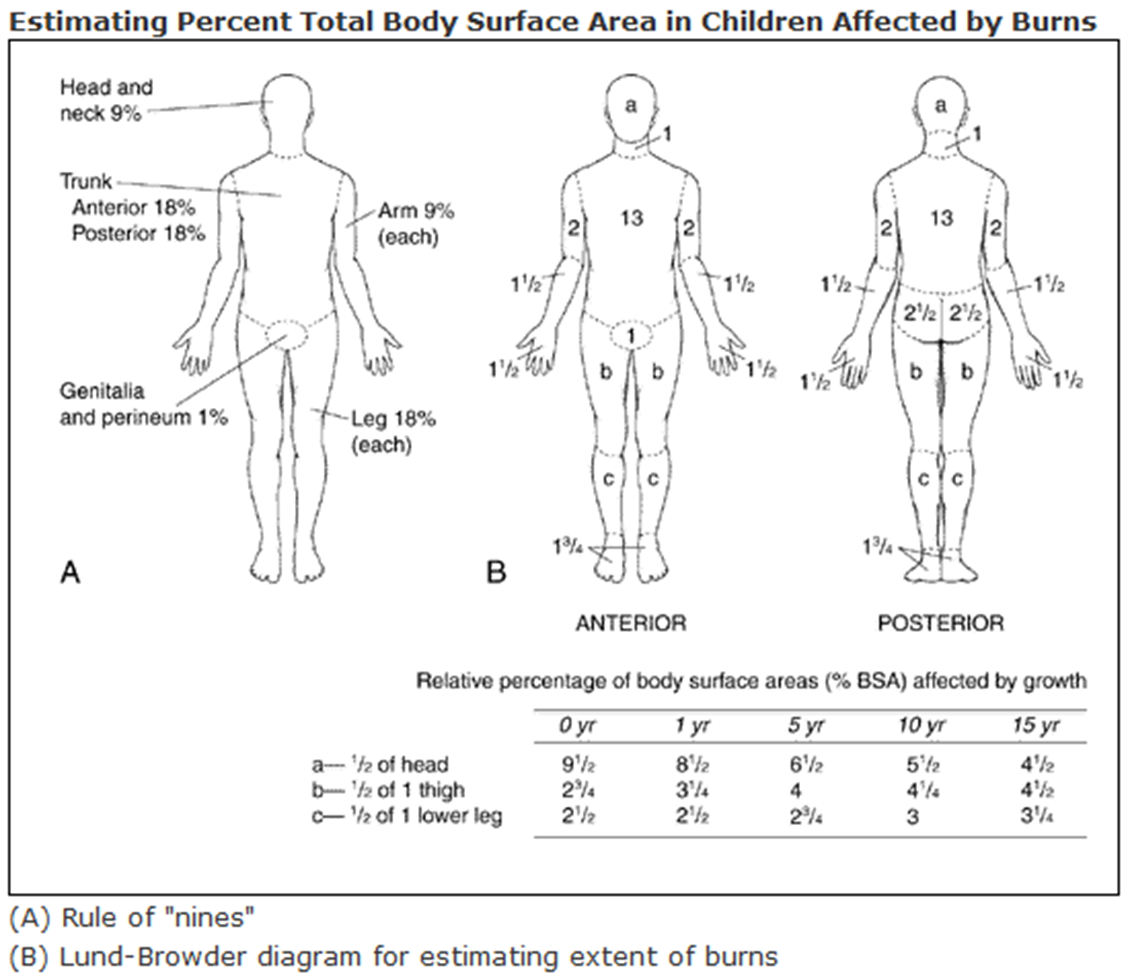
Table 5
Burn Depth Assessment7
| Epidermal Burn | Superficial Dermal/Superficial Partial Burn | Deep Dermal/ Deep Partial Burn | Full Thickness Burn | |
|---|---|---|---|---|
| Pathology | Involves the epidermis only | Involves the epidermis and upper dermis | Involves the epidermis and most of the dermis | Involves the epidermis and all of the dermis |
| Appearance | Red only | Pale pink; blanches to pressure | Red or pale pink; non-blanching | Waxy and white; leathery; non-blanching |
| Blistering | None or only a few days later | Yes, within hours of the burn | Yes—early blistering | No |
Patients meeting specific criteria, such as extensive TBSA involvement or burns in high-risk areas (e.g., face, hands, feet), require referral to specialized burn centers. Interprofessional collaboration ensures seamless transitions of care. Some examples include the following:
Care coordinators arrange transportation and communicate referral details with the burn center.
