COMPOUNDING TECHNIQUES: NONSTERILE ORAL DOSAGE FORMS
Faculty:
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy, where she is course director of the Parenteral Products and Basic Pharmaceutics Lab courses.
Pamela Sardo, PharmD, BS
Pamela Sardo is a freelance medical writer and licensed pharmacist. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, and Veterans Affairs, as well as in managed health care, with responsibilities across a broad range of therapeutic classes and disease states.
Abstract
Pharmaceutical compounding is considered both an art and a science and involves preparing medications tailored to an individual’s specific health needs. Compounded nonsterile preparations (CNSPs) encompass many different oral dosage forms, including capsules, tablets, suspensions, solutions, and lozenges. These dosage forms enhance medication adherence, mask the bitter taste of active pharmaceutical ingredients (APIs), and protect APIs from degradation. Pharmacists and pharmacy technicians who compound oral medications should be well-versed in compounding standards and skilled in the techniques required to prepare medications that are effective, safe, and high-quality.
Accreditation Statements
In support of improving patient care, RxCe.com LLC is jointly accredited by the Accreditation CouncilTM for Continuing Medical Education (ACCME®), the Accreditation Council for Pharmacy Education (ACPE®), and the American Nurses Credentialing Center (ANCC®), to provide continuing education for the healthcare team.

Joint Universal Activity Number: The Joint Accreditation Universal Activity Numbers assigned to this activity are as follows:
Pharmacists: JA4008424-0000-26-072-H07-P
Pharmacy Technicians: JA4008424-0000-26-072-H07-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit.
Credit Types:
Pharmacy - 2 Credits
Type of Activity: Knowledge
Media: Computer-Based Training (i.e., online courses)
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Activity Pre-Test, Post-Test, and Activity Evaluation.
Release Date: May 22, 2026 Expiration Date: May 22, 2029
Target Audience: This educational activity is for Pharmacists and Pharmacy Technicians
How to Earn Credit: From May 22, 2026, through May 22, 2029, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Take the “Educational Activity Pre-Test;”
Study the section entitled “Educational Activity;” and
Complete the Educational Activity Post-Test and Activity Evaluation. The Educational Activity Post-Test will be graded automatically. Following successful completion of the Educational Activity Post-Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
CE and CME Credits: Credits for this course will be uploaded to CPE Monitor® for pharmacists and pharmacy technicians. Physicians may receive AMA PRA Category 1 Credit™️ and use these credits toward Maintenance of Certification (MOC) requirements. Physician Assistants may earn AAPA Category 1 CME credits, reportable through PA Portfolio. All learners shall verify their individual licensing board’s specific requirements and eligibility criteria.
Statement of Need
Oral dosage forms remain essential because they support medication adherence, mask unpleasant taste, and provide practical options when commercially available products do not meet patient needs. Regulatory agencies have increased monitoring and oversight of compounding due to deficiencies that adversely affect patients. There is an ongoing need for compounding professionals to maintain competencies because errors in technique can affect dose uniformity, product quality, and patient outcomes. It is critical to strengthen the ability to apply USP-compliant compounding principles. This activity aims to reinforce appropriate weighing, measuring, mixing, particle-size reduction, and formulation selection to address gaps across diverse patient populations. The ultimate goal is to prepare safe, effective, and high-quality dosage forms.
Learning Objectives:
Upon completion of this educational activity, participants should be able to:
Recall the importance of oral dosage forms
Identify compounding techniques used to prepare capsules and tablets
Describe the preparation of solutions and suspensions
Recall methods by which to prepare lozenges
Disclosures
The following individuals were involved in planning, developing, and/or authoring this activity: Liz Fredrickson, PharmD, BCPS, and Pamela Sardo, PharmD, BS. None of the individuals involved in developing this activity has a conflict of interest or financial relationships related to the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity Pre-Test
According to updated USP <795> standards, which of the following is essential for compounding personnel preparing oral dosage forms?
Only final product labeling is required without assessing microbial contamination
Use of automated equipment for all preparations rather than the mortar and pestle
The elimination of documentation requirements that reveal product variability
Competency in compounding techniques, including measuring and mixing
Which of the following is the FIRST step when preparing a suspension?
Achieving particle size reduction of the active pharmaceutical ingredient
Wetting the active pharmaceutical ingredient
Blending the active pharmaceutical ingredient with the vehicle
Mixing the active pharmaceutical ingredient and the wetting agent to form a paste
An inspector is observing a compounding professional formulate a lozenge. The inspector stops the process to discuss a suboptimal misstep. Which of the following steps is identified as being a suboptimal misstep?
The ingredients are placed into a mold that requires calibration to determine the weight of each lozenge
Calibration is observed to determine the weight of each lozenge based on the specific base used.
