MEASLES: A RENEWED THREAT
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and currently licensed pharmacist in 3 states. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Topic Overview
Measles is one of the most contagious viral infections. It is spread through airborne droplets or direct inoculation through the nose, mouth, or eyes after touching an infected surface. Measles was declared eliminated in the USA in 2000 due to a very high percentage of people receiving the safe and effective measles-mumps-rubella (MMR) vaccine. The Center for Disease Control and Prevention (CDC) issued a nationwide alert in April 2024. Measles activity in the USA and globally is increasing while MMR vaccination has decreased. As of May 2024, a total of 142 measles cases were reported by 21 jurisdictions. This places the public at high risk for a measles outbreak. Measles can cause pneumonia, ear and upper airway infection, pain and sores in the mouth, and diarrhea. Rare but serious neurologic complications include swelling of the brain and spinal cord or progressive neurologic disorders that develop weeks to years after measles infection. Approximately 1 to 3 per 1000 people infected with measles die from respiratory or neurologic complications. Pharmacy teams are well-positioned to educate the public regarding prevention strategies and provide vaccination recommendations.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-073-H01-P
Pharmacy Technician 0669-0000-24-074-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Course Test and course evaluation
Release Date: June 18, 2024 Expiration Date: June 18, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians
How to Earn Credit: From June 18, 2024, through June 18, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Describe the seriousness of measles
Explain why measles activity is increasing
Prepare strategies to protect the public from measles
Disclosures
The following individuals were involved in developing this activity: Pamela Sardo, PharmD, BS. Pamela Sardo has no conflicts of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Measles: A Renewed Threat Introduction
Measles is a highly contagious, potentially fatal viral infection. It is preventable through vaccination, and as a result of vaccination, measles was declared eliminated in the USA in 2000. However, measles vaccination rates decreased largely due to the COVID-19 pandemic and a rise in vaccine hesitancy. The Centers for Disease Control and Prevention (CDC) issued a nationwide alert because of the rise in measles cases. Pharmacists and pharmacy staff are on the front lines regarding measles vaccinations. They should be prepared to address vaccine hesitancy in patients to help increase measles vaccination rates and return the US to the situation when measles was eliminated.
What is Measles?
Measles is a highly contagious disease that results from infection with the measles morbillivirus, also called the measles virus.1,2 Early references to measles can be found during the 7th century. In the 10th century, Persian physician Rhazes described the disease as “more to be dreaded than smallpox.”1
From 2000–2017, the number of measles cases reported globally fell by 80% (from 853,479 in 2000 to 173,330 in 2017).3 This was due to increased vaccination rates during these years, which were boosted by the Global Vaccine Action Plan, initiated in 2012.3 The annual incidence of measles also decreased by 83%, from 145 to 25 cases per million population, and measles deaths decreased by 80% (545,174 to 109,638).3 Based on these statistics, measles vaccinations prevented an estimated 21.1 million deaths globally during this period (2000–2017).3
The measles virus is transmitted by the respiratory route, and illness begins with fever, cough, coryza (inflammation of nasal mucus membranes), and conjunctivitis, the classic three C’s.4 This can be followed by a characteristic rash, Koplik’s spots, that spreads cephalocaudally.4 Cephalocaudal spread occurs along the body's long axis, from the head downward. Using the word cephalocaudal to describe the fourth symptom has led some scholars to refer to the symptoms as the four C’s: cough, coryza, conjunctivitis, and cephalocaudal spread.5
Small white spots typically appear on the inside of the cheek two to three days before the rash starts.6 The measles rash consists of flat red spots that spread from the head to the lower extremities.6 It can be contagious over four days before to four days after the rash appears.6 The virus is spread through airborne droplets or direct inoculation through the nose, mouth, or eyes after touching an infected surface.6
Measles is most commonly diagnosed by identifying the virus in throat or nasopharyngeal swabs, saliva, or urine using a laboratory test that identifies genetic material in a sample.6 The primary site of infection is alveolar macrophages or dendritic cells.1 Two to three days after replication in the lung, the measles virus spreads to regional lymphoid tissues, followed by a systemic infection.1 Following further viral replication, a second viremia occurs 5 to 7 days after initial infection. During this phase, infected cells migrate into the subepithelial cell layer and transmit measles to epithelial cells. The virus is then released into the respiratory tract.1 Figure 1 below is an image of a measles rash.
