UNDER PRESSURE: PREVENTION AND MANAGEMENT OF PRESSURE INJURIES
Austin Fredrickson, MD, FACP
Austin Fredrickson is an Associate Professor of Internal Medicine at NEOMED and is a board-certified general internal medicine