Nurses provide detailed handoffs, including assessments and wound care protocols.
Physicians ensure timely updates to the receiving specialists regarding the patient's condition.
Table 6 provides criteria for referring patients to burn centers.9
Table 6
American Burn Association Criteria for Burn Center Referral9
| Criteria |
| Burns to the face, hands, feet, major joints, genitalia, or perineum |
| Children in health care facilities without staff trained to treat children or appropriate equipment for children |
| Concurrent trauma |
| Electrical or chemical burns |
| Full-thickness (third-degree) burns at any age |
| Greater than 10% of the total body surface area involved |
| Inhalation injuries |
| Need for special support (social, emotional, rehabilitative) |
| Preexisting medical issues that may complicate treatment or recovery or increase mortality risk |
Treatment and Management Strategies
The management of burn injuries benefits significantly from applying the Interprofessional Education Collaborative (IPEC) competencies, which emphasize team-based care and collaboration.10 By leveraging the IPEC competencies—values and ethics, roles and responsibilities, interprofessional communication, and teamwork—healthcare professionals can ensure a high-quality, patient-centered approach to burn care.
Interprofessional Care Teams
Effective communication and shared decision-making are critical during initial burn assessment and treatment.11 The management of burn injuries exemplifies the need for integrated multidisciplinary care due to the complex nature of these cases. Burn care involves a diverse team of specialists working collaboratively to provide comprehensive care. Research highlights the variability and complexity of multidisciplinary teams in healthcare, emphasizing the importance of defining team components to optimize team functioning.11 Strong communication will be a cornerstone of team success and can help foster coordination within the team and with patients and their families. However, while diverse professional healthcare backgrounds are an asset, they can lead to conflicts, miscommunication, and a loss of patient confidence if members do not communicate well.11
Key challenges include conflicting professional opinions and the potential for patients or their families to inadvertently exacerbate team disagreements.11 These issues can be mitigated through frequent, open communication and respect for diverse perspectives.11 Emotional dynamics and conflict resolution are critical for smooth team functioning, and recognizing the value of each member's input is essential. A well-functioning team is characterized by common objectives and aligned values, enabling the delivery of optimal care for burn patients.11 Each team member's primary roles and contributions concerning burn management are summarized in Table 7 below.
Challenges in this setting have been described in the literature elsewhere. One study examined communication networks within healthcare teams, focusing on the interaction patterns among 71 health professionals in a burn unit across four roles: physicians, nurses, health management/support personnel (dietitians, pharmacists, social workers), and other health professionals (therapists, medical students).12 Using a cross-sectional survey, researchers identified communication ties based on discussions about patient care during shifts.12 Findings revealed that 94% of health management/support personnel’s ties were interprofessional, compared to 60% for nurses. Nurses and other health professionals were less likely than physicians to form ties, and nurses were 1.64 times as likely to communicate with other nurses as with non-nurses.12 Physicians and health management/support personnel showed no significant preference for interprofessional communication.12 Understanding these networks is crucial for improving teamwork in healthcare, with future studies needed to explore the quality and types of interprofessional interactions.12
Table 7
Team Member's Primary Roles and Contributions in Burn Management11
| Role | Responsibilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Barriers for care teams are presented in Table 8.