Complications of Measles
Suspected measles cases should be reported to the local health department, so contact tracing can occur.7 Complications of measles can affect most organ systems, with pneumonia accounting for most measles-associated morbidity and mortality.5 Measles can also cause ear and upper airway infection, pain, sores in the mouth, and diarrhea.8 Rare but serious neurologic
complications include swelling of the brain and spinal cord or progressive neurologic disorders that develop weeks to years after measles infection.9 Approximately 30% of measles cases in the United States (USA) from 1987 to 2000 were reported to have one or more complications.1 Approximately 1 to 3 per 1000 people infected with measles die from respiratory or neurologic complications.8

Figure 1 Measles Rash
People at the highest risk of developing complications from measles include unvaccinated individuals younger than 5 years or older than 20 years.6 Additional populations at risk include those who are immunocompromised or pregnant. Measles acquired during pregnancy can result in preterm labor and low infant birth weight.6
Centers for Disease Control and Prevention Alert
Measles was declared eliminated in the USA in 2000 due to a very high percentage of people receiving the safe and effective MMR vaccine.8 After 2017, measles vaccination rates decreased largely due to the COVID-19 pandemic. During the pandemic, public health efforts focused on vaccinating for the SARS-CoV-2 virus, and other health issues, such as measles
vaccinations, were not as vigorously pursued as in past years.10 There was also a rise in vaccine hesitancy.
As a result, the CDC issued a nationwide alert in 2024 warning of the increasing number of measles cases in the USA and globally.11 In the alert, the CDC reported that measles-mumps-rubella vaccination (M-M-R II, abbreviated as MMR in this course) had decreased.12 Vaccination coverage has been decreasing since the start of the COVID-19 pandemic.
Since measles is still common in many countries, travelers will continue to bring this disease into the United States. As of May 2024, 142 measles cases were reported in 21 jurisdictions, including Arizona, California, Florida, Georgia, Illinois, Indiana, Louisiana, Maryland, Michigan, Minnesota, Missouri, New Jersey, New York City, New York State, Ohio, Pennsylvania, Vermont, Virginia, Washington, West Virginia, and Wisconsin.8 Fifty-five percent of cases were hospitalized for isolation or management of measles complications.8
The U.S. MMR protective coverage among kindergarteners is below the
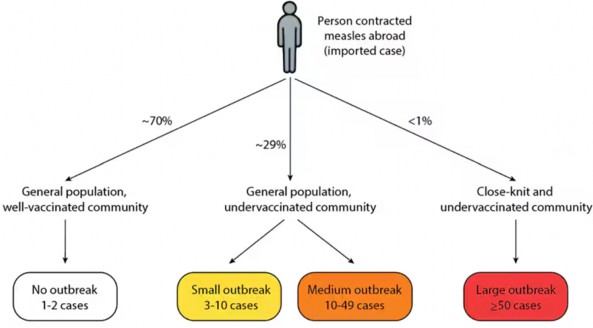
95 percent coverage target.12 It is much lower in some communities and continues to decrease.12 Measles could become endemic (defined as the constant presence of a disease in an area) again, especially if vaccine coverage levels drop. For example, 70% of international measles importations did not lead to outbreaks in a well-vaccinated setting.12 If a person who acquired measles abroad returns to a close-knit and under-vaccinated community with a high population density, a large outbreak is likely. From 2001-2023, 88% of outbreaks larger than 50 cases have occurred within these settings.12 Figure
2 describes measles outbreaks among different populations from diverse regions and the possible resulting spread. For example, from 2001-2023, 70% of international measles importations did not lead to outbreaks (but only 1-2 cases) because the population was well-vaccinated.
Figure 2
Published Measles Outbreak Among Different Coverage of Populations12
Measles Prevention
Urgent efforts are needed to increase vaccination and reduce morbidity and mortality from measles infection.2,5 Actions include supporting coverage with two doses of measles vaccine through advocacy, education, and emphasizing routine immunization.