This calibration involves placing the lozenge base into molds as a powder without melting
The inspector observes cooling the blank lozenges, weighing them, and then calculating the average weight per lozenge
Educational Activity
Compounding Techniques: Nonsterile Oral Dosage Forms
Highlights Compounding personnel should be competent in measuring, mixing, and preparing oral dosage forms to ensure safety, quality, and accuracy Oral dosage forms (capsules, tablets, solutions, suspensions, lozenges) support adherence, taste masking, and API stability Particle size reduction and proper mixing techniques are essential to achieve homogeneity and consistent dosing Dosage form–specific techniques vary, including capsule filling, tablet molding, solution preparation, and suspension formulation Preparation of solutions and suspensions requires careful consideration of solubility, pH, and order of mixing Quality control procedures (e.g., weight, uniformity, appearance, pH) are essential to ensure formulation accuracy and performance USP <795> emphasizes personnel competency, documentation, and standardized compounding practices to reduce the risk of contamination, variability, and errors Proper storage conditions must be followed for each dosage form to maintain stability and product integrity |
Introduction
Pharmaceutical compounding involves preparing medications unique to an individual’s specific health needs. Compounded nonsterile preparations encompass many different oral dosage forms, including capsules, tablets, suspensions, solutions, and lozenges. These dosage forms play essential roles in the pharmaceutical care of patients, including enhancing medication adherence, flavoring, and protecting compounding ingredients from deterioration. Pharmacists and pharmacy technicians who compound oral medications should be well-versed in compounding standards and skilled in the techniques required to prepare medications that are effective, safe, and high-quality. This continuing education program will review the importance of oral dosage forms, discuss United States Pharmacopeia standards for these dosage forms, and review techniques for preparing capsules, tablets, solutions, suspensions, and lozenges.
USP <795> Pharmaceutical Compounding - Nonsterile Preparations
Pharmaceutical compounding is considered both an art and a science and involves preparing medications tailored to an individual’s specific health needs.1 Compounded nonsterile preparations (CNSPs) encompass many different oral dosage forms, each with a specific purpose and associated patient benefits. Oral dosage forms enhance medication adherence, mask the bitter taste of active pharmaceutical ingredients (APIs), and protect APIs from degradation.1,2
The United States Pharmacopeia (USP) <795>, “Pharmaceutical Compounding, Nonsterile Preparations,” defines nonsterile compounding as combining, admixing, diluting, pooling, reconstituting other than as provided in the manufacturer’s labeling, or otherwise altering a drug product or bulk drug substance to create a nonsterile preparation.3 The chapter requirements are essential to minimize harm, including death, to human and animal patients that could result from the following:
Excessive microbial contamination3
Variability from the intended strength of correct ingredients3
Physical and chemical incompatibilities3
Chemical and physical contaminants3 and/or
Use of ingredients of inappropriate quality3
The scope of the chapter pertains to numerous CNSPs, including:
Solid oral preparations (such as capsules or tablets)3
Liquid oral preparations(such as solutions or suspensions)3
Rectal preparations3
Vaginal preparations3
Topical preparations (such as creams, gels, and ointments)3
Nasal and sinus preparations intended for local application (such as nasal sprays and nasal irrigation)3
Otic preparations (excluding use in perforated eardrums)3
Revised USP <795> reinforces that compounding personnel must demonstrate competency in the techniques required to prepare nonsterile oral dosage forms.3 This includes skills such as accurate weighing and measuring, particle size reduction, geometric dilution, and proper mixing.3 These competencies are essential when preparing capsules, tablets, solutions, and suspensions, where variability in technique can directly affect dose uniformity and product quality. Ongoing competency assessment helps ensure consistency and reduces the risk of compounding errors.3
The updated standards also emphasize clear and complete documentation of compounding procedures, which is particularly important for oral dosage forms.3 Compounding records should include formulation components, preparation steps, and any quality control checks performed.3 For preparations such as capsules and suspensions, documentation supports reproducibility and ensures that future batches are prepared consistently. Accurate records also help identify and correct potential sources of variability in technique.3
The Oral Route of Administration
The oral route is essential for administering numerous medications. In fact, oral medication delivery is the most common and preferred route for systemic and local drug delivery.4 Oral administration is one of two gastrointestinal routes of administration–the other being the rectal route.5 Anatomical routes for the systemic delivery of drugs are summarized in Table 1.5
Table 1
Anatomical Routes for the Systemic Delivery of Drugs5
| Gastrointestinal system |
| Oral |
| Rectal |
| Parenteral |
| Subcutaneous injection |
| Intramuscular injection |
| Intravenous injection |
| Intra-arterial injection |
| Transmucosal: buccal and through the mucosa lining the rest of the gastrointestinal tract |
| Transnasal |
| Pulmonary: drug delivery by inhalation |
| Intraosseous infusion |
Table 2 illustrates the differences in routes of administration. It compares the oral route to the intravenous route.5
Table 2
Comparison of the Oral and Intravenous Routes5
| Issue | Oral Route | Intravenous Route |
| Delivery to the blood circulation | Indirectly through the GI tract | Direct |
| Onset of action | Slow | Rapid |
| Bioavailability | Low to high | High |
| Dose control | Moderate | Good |
| Administration | Self | Health professional |
| Patient convenience | High | Low |
| Adverse effects | GI upset | Acute reactions |
| Use for peptides and proteins | No | Yes |
Administering medications orally has associated advantages and disadvantages. These should be considered when choosing this route of administration.