Table 8
Barriers to Interprofessional Collaboration
| Barrier | Description | Solution |
| Communication Challenges | Miscommunication or lack of communication among team members can lead to errors and fragmented care. | Implement structured communication tools, such as SBAR, and schedule routine interdisciplinary meetings. |
| Role Ambiguity | An unclear understanding of each team member's roles and responsibilities can cause overlap or gaps in care. | Clearly outline roles and responsibilities and provide interprofessional education to foster mutual respect. |
| Hierarchical Structures | Traditional hierarchies can inhibit open communication, with lower-ranking members hesitant to voice concerns or suggestions. | Encourage equality, inclusive discussions, and train leaders to value input from all disciplines. |
| Time Constraints | Busy schedules and heavy workloads can limit opportunities for team collaboration and communication. | Utilize brief, focused huddles or bedside rounds, and allocate specific times for interdisciplinary activities. |
| Cultural and Professional Differences | Variations in professional cultures, terminologies, and approaches can lead to misunderstandings and conflicts. | Offer cultural competency training and engage in team-building activities to build trust and rapport. |
| Lack of Interprofessional Education | Limited training on collaborative practices during professional education can result in inadequate preparation for teamwork. | Incorporate interprofessional education modules into healthcare training and offer continuing education workshops. |
| Resource Limitations | Insufficient staffing, facilities, or financial resources can hinder effective implementation of collaborative practices. | Advocate for resources and optimize existing tools and technologies to facilitate communication and coordination. |
Treatment Strategies
Burns to the face or neck, or resulting from enclosed fires or chemicals, increase the risk of airway injury and require close monitoring.9 A quick assessment to identify the cause and extent of the burn is critical, though determining burn depth can be difficult initially.9 Deep burns often exhibit slow or absent skin blanching, and pain intensity decreases with burn depth.9 Burn injuries are dynamic and can worsen over 24 to 72 hours, with even minor burns potentially deepening due to factors like inadequate treatment or infection.9 Treatment strategies and their related benefits are summarized in Table 9 and discussed in more detail below.
Table 9
Treatment1
| Treatment | Description | Key Benefits |
|---|---|---|
| Cooling of Burned Areas | Immediate cooling of burned tissue at 10–20°C to reduce temperature and pain | Reduces tissue damage, provides relief, and avoids frostbite or hypothermia |
| Fluid Resuscitation | Uses the Parkland formula to estimate and administer fluids after severe burns | Prevents hypovolemic shock, maintains organ function |
| Ventilation | Lung-protective ventilation strategies for respiratory burns | Reduces lung damage, improves respiratory outcomes |
| Surgical Treatment | Early excision of burn wounds, skin grafting, and reconstructive surgery | Lowers infection risk, speeds healing, restores function and appearance |
| Sepsis Management | Prevention through antimicrobial dressings, excision, and nutritional support | Reduces infection risk, lowers sepsis-related mortality |
| Thermoregulation | Raising ambient temperature in care settings to maintain patient body temperature | Reduces hypermetabolism, prevents hypothermia |
| Contracture Prevention | Physical therapy, corticosteroids, hydrotherapy, and surgical interventions | Prevents permanent contractures, improves mobility |
| Hormonal Regulation | Use of growth hormone, IGF-1, insulin, oxandrolone, and propranolol | Promotes muscle growth, reduces catabolism, and improves healing |
| Nutrition | Enteral feeding with high-protein, high-carbohydrate diets | Maintains lean body mass, preserves gut function, reduces infection risk |
Minor Burns
The primary goals of treating minor burns are to limit damage, clean the wound, and manage pain.9 For scalds, removing clothing immediately helps minimize injury.9 Chemical burns require careful removal of contaminated clothing using protective gear.9 To prevent further complications, any items that could restrict circulation (e.g., jewelry, belts) should be removed, and the environment should be kept warm, as burns impair thermoregulation.9
Cooling the burn with running water (46.4°F to 77°F) for at least 20 minutes, ideally within 30 minutes but effective up to three hours post-burn, reduces burn depth and accelerates healing.9 However, ice should not be used, as it can cause further damage.9 Cleaning with tap water is sufficient to prevent infection, and sterile or antiseptic agents are unnecessary.9
Superficial burns typically do not require dressings, though wet gauze may reduce pain.9 Maintaining a moist environment is crucial for superficial partial-thickness burns to promote healing and prevent complications. Blister management, particularly in partial-thickness burns, is debated.9 Large or joint-area blisters may require debridement to reduce infection risk and improve healing, though recent evidence suggests aspiration may be equally effective.9