A historical formulation of the measles vaccine incorporated a ‘killed’ measles virus. Individuals who received the prior formulation should talk to their healthcare provider about getting revaccinated with the current, live MMR vaccine.13 The killed vaccine was given to less than 1 million people between 1963 and 1967.13 Most people do not know if they got the killed vaccine during this time. If a patient is unsure whether they fall into this group, they should first find their vaccination records or obtain documentation of measles immunity.13 If written documentation of measles immunity is
unavailable or unknown, the patient should get vaccinated with the MMR vaccine. Experts recommend adults born in 1957 or later without evidence of immunity against measles should receive another dose of MMR.6,13 An additional option is to have a healthcare provider test the patient’s blood to determine whether the patient is immune, but this is generally not recommended.13
The more unvaccinated children in a school, the higher the chance of a measles outbreak within that school, and the larger that outbreak could be.12 This puts children who are unvaccinated for medical reasons, or unvaccinated due to household members who are immunocompromised, or babies who are too young to be vaccinated at risk of measles and its complications.12
Intentionally delaying vaccination until older is not recommended. Researchers have published that children vaccinated outside the recommended ages have a higher chance of adverse reactions, such as seizures or fatigue.14,15 One study found that the higher chance of adverse reactions was limited to a delay in the second MMR vaccine dose, not the first.16 This is an off-label use; however, sometimes, a vaccine may need to be administered outside the recommended age if a patient was not vaccinated under the schedule, for international travel, or outbreak control. The vaccine may also need to be administered to adults lacking proof of immunity. Healthcare workers, military, immigrants, travelers, and others at higher risk may also require vaccination outside the routine schedule.16
Refusing or intentionally delaying vaccination creates a substantial public health burden, including strain on medical facilities, doctors, nurses, pharmacy teams, and local health departments.12 Table 1 shows different levels of MMR coverage and the chance of an outbreak within a school sample of 100 children, starting with one infectious child potentially exposing others.
Table 1
Published Chance of an Outbreak Based on MMR Coverage13
| MMR Coverage | Number of children susceptible | Chance of an outbreak |
| 97% | 6 | 16% |
| 93% | 10 | 36% |
| 80% | 22 | 64% |
| 70% | 32 | 78% |
A single dose is approximately 0.5 ml.17 It can be administered subcutaneously or intramuscularly. The first dose should be administered at ages 12 to 15 months. The second dose administration should be at ages 4 to 6 years.6,17 All children should receive two doses of MMR vaccine.6,17 College and university students without prior measles vaccination or infection should receive 2 doses of MMR vaccine, spaced at least 28 days apart.6
Detectable antibodies generally appear within just a few days after vaccination. People are usually fully protected after about 2 or 3 weeks. If pharmacy personnel become aware of patients traveling internationally, advise them to ensure they are immunized against measles. Patients should plan to be fully vaccinated at least 2 weeks before departure. If travel is less than 2 weeks away and they are not yet immunized, they will not be fully protected against measles but should still get a dose of the measles vaccine.13
Safety
Reported side effects include injection site reactions, erythema, pain, and swelling.17 Systemic side effects include measles-like rash or fever.17 Headache, dizziness, vasculitis, arthralgia, and sore throat have been reported.17
The MMR vaccine is contraindicated in individuals with hypersensitivity to any vaccine component or if immunosuppressed.17 It is also contraindicated if moderate or severe febrile illness is present and in individuals with active untreated tuberculosis and pregnancy.17 Warnings and precautions have been reported, including anaphylactic hypersensitivity to eggs and transient thrombocytopenia. Immune globulins (IG) and transfusions should not be given concurrently with MMR vaccination.17 The prescribing information should be reviewed for comprehensive safety and efficacy information.
The risk of serious adverse events is low. Around one out of every million doses of the MMR vaccine can cause a life-threatening allergic reaction.18 Allergic reactions should be reported to the Vaccine Adverse Event Reporting System (VAERS).19 The government has a program to compensate individuals whose injuries are scientifically determined to result from vaccines, including MMR.20 This program is named the National Vaccine Injury Compensation Program (VICP).20
Patient Discussion Points:12,16-20
Provide required vaccine information to patients, parents, or guardians
Inform of the vaccination benefits and risks
Instruct individuals to report any adverse reactions
The Vaccine Adverse Event Reporting System (VAERS) accepts all reports of suspected adverse events (1-800-822-7967 or https://www.vaers.hhs.gov)
Inquire about reactions to any previous dose of MMR vaccine
Question females of reproductive potential regarding the possibility of pregnancy
Two doses of MMR vaccine provide better protection against measles than one dose: two doses of MMR vaccine are about 97% effective at preventing measles; one dose is about 93% effective.
Measles is extremely infectious and can cause life-threatening illness. Anyone who is not protected against measles is at risk.