Advantages of the Oral Route of Administration
Benefits of this route include ease of administration, which may be the patient’s preferred method of taking the medication.5 However, this route is encumbered by numerous limitations, as noted below. Improvements in drug formulations have helped to overcome many of these issues.5
Disadvantages of the Oral Route of Administration
Variable absorption rates and sometimes unpredictable serum concentrations when drugs are used orally for systemic effects5
Potential for drug degradation in the digestive tract before they reach their intended site of absorption into the bloodstream5
The use of macromolecules is limited to the GI tract due to the inability to cross cells in the small intestine to reach the bloodstream5
Reduced bioavailability of some drugs when they become insoluble at the low pH in the GI tract5
Drug inactivation by the liver5
Some drugs irritate the mucous lining of the GI tract5
Compounding Techniques for Nonsterile Oral Dosage Forms
Compounding starts with understanding general compounding techniques. Additional compounding techniques are then applied to oral dosage forms: tablets, capsules, solutions, suspensions, and lozenges.
General Techniques
Compounding personnel should be familiar with general compounding techniques for particle-size reduction and mixing when formulating oral dosage forms. Perfecting these skills will help ensure that preparations are compounded accurately. Particle size reduction, also known as comminution, helps ensure that ingredients are within the same particle-size range, and various methods can achieve this.1 Manual methods of comminution are defined in Table 3.1 The method used will be dependent on the API characteristics.1
Table 3
Manual Comminution Methods1
| Term | Definition |
| Trituration | Grinding solids into a fine powder while simultaneously mixing |
| Levigation | Grinding an insoluble substance to a fine powder while wet |
| Pulverization by intervention | An intervening solvent is used to dissolve the compound, and this is mixed to enhance the evaporation of the solvent |
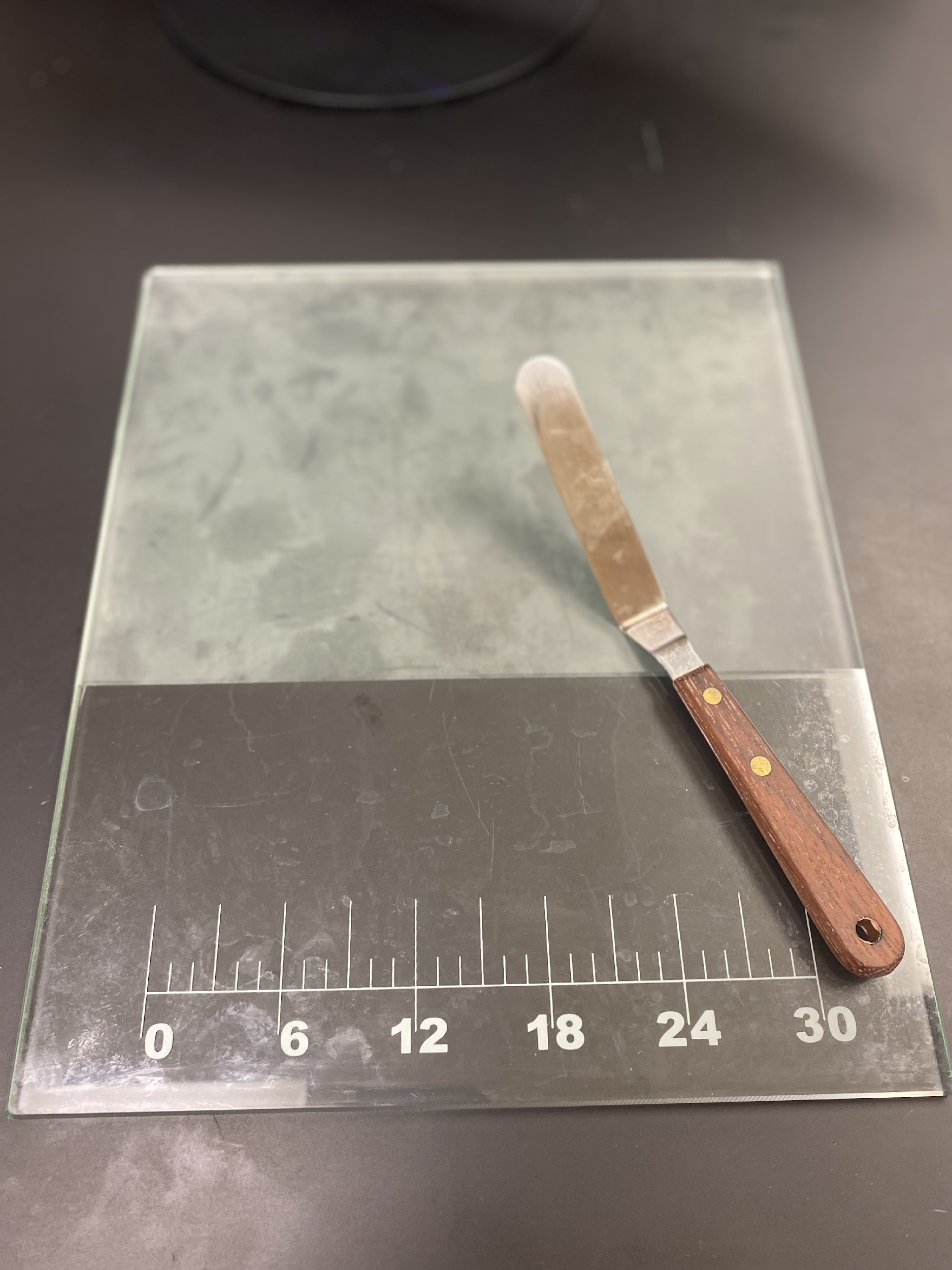
Understanding the methods for mixing the components of preparations is also vital, as this helps ensure homogeneity and even dose distribution.1 Geometric dilution is a manual mixing method that starts with the ingredient of the smallest quantity.1 Other ingredients are then added to the mixture in order of quantity required by doubling the portion being mixed each time.1 Ultimately, the primary objective in mixing ingredients is to achieve homogeneity in the final product, which is essential for optimal therapeutic outcomes. Equipment used to mix may include a mortar and pestle (Figure 1) or a pill tile with a spatula (Figure 2).
Figure 1
Mortar and Pestle

Figure 2
Pill Tile and Spatula
Tablets
Tablets are a common oral dosage form due to their stability and effectiveness.1 Components of tablets can include APIs and excipients such as diluents, binders, disintegrants, lubricants, coloring agents, and flavoring agents.1 The use of these excipients and others depends on the specific formulation used.1 Table 4 presents examples of these excipients.1
Table 4
Tablet Excipients1
| Excipient | Example | Purpose |
| Binders | Water, alcohol, starch paste | Hold powders together |
| Disintegrants | Cellulose derivatives and starch | Aid in tablet breakdown |
| Lubricants | PEG, starch, calcium stearate | Prevent sticking |
| Flavoring agents | Various flavors available | Mask the bitter taste of an API Improve patient adherence |
Tablets can be molded, sintered, or compressed.1 Tablet triturate molds used to compound tablets may be made of either plastic or metal, though metal molds are more common.1 These molds typically consist of two plates, one with pegs and the other with corresponding holes or cavities.1 Capacity determination is essential for each base type used; this involves creating tablets solely from the base, weighing the entire batch, and dividing the weight by the number of tablets to derive the average weight per tablet for that base.1