There are two common approaches to dressing partial-thickness burns. One involves applying a topical antimicrobial agent with regular dressing changes to monitor progress. Silver sulfadiazine is a popular choice, though it has been shown to delay healing and may increase infection risk, with studies suggesting it impairs immune function and wound recovery.9 Topical agents are described in Table 10.9
Table 10
Topical Treatments9
| Agent | Description | Advantages | Disadvantages |
|---|---|---|---|
| Bacitracin | Antimicrobial ointment | Inexpensive and painless; can be used on the face and near mucous membranes | Narrow microbial coverage, frequent dressing changes, and does not penetrate eschar |
| Impregnated nonadherent gauze | Semiocclusive, non-absorptive dressing | A nonadherent barrier helps maintain a moist environment and clings to the body | No antimicrobial activity |
| Mafenide acetate | Water-based cream; bacteriostatic against gram-positive and gram-negative bacteria | Pseudomonal coverage, penetrates eschar, can be used for deep burns or on the face | Pain with application may delay wound healing and is associated with metabolic acidosis |
| Medical-grade honey | A variety of preparations, including honey-based hydrogel dressings | Inhibits growth of common burn pathogens, reduces healing time for partial-thickness burns | Low-quality evidence |
| Mupirocin | Ointment; inhibits bacterial protein and RNA synthesis | Good gram-positive antimicrobial coverage, effective against MRSA, painless, may be used on the face | Frequent dressing changes, expensive |
| Silver sulfadiazine | Water-based cream; interferes with bacterial DNA synthesis | Painless, long shelf life, broad antimicrobial coverage | Delays wound healing, frequent dressing changes, contraindicated in certain populations |
Severe Burns
Initial care for burns in the prehospital setting includes providing oxygen for smoke inhalation, extinguishing ongoing burning, and removing hot or smoldering material.2 For chemical burns, extensive flushing with water is essential.2 Partial-thickness and full-thickness burns covering more than 10% of the total body surface area (TBSA) require intravenous (IV) fluids based on the Parkland formula to address fluid loss and prevent shock.2
Wound care involves cleansing, dressing, and ongoing assessment.2 Small blisters may be left intact, while ruptured ones are debrided. Antimicrobial ointments, silver dressings, or biosynthetic coverings may be applied to protect the wound.2 If burns exceed 20% TBSA or if the patient is malnourished, nutritional support is initiated.2 For larger or complex burns, specialized care in burn centers is often necessary.2 Surgery, including escharotomy, excision, and grafting, is required for deep partial-thickness and full-thickness burns, often within three days of injury, to prevent sepsis and promote healing.2
Infections are managed without routine prophylactic antibiotics; those presenting after five days require broad-spectrum antibiotics tailored to culture results.2 Physical and occupational therapy are crucial to maintain mobility and prevent contractures.2 Outpatient treatment, where feasible, involves daily dressing changes and maintaining cleanliness, elevation, and compression.2
Preventing Burn Injuries
Burns are largely preventable, and high-income countries have made significant strides in reducing burn-related deaths by implementing comprehensive prevention strategies and improving care for burn victims.5 Effective prevention requires a multidimensional, interprofessional approach, as emphasized by the IPEC competencies. Collaboration across disciplines ensures that prevention efforts target specific hazards, educate vulnerable populations, and equip communities with the skills and resources needed to minimize risks. A successful prevention plan should be multidimensional, focusing on improving awareness, creating and enforcing effective policies, identifying risk factors, setting research priorities, promoting interventions, providing prevention programs, and strengthening burn care and capacity.5
Several specific measures can help reduce burn risks at individual, community, and public health levels. These include enclosing fires and controlling open-flame heights in homes, and promoting safer stoves and fuels. Housing regulations should encourage fire-safe design and materials, while stove designs should prioritize stability and child safety.5 Lowering hot water tap temperatures, promoting fire safety education, and encouraging smoke detectors, fire sprinklers, and fire-escape systems are crucial.5 Compliance with industrial safety regulations, use of fire-retardant fabrics for children's sleepwear, and avoiding smoking in bed are also vital steps.5
Summary
Burn injuries, which can range from mild to severe, present a unique and complex challenge for healthcare professionals, requiring prompt and effective treatment to prevent complications and promote healing. While minor burns can often be managed on an outpatient basis, severe burns require intensive treatment and have the potential to create long-lasting impacts on patients.