Parents should get their children vaccinated on schedule with MMR vaccine
Teens and adults should check with their providers to make sure they are protected against measles
International travel: Published recommendations are that people 6 months and older should be protected against measles before leaving for international trips
Infants under 12 months old who are traveling internationally should get an early dose at 6 through 11 months, then follow the recommended schedule for doses. This is an off-label use
People 12 months and older should receive 2 doses before travel
Monitor health for 3 weeks after returning from travel
If a rash and fever develops, the healthcare provider should be contacted
Case Reports
Case Report # 1
In 2021, Operation Allies Welcome (OAW) was established to support the resettlement of more than 80,000 Afghan evacuees into the USA.21 Mass measles vaccination of evacuees aged 6 months or older was introduced domestically and overseas, with a 21-day quarantine period after vaccination.21 Forty-seven people with measles (attack rate: 0·65 per 1000 evacuees) were reported in six US locations housing evacuees in four states. The median age of patients was 1 year (range 0–26); 33 (70%) were younger than 5 years.21 The rapid implementation of control measures successfully
curbed measles virus transmission after arrival to the USA.21 First, the decision to pause evacuee flights from overseas locations allowed for mass vaccination while population immunity was building among evacuees. Second, the high MMR vaccine coverage was achieved within 3 weeks of identifying the first case, limiting the spread among evacuees.21 This highlights the importance of communication, collaboration, and quick action.
ACTIVE LEARNING PAUSE: QUESTION 1
What were some causes of the actions taken in this case?
ACTIVE LEARNING PAUSE: ANSWER
Measles is very contagious
Identification of measles in this resettled population with low measles vaccination coverage
Living in close proximity demanded immediate public health action
Case Report # 2
Patient L.N. had a positive pregnancy test and, one week later, had a fever of 101.4 degrees Fahrenheit, runny nose, and cough.22 A few days later, she developed a rash on her face, sores in her mouth, and diarrhea.22 She contacted her healthcare provider. A laboratory confirmed a diagnosis of measles.22 L.N. was advised to take acetaminophen or ibuprofen, stay hydrated, and self-isolate on bed rest.22 L.N. shared that her parents had declined all immunizations when she was young due to religious beliefs. The provider reported the measles to the local health department.22 L.N. felt very ill for about 7 days. Her pregnancy proceeded normally after her recovery.
L.N. told the healthcare provider the infant would receive vaccines at the recommended times.22
ACTIVE LEARNING PAUSE: QUESTION 2
Why did the provider report measles to the local health department?
ACTIVE LEARNING PAUSE: ANSWER
Measles is extremely contagious
Contact tracing is important to find and isolate the source, if possible
Anyone in direct contact with the patient is exposed
Isolation of exposed persons should occur
Reporting is a reminder to undertake early treatment of cases
Reporting may result in a public health announcement to vaccinate
Management of Measles
Management of measles is mostly supportive. There are no proven effective antiviral treatments for measles.6 Infected individuals should be isolated and monitored closely for complications. The CDC recommends vitamin A supplementation for children hospitalized with measles.6 Some authors recommend that adults should also receive vitamin A.2,5,23 The recommended administration is vitamin A once daily for 2 days, at the following doses:23
Children 12 months of age or older: 200,000 IU
Infants 6–11 months of age: 100,000 IU
Infants < 6 months: 50,000 IU
If vitamin A deficiency is likely present, another dose is recommended 4–6 weeks after the onset of the acute infection.