The active drug is mixed with a diluent, such as lactose or mannitol, as the base when preparing molded tablets.1 Lactose is often preferred.1 Once the tablet mixture is ready, the mass should be moistened and then pressed into the mold cavities using a spatula.1 The cavity plate can then be set on the peg plate, with pegs aligned.1 This is then allowed to drop, which pushes out the tablets.1 The tablets should be left to dry, and then can be removed and packaged.1
Capsules
Capsules are an alternative oral dosage form to tablets and can encapsulate powders, liquids, and semisolids.6 Compounding medications in capsule form can offer various benefits.1 First, many drugs are often bitter or unpleasant tasting, and capsules help mask or hide the taste of these medications.7,8 Additionally, compounding personnel can add numerous medications to one single capsule, which can assist patients in improving adherence to their medication therapies.7,8 Despite these benefits, capsules have a number of associated disadvantages, including their susceptibility to humidity and microbial contamination.7,8 Additionally, their use can potentially decrease adherence for individuals who have difficulty swallowing pills, such as geriatric and pediatric patients.7,8
Capsules are generally prepared as either hard or soft-shell capsules, each with a different purpose.6 Soft-shell capsules, also called softgels, may contain nonaqueous liquid or semisolid formulations.6 Ingredients in softgels include gelatin, water, and additives such as colorants.6 Hard capsules are two-piece shells that may be filled with powders, pellets, granules, non-aqueous solutions, suspensions, or semi-solids.6 The two components of the hard capsule include the base (or body) and the cap.6 The base is longer, has a small diameter, and holds the capsule contents.6 The cap is shorter with a slightly larger diameter and slides over the base to form a snug seal.6
Capsules are available in 8 sizes for human use. The smallest is size 5, and the largest is size 000.1 The sizes and associated volumes of capsules are detailed in Table 5 below.1
Table 5
Capsule Sizes1
| Capsule Size | Volume (mL) |
| 000 | 1.37 |
| 00 | 0.95 |
| 0 | 0.68 |
| 1 | 0.50 |
| 2 | 0.37 |
| 3 | 0.30 |
| 4 | 0.20 |
| 5 | 0.13 |
Compounding personnel can utilize the Rule of Sixes when filling hard-gelatin capsules to select an appropriate size.1 This is detailed in Table 6.1 Patient considerations, such as whether the patient can swallow a particular size capsule, should also be considered.1
Table 6
Rule of Sixes 1
| 1. | Set up six “6s” | 6 | 6 | 6 | 6 | 6 | 6 |
| 2. | List the capsule size | 0 | 1 | 2 | 3 | 4 | 5 |
| 3. | Subtract values in step 2 from those in step 1 to determine the average fill weight in grains | 6 | 5 | 4 | 3 | 2 | 1 |
| 4. | Convert fill weight to grams (1 grain = 0.065 g) | 0.390 | 0.325 | 0.260 | 0.195 | 0.130 | 0.065 |
| 5. | Determine fill volume in milliliters | 0.67 | 0.50 | 0.37 | 0.30 | 0.21 | 0.12 |
| 6. | Calculate and list average capsule fill density (divide weight values in step 4 by volume values in step 5) | 0.58 | 0.65 | 0.70 | 0.65 | 0.62 | 0.54 |
Two methods are widely used to prepare capsules: individual hand filling and capsule machine filling.1 Regardless of the selected method, compounding personnel must first determine the materials they will utilize to prepare and fill the capsules.1 Sources of APIs may include pure drug powders or can be obtained from manufactured tablets, capsules, or liquids.1 These are summarized in Table 7.
Table 7
Capsule Ingredients1
| Source | Considerations |
| Pure powder | The least amount of complications |