Burn injuries occur when the skin comes into contact with a damaging agent, including radiation, chemicals, high temperatures, electricity, or friction. Burns can be distinguished by several characteristics, including their etiology, depth, and the percentage of body surface area affected.
Burn assessment requires the combined expertise of an interprofessional team to evaluate depth, extent, and complications. Clear communication, shared decision-making, and role delineation are crucial. The management of burn injuries benefits significantly from the application of the Interprofessional Education Collaborative (IPEC) competencies, which emphasize team-based care and collaboration.
Burns can result in local and systemic effects in patients. The care team should recognize both types of effects to anticipate possible outcomes and devise treatment strategies. Criteria may be present for referring patients to burn centers.
References
Żwierełło W, Piorun K, Skórka-Majewicz M, Maruszewska A, Antoniewski J, Gutowska I. Burns: Classification, Pathophysiology, and Treatment: A Review. Int J Mol Sci. 2023;24(4):3749. Published 2023 Feb 13. doi:10.3390/ijms24043749
Carter, D. Burns. Merck Manual. September 2024. Accessed November 2024. https://www.merckmanuals.com/professional/injuries-poisoning/burns/burns
Wikimedia Commons. Burn Degree Diagram. Accessed November 2024. https://commons.wikimedia.org/wiki/File:Burn_Degree_Diagram.png
Burn Incidence Fact Sheet. The American Burn Association. Accessed November 2024. https://ameriburn.org/resources/burn-incidence-fact-sheet/
World Health Organization. Burns. October 2023. Accessed November 2024. https://www.who.int/news-room/fact-sheets/detail/burns
Kamolz LP, Parvizi D, Giretzlehner M, et al: Burn surface area calculation: What do we need in future. Burns 40(1):171-172, 2014. doi: 10.1016/j.burns.2013.07
Wall S, Perumal-Pillay VA. Burning Questions: What Should the Pharmacist Know about Managing Minor Burns?. Pharmacy (Basel). 2022;10(4):100. Published 2022 Aug 22. doi:10.3390/pharmacy10040100
Radiation Emergency Medical Management. U.S. Health and Human Services. November 13, 2024. Accessed December 2, 2024. https://remm.hhs.gov/burns.htm
Lanham JS, Nelson NK, Hendren B, Jordan TS. Outpatient Burn Care: Prevention and Treatment. Am Fam Physician. 2020;101(8):463-470.
Interprofessional Education Collaborative. IPEC Core Competencies for Interprofessional Collaborative Practice: Version 3. November 20, 2023. Washington, DC: Interprofessional Education Collaborative.
Al-Mousawi AM, Mecott-Rivera GA, Jeschke MG, Herndon DN. Burn teams and burn centers: the importance of a comprehensive team approach to burn care. Clin Plast Surg. 2009;36(4):547-54. doi: 10.1016/j.cps.2009.05.015
Shoham DA, Harris JK, Mundt M, McGaghie W. A network model of communication in an interprofessional team of healthcare professionals: A cross-sectional study of a burn unit. J Interprof Care. 2016;30(5):661-667. doi:10.1080/13561820.2016.1203296
DISCLAIMER
The information provided in this course is general in nature, and it is designed solely to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals must consult their employer, healthcare facility, hospital, or other organization for guidelines, protocols, and procedures to follow. The information provided in this course does not replace those guidelines, protocols, and procedures, but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses is constantly changing. Any person taking this course understands that such a person must make an independent review of medication information before any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course or course material.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
RxCe.com
© RxCe.com LLC 2025: All rights reserved.