Precautions are in place to protect healthcare practitioners treating a patient with suspected or confirmed measles.24 If a patient believes they have measles or have been exposed to someone with measles, isolate them from others and call a healthcare provider, urgent care, or emergency room before arriving to be tested.12 Do not arrive at a healthcare facility without giving advance notice.12
Place a surgical mask on the patient immediately.24 In a medical center, place the patient in Airborne Precautions.24 This means ensuring anyone entering the room (regardless of measles immunity) wears a fit-tested N-95 respirator or powered air purifying respirator (PAPR).24 Place the patient in a negative pressure room.23 If none is available, place the individual in a regular patient room and contact infection prevention staff. Clean hands before and after entering. Only remove the respirator after exiting the room and shutting the door.24
Usual isolation room cleaning is fine, but the room must remain vacant for 2 hours after the patient leaves. After waiting 2 hours, the staff may proceed with room cleaning using the protocol for isolation patients. Infectious skin lesions should be covered if transporting the patient.24
Most people born before 1957 were exposed to at least two major measles outbreaks, which conferred immunity.25 Once a person has had the measles, they are presumed to be immune for life. Individuals who received the vaccine between 1963 and 1967 are the exception.25 People without previous measles vaccination or infection should receive the MMR vaccine within 72 hours or immunoglobulin (derived from donated blood that contains antibodies to measles) within 6 days of exposure to a patient with measles.6
Barriers to Measles Vaccination
Despite the efficacy and safety record of the MMR, measles-vaccine hesitancy persists.26 Understanding the reasons for vaccine hesitancy can help the clinician address and eliminate the barriers. Barriers to measles vaccination include the following:26
Fear of autism
Philosophical, moral, and religious objections
Ethnicity
Income and education levels
Healthcare access
Tips for Navigating Hesitancy
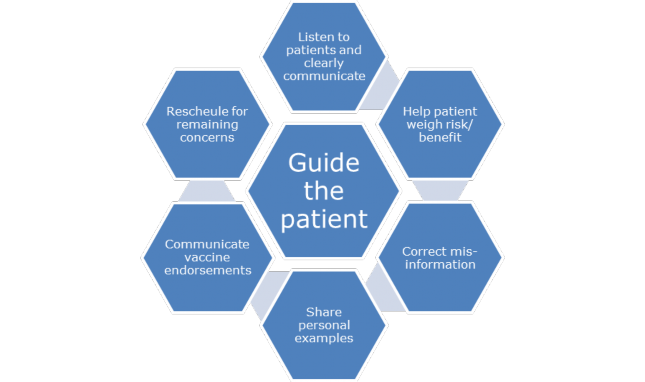
Pharmacy teams can guide the patient along the vaccine hesitancy continuum, even if not ultimately successful. The conversation is valuable. During a vaccine discussion with a parent, the clinician should first identify the cause of parental hesitancy. Once the parent’s concerns have been identified, discussions can be held to address them. Be a good listener. Communicate clearly and in a personalized manner. Avoid jargon. Help the patient weigh the risks and benefits and explain the mild side effects and the low risk of serious adverse events. Accept questions and gently correct misinformation. For example, articles and presentations exist that attempt to tie MMR vaccines to autism. Patients often lack an understanding of the type or quality of the articles and presentations. This can lead to a long-lasting belief in false information. Share personal experiences, fact sheets, or resources. Communicate vaccine endorsements by communities or experts. Refer to or schedule another appointment to address the remaining concerns. Figure 3 illustrates conversation considerations for vaccine hesitancy.
Figure 3
Vaccine Hesitancy Discussion Opportunities26
What’s Next?
In recent years, vaccine hesitancy to MMR clustered in middle- to high- income areas among mothers with a college-level education or higher who preferred internet/social media narratives over physician-based vaccine information.23,24 They had low parental trust, low perceived disease susceptibility, and were skeptical of vaccine safety and benefits.26,27 Combating MMR vaccine misinformation and hesitancy requires ongoing individualized, multifaceted approaches at various socio-ecological levels to address the social drivers of vaccine behavior.
Pharmacy personnel are well-positioned to nurture trust among parents, physicians, and government sectors to dispel myths and doubts about the benefits and safety of vaccines.26,27 Healthcare providers and public health
practitioners can explore innovative and culturally appropriate communication regardless of vaccine beliefs. Engaging parents in safe and nonjudgmental discussions is vital in effectively tackling vaccine misinformation and hesitancy. Combining the science with understanding parental sentiments could enable conversations among those with lingering concerns.26 Using messages tailored to specific issues may improve vaccination rates among traditionally hesitant populations.26
Ongoing research, including the development of point-of-care diagnostics and microneedle patches, is being studied to facilitate progress toward measles elimination and eradication.5
Summary
Pharmacy teams must prepare for questions about measles and the MMR vaccine. They should remain aware of measles alerts impacting public health. Pharmacists should have strategies for discussing prevention and mitigating vaccine hesitancy. Pharmacy teams are prepared to educate and support patient management with vaccination. Information about vaccine safety and efficacy and educating patients about the benefits of vaccination and non-vaccination risks have been shown as effective strategies.
Course Test
Place the signs and symptoms of measles in the order they appear or present.
Pneumonia, ear infection, rash on torso, cephalocaudal spread
Flat red spots on the head, rash on torso and lower, white spots in cheek
White spots in cheek, flat red spots on the head, rash on torso and lower
Swelling of the brain after international travel, cephalocaudal spread
Which option below is a complication of measles?