| Tablets | Need to be finely comminuted Cannot use controlled-release tablets |
| Capsules | Challenges with the use of closed capsules |
| Liquids | Evaporated to dryness first Soaked up with an absorbent first |
The first step of preparing powders for capsules involves accurately weighing and/or measuring each ingredient.1 In general, compounding personnel should aim to prepare an additional capsule or 5% to 10% more of the intended formulation.1 This extra quantity will help account for any potential loss of powder during the compounding process.1
After weighing and measuring, the next step is to reduce particle size. This is followed by sieving the mixture using mesh.1 The size utilized may range from Nos. 60 to 100, depending on the specific powders used.1 This process will further refine particle size.1 Powders can then be mixed using geometric dilution.
When hand-filling capsules, precise techniques will ensure accurate dosing and formulation integrity.1 The process begins by arranging the powder into a pile using a spatula, ensuring that the pile's thickness is approximately one-third the length of the capsule body.1 It is very important that direct contact between personnel’s hands and the powder is avoided while punching the capsules. Wearing gloves will minimize contact.1 During the filling process, the capsule should be pressed into the powder on the working surface while gently rotating to pack the powder evenly.1 A slight resistance will be sensed as the capsule is pressed through the powder, indicating it is full.1
After filling, the capsule's weight should be checked, and the powder amount should be adjusted as needed to achieve the desired weight.1 One issue that may occur during this process is a powder not adhering well within capsules during punching. This can be mitigated by placing the capsule base on its side and using a spatula to guide or fill the powder. It is important to avoid scraping or scratching the capsules during this process.1
Personnel can use automated capsule-filling machines as an alternative approach to hand-filling.1 During this process, empty gelatin capsules are inserted into the machine with the cap placed on top.1 The machine then separates the capsule base from the cap, and the part of the machine holding the caps is removed.1 The capsule bases will drop into position, aligning the top of the base with the working surface.1 Next, the powder mixture is spread evenly over the working surface, using a plastic scraper held perpendicular to the plate to allow the powder to fall naturally into the empty capsule bases by gravity.1 It is important not to push the powder into the capsule shells with the scraper, as this can lead to inconsistent quantities of powder in each shell.1 A specialized tamper is used to compress the powder in the shells.1 Before tamping, the excess powder is moved aside, and the tamper is applied to the cleaned area. The tamping process is repeated as needed until all capsules are filled evenly.1 Once capsules are filled, the part of the machine holding the caps is placed over the machine.1 The capsules are then capped and can be removed.1
After they have been prepared, capsules should be cleaned.1 This can be done by placing the capsules in a folded cloth or a container with sodium bicarbonate, sugar, or salt.1 The cloth or bag can then be gently rolled, passing the contents through a No. 10 sieve, which allows the salt but not the capsules to pass through.1
Solutions
Solutions are the most common liquid dosage form.1 They are defined as liquid preparations where one or more drug substances are dispersed at a molecular level in a suitable solvent or a blend of mutually miscible solvents.1 A solvent is a substance in which another substance dissolves. A miscible solvent is one with which another liquid can be mixed without separation.
Some of the common reasons for preparing a compound in an oral liquid dosage form include the following:1
The drug product is not commercially available as an oral liquid
Different patient populations, including infants, pediatric, and geriatric patients, cannot swallow solid dosage forms
Some products are therapeutically better in liquid form
Patients receiving enteral feedings require a liquid dosage form
Oral liquid dosage forms are diverse and have varying dosage strengths
When preparing an oral liquid dosage form, compounding personnel may need to decide whether to prepare a solution or a similar dosage form, such as a suspension. The following are key considerations in this decision process:
Any physical and chemical properties of the ingredients
The order of mixing
The required pharmaceutical compounding techniques
Any incompatibilities in preparation and storage
The complexity of a solution's composition can vary widely and depends on factors such as the APIs used, the intended use of the preparation, patient characteristics, and storage conditions.1 Formulations used to prepare solutions typically consist of the API and excipients such as cosolvent systems, flavorings, sweeteners, colorings, preservatives, buffering agents, antioxidants, or other additives.1 When choosing a solvent, it is recommended to use official solvents listed in the United States Pharmacopeia/National Formulary (USP-NF). Compounding personnel should also remember that polar solutes will dissolve in polar solvents, and nonpolar solvents should be used to dissolve nonpolar solutes.1
When preparing a solution, the pH range is an important consideration. It can affect a drug’s solubility, activity, absorption, and stability.1 Certain drugs will precipitate in the solution when the pH falls outside the intended range.1 Additionally, the stability of many APIs will depend on the pH of the dosage form.1
Selecting the appropriate vehicle for the solution is also a key consideration.1 Various vehicles can be used to prepare oral solutions, with ethanol, glycerin, syrups, and water being among the most common.1 Water is a common solvent, and personnel can reference USP/NF for many types of water, including pharmaceutical waters.1
Various techniques are employed in preparing oral solutions. A simple solution is most commonly prepared by dissolving a drug in a solvent.1 This process may only require stirring, but other times, heat or agitation may be required for the solution to form. Tips and tricks for compounding solutions are detailed in Table 8.1
Table 8
Tips to Compound Solutions1
| Stir preparations gently to avoid foaming |
| Magnetic stirrers and blenders can be used to save time and help to prepare homogeneous preparations |
| Do not use a stirring rod when adding “sufficient volume” of a solvent to a graduate in which you are preparing the solution |
| Liquid filtration can help to produce a clear preparation |
| Always know the pH and alcohol concentrations of preparations you are compounding |
| Preservative effectiveness can be related to pH |
| Dissolve salts in small quantities of water before adding the viscous vehicle |
| When combining two liquids, stir the mixture constantly to decrease the chance of incompatibilities resulting from concentration effects |
Suspensions
Suspensions are valuable dosage forms that enhance the stability of drugs that are unstable in solution.1 This dosage form is defined as a two-phased system consisting of finely divided solids dispersed in a solid, liquid, or gas.1 When a good suspension has been compounded, the APIs will be uniformly dispersed in the vehicle. Suspension formulations typically contain insoluble particles, a liquid medium, a surfactant or viscosity enhancer, and a preservative.1 The sequence in which these components are combined significantly impacts the stability of the final preparation.1
Compounding a suspension begins with achieving uniform, fine particles of the drug.1 Once particle size reduction is accomplished, it is crucial to thoroughly wet the API before blending it with the vehicle.1 Hydrophilic materials are effectively wetted using water-miscible liquids like glycerin, while hydrophobic substances can be wetted using nonpolar liquids or surfactants.1 It is considered best practice to use the smallest amount of wetting agent necessary. Once the drug and wetting agent have been mixed to form a thick paste, the vehicle is added while stirring continuously.1
Viscosity is key to keeping APIs in suspension, and viscosity-increasing agents are best dispersed by gradually adding the powder into vigorously stirred water, maintaining stirring throughout hydration.1 Alternatively, these agents can be mixed with a water-soluble substance like sucrose before incorporation into water or formed into a paste with a water-miscible liquid before addition to water.1 Some agents may require initial dispersion in hot water followed by the addition of cold or ice water to minimize clumping, especially with polymers that tend to clump and complicate the preparation process.1 These methods contribute to the successful formulation of stable and well-dispersed suspensions.1 Compounding personnel should also observe suspensions for resuspendability, and these preparations should be observed to determine if they have caking tendencies.1 Further, suspensions should not be too thick, as this can affect the pourability of the preparation.1
Lozenges
Lozenges are useful for systemic and local effects. While some lozenges dissolve slowly in the mouth, others can be chewed and swallowed. They typically contain the API and a flavoring component.1 It is important that ingredients utilized within compounded lozenges are heat-stable.1 Various types of lozenges may be prepared, including hard lozenges, soft lozenges, and chewable lozenges.1 Hard lozenges have firm candy bases derived from sugar and syrup and frequently incorporate adhesive agents like acacia.1 Soft lozenges typically rely on a polyethylene glycol (PEG) base, while chewable varieties utilize a glycerinated gelatin base.1
The preparation of lozenges involves molding a carbohydrate mixture into hard candies, forming a soft lozenge matrix, or molding a gelatin base into a chewable mass.1 Each method has its associated process.