Pneumonia
Toothache
Constipation
Deviated septum
Which of the following can result when a mother acquires measles during pregnancy?
Mandatory C-section to prevent exposure to the OB-GYN provider
During delivery, shoulders became stuck in the birth canal
Delayed labor and large birth weight
Preterm labor and low infant birth weight
Which population group below is at the highest risk for complications from measles?
Native American Indians with type 1 or type 2 diabetes
Vaccinated individuals younger than 5 years and older than 20 years
Unvaccinated individuals younger than 5 years or older than 20 years
Asian Americans with genetic susceptibility to measles
In 2024, the CDC reported an increase in measles cases in the US and worldwide. Which of the following is a reason for this increase in measles cases?
County fairs were implicated
Airplane air filters were found to be insufficient
MMR vaccination has been increasing
MMR vaccination has been decreasing
How many doses of measles vaccine are recommended for children to protect them optimally against measles?
a. 1
b. 2
c. 3
d. 4
At what age should the first MMR vaccine dose normally be administered?
6 to 9 months
9 to 11 months
12 to 15 months
20 to 24 months
Are there any special cleaning requirements for a room where a suspected or confirmed measles patient has resided?
There are no special recommendations for cleaning a room that housed a confirmed measles patient
After waiting 2 minutes, the staff may proceed with room cleaning using the protocol for isolation
After waiting 2 hours, the staff may proceed with room cleaning using the protocol for isolation
After waiting 2 days, the staff may proceed with room cleaning using the protocol for isolation
What is a staff precaution in a facility that can minimize the risk of exposure to measles?
Staff entering the room must wear an N-59 respirator or PREP
Staff entering the room must wear an N-95 respirator or PAPR
Place a surgical mask on the patient within 10 minutes of arrival
Place a surgical mask on the patient if they are coughing
The four ‘Cs’ of measles comprise the following symptoms:
cough, conjunctivitis, coryza, cephalocaudal spread
childhood, cough, cataracts, cartilage changes
childhood, coaxial spread, constipation, cartilage changes
conjunctivitis, coryza, coaxial spread, constipation
References
Gastanaduy P, Haber P, Rota P, Patel M. Chapter 13: Measles. CDC. August 18, 2021. https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html. Accessed May 24, 2024.
Hübschen JM, Gouandjika-Vasilache I, Dina J. Measles. Lancet.
2022;399(10325):678-690. doi:10.1016/S0140-6736(21)02004-3
Dabbagh A, Laws RL, Steulet C, et al. Progress Toward Regional Measles Elimination - Worldwide, 2000-2017. MMWR Morb Mortal Wkly Rep. 2018;67(47):1323-1329. Published 2018 Nov 30.
doi:10.15585/mmwr.mm6747a6
Vassantachart JM, Yeo AH, Vassantachart AY, Jacob SE, Golkar L. Art of prevention: The importance of measles recognition and vaccination. Int J Womens Dermatol. 2019;6(2):89-93. Published 2019 Jul 8. doi:10.1016/j.ijwd.2019.06.031
Moss WJ. Measles. Lancet. 2017;390(10111):2490-2502. doi:10.1016/S0140-6736(17)31463-0
Walter K, Malani PN. What Is Measles? JAMA. 2022;328(23):2370. doi:10.1001/jama.2022.21363
Blutinger E, Schmitz G, Kang C, et al. Measles: Contemporary considerations for the emergency physician. J Am Coll Emerg Physicians Open. 2023;4(5):e13032. Published 2023 Sep 9. doi:10.1002/emp2.13032
Centers for Disease Control and Prevention. Measles cases and outbreaks. Measles (Rubeola). CDC. May 24, 2024. https://www.cdc.gov/measles/data-research/index.html. Accessed May 27, 2024.
Upadhyayula PS, Yang J, Yue JK, Ciacci JD. Subacute Sclerosing Panencephalitis of the Brainstem as a Clinical Entity. Med Sci (Basel). 2017;5(4):26. Published 2017 Nov 7. doi:10.3390/medsci5040026
Centers for Disease Control and Prevention. Nearly 40 million children are dangerously susceptible to growing measles threat. CDC. 2022. https://www.cdc.gov/media/releases/2022/p1123-measles-threat.html. Accessed June 18, 2024.