Hard lozenges, sugar, and other components are heated to the appropriate temperature, poured into molds, or pulled into ribbons as they cool, then cut to the desired lengths.1 Alternatively, they can be compressed into very hard tablets using commercial methods.1
Figure 3
Lozenge Mold
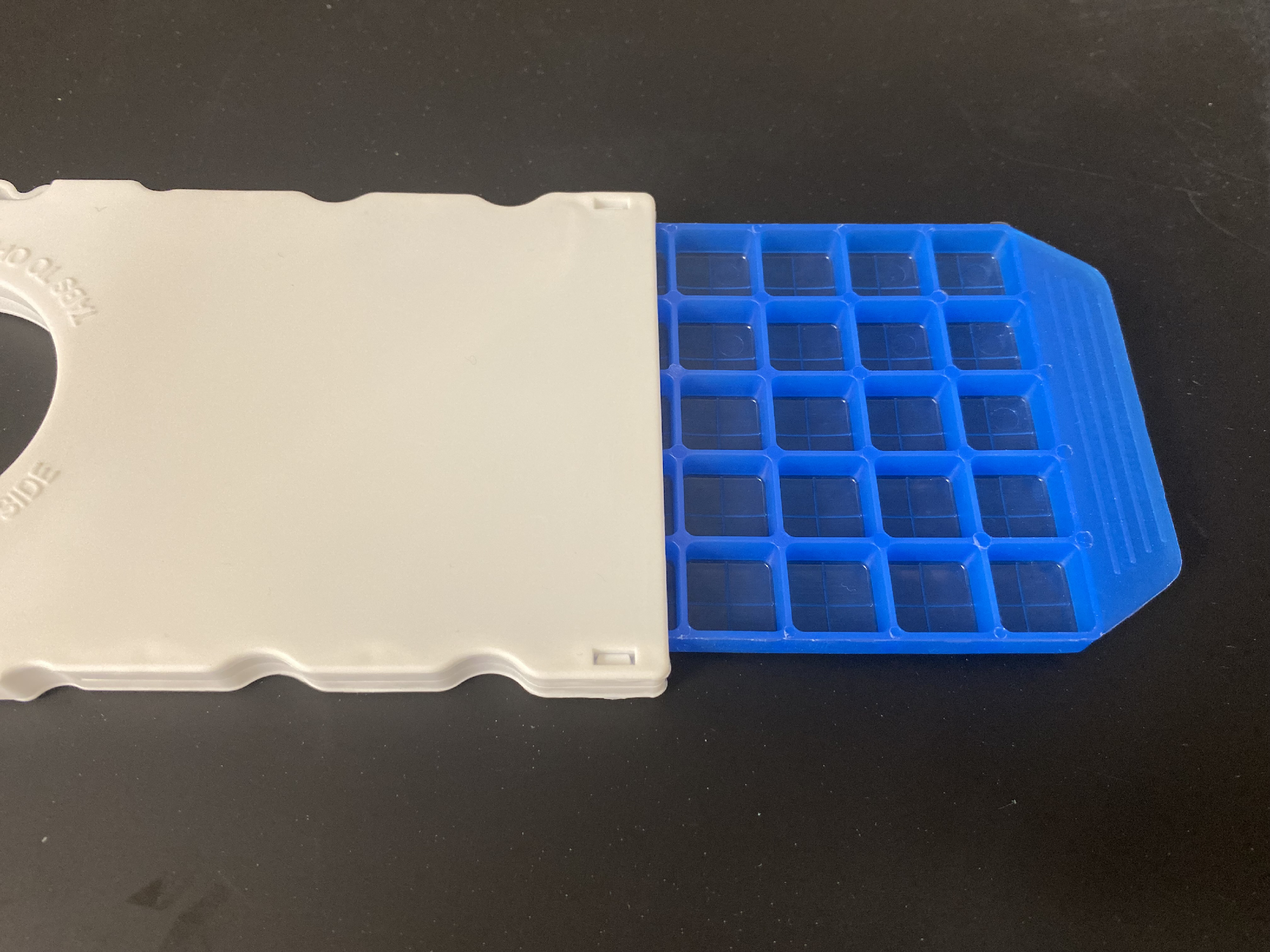
Soft, chewable lozenges are prepared using molds depicted in Figure 3, which require calibration to determine the weight of each lozenge based on the specific base used.1 This calibration involves melting the lozenge base, pouring it into molds, cooling the blank lozenges, weighing them, and then calculating the average weight per lozenge.1 Another method involves pouring the lozenge mixture onto the work surface to form a sheet of even thickness, then punching out the lozenges.1
Flavoring agents are crucial components of lozenges. They are typically added at a higher concentration than in regular candies to mask the medication's flavor.1 If the flavoring agent is not miscible with the base, it can be dissolved in glycerin before incorporation into the preparation.1 The same technique applies to incorporating oily drugs into lozenges when using a solvent technique.1
Quality Control and Storage
USP <795> highlights the importance of performing appropriate quality control checks for compounded preparations.3 For oral dosage forms, this includes assessments such as weight uniformity for capsules and tablets, and evaluation of appearance, pH, and dispersibility for liquid preparations.1 These checks help confirm that the preparation meets expected standards for consistency and performance, which is critical for ensuring accurate dosing and therapeutic effectiveness.
The revised chapter emphasizes the use of appropriate and high-quality components in compounding.3 For oral dosage forms, this includes selecting active pharmaceutical ingredients (APIs) and excipients that are compatible with the formulation and suitable for oral administration.3 Ingredients should meet USP–NF standards when available, and their selection should support stability, palatability, and proper drug release.3
Table 9 summarizes quality control procedures for capsules, tablets, solutions, suspensions, and lozenges, and Table 10 details storage recommendations for these dosage forms.1
Table 9
Quality Control Procedures1
| Dosage Form | Procedure for Quality Control |
| Capsules |
|
| Tablets |
|
| Solutions |
|
| Suspensions |
|
| Lozenges |
|
Table 10
Storage Recommendations1
| Dosage Form | Recommendation |
| Capsules |
|
| Tablets |
|
| Solutions |
|
| Suspensions |
|
| Lozenges |
|
The Role of the Pharmacy Technician
Nonsterile compounding is a specialized skill for pharmacy technicians. They can assist in preparing safe, high-quality, and effective compounds by utilizing skills in weighing, mixing, and measuring, as well as techniques specific to each dosage form. Pharmacy technicians can also assist pharmacists in determining if a patient has experienced any issues with their compounded medications. Useful resources pertaining to the topic include the Art, Science, and Technology of Pharmaceutical Compounding, The International Journal of Pharmaceutical Compounding, and USP <795> - Pharmaceutical Compounding - Nonsterile Preparations.
Summary
Compounding nonsterile preparations encompasses a variety of dosage forms, each with a specific purpose and associated patient benefits. Compounding personnel, including pharmacists and pharmacy technicians, should be skilled in preparing various dosage forms to produce safe, high-quality, and effective medications. This includes skills needed to prepare tablets, capsules, solutions, suspensions, and lozenges.
References
Allen, Lloyd. The Art, Science, and Technology of Pharmaceutical Compounding, 6th Edition. APhA. October 2020.
Carvalho M, Almeida IF. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals (Basel). 2022;15(9):1091. Published 2022 Aug 31. doi:10.3390/ph15091091
General Chapter: USP. Pharmaceutical Compounding - Nonsterile Preparations <795>. In: USP–NF. Rockville, MD: USP; Dec 1, 2020
Lou J, Duan H, Qin Q, et al. Advances in Oral Drug Delivery Systems: Challenges and Opportunities. Pharmaceutics. 2023;15(2):484. Published 2023 Feb 1. doi:10.3390/pharmaceutics15020484
Jain KK. An Overview of Drug Delivery Systems. Methods Mol Biol. 2020;2059:1-54. doi:10.1007/978-1-4939-9798-5_1
Gullapalli RP, Mazzitelli CL. Gelatin and Non-Gelatin Capsule Dosage Forms. J Pharm Sci. 2017;106(6):1453-1465. doi:10.1016/j.xphs.2017.02.006
Thompson J. A practical guide to contemporary pharmacy practice. 2nd Edition. Lippincott Williams and Wilkins. 2004.
Capsules. Pharmaceutics and Pharmaceutical Compounding Laboratory. Accessed April 14, 2026. https://pharmlabs.unc.edu/labexercises/compounding/capsules
DISCLAIMER
The information provided in this course is general in nature, and it is designed solely to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals must consult their employer, healthcare facility, hospital, or other organization for guidelines, protocols, and procedures to follow. The information provided in this course does not replace those guidelines, protocols, and procedures, but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses is constantly changing. Any person taking this course understands that such a person must make an independent review of medication information before any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course or course material.
© RxCe.com LLC 2026: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
RxCe.com
© RxCe.com LLC 2025: All rights reserved.