Centers for Disease Control and Prevention. 04/10/2024: Lab Advisory: CDC Issues Alert for Increase in Global and Domestic Measles Cases and Outbreaks. CDC. 2024. https://www.cdc.gov/locs/2024/04-10- 2024-Lab-Advisory- CDC_Issues_Alert_Increase_Global_Domestic_Measles_Cases_Outbreak s.html#:~:text=On%20March%2018%2C%202024%2C%20the,provid
e%20guidance%20on%20measles%20prevention. Accessed May 29, 2024.
Centers for Disease Control and Prevention. Assessing Measles Outbreak Risk in the United States. CDC National Center for Immunization and Respiratory Diseases. CDC. April 4, 2024. https://www.cdc.gov/ncird/whats-new/measles-outbreak-risk-in- us.html#:~:text=It's%20important%20to%20remember%20that,com munities%20with%20low%20vaccination%20rates. Accessed May 22, 2024.
Centers for Disease Control and Prevention. Questions about measles.
CDC. March 29, 2024. https://www.cdc.gov/measles/about/questions-
about-measles.html . Accessed May 26, 2024.
Davis RL, Marcuse E, Black S, et al. MMR2 immunization at 4 to 5 years and 10 to 12 years of age: a comparison of adverse clinical events after immunization in the Vaccine Safety Datalink project. The Vaccine Safety Datalink Team. Pediatrics. 1997;100(5):767-71. doi: 10.1542/peds.100.5.767
Hambidge SJ, Newcomer SR, Narwaney KJ, et al. Timely versus delayed early childhood vaccination and seizures. Pediatrics. 2014;133(6):e1492-e1499. doi:10.1542/peds.2013-3429
Pawaskar M, Schmidt E, Marshall GS, et al. Use of M-M-R II outside of the routinely recommended age range - a systematic literature review. Hum Vaccin Immunother. 2022;18(1):1-7. doi:10.1080/21645515.2021.1933874
M-M-R II. Prescribing information. Merck and Co., Inc. August 2023. https://www.fda.gov/media/75191/download?attachment#:~:text=2% 20DOSAGE%20AND%20ADMINISTRATION%20For%20Intramuscular%
20or%20Subcutaneous%20administration%20only.&text=A%20single
%20dose%20of%20M%2DM%2DR,to%206%20years%20of%20age. Accessed May 27, 2024.
Erlewyn-Lajeunesse M, Bonhoeffer J, Ruggeberg JU, Heath PT. Anaphylaxis as an adverse event following immunisation. J Clin Pathol. 2007;60(7):737-739. doi:10.1136/jcp.2006.037457
VAERS Vaccine Adverse Event Reporting System. Undated. https://vaers.hhs.gov/. Accessed June 2, 2024.
Frequently asked questions. About the VICP. Health Resource and Services Administration. May 2024. https://www.hrsa.gov/vaccine- compensation/faq. Accessed May 27, 2024.
Masters NB, Beck AS, Mathis AD, et al. Measles virus transmission patterns and public health responses during Operation Allies Welcome: a descriptive epidemiological study. Lancet Public Health. 2023;8(8):e618-e628. doi:10.1016/S2468-2667(23)00130-5
Kraus N, Condon SB. Measles (Rubeola): A Case Of Vaccine Hesitancy And Pregnancy. J Midwifery Womens Health. 2021 May;66(3):391-396. doi: 10.1111/jmwh.13223. Epub 2021 May 22
Porter A, Goldfarb J. Measles: A dangerous vaccine-preventable disease returns. Cleve Clin J Med. 2019 Jun;86(6):393-398. doi: 10.3949/ccjm.86a.19065
Yes, some adults do need to be revaccinated against measles. Healthline. February 9, 2019. https://www.healthline.com/health- news/some-adults-need-to-be-revaccinated-against-measles- 021115#Who-needs-revaccination?. Accessed May 27, 2024.
Murdan S, Ali N, Ashiru-Oredope D. How to address vaccine hesitancy. The Pharmaceutical Journal. April 13, 2021. https://pharmaceutical- journal.com/article/ld/how-to-address-vaccine-hesitancy. Accessed May 27, 2024.
Novilla MLB, Goates MC, Redelfs AH, et al. Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy. Vaccines (Basel). 2023;11(5):926. Published 2023 May 2. doi:10.3390/vaccines11050926
Shen AK, Tan ASL. Trust, influence, and community: Why pharmacists and pharmacies are central for addressing vaccine hesitancy. J Am Pharm Assoc (2003). 2022;62(1):305-308. doi:10.1016/j.japh.2021.10.001
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any
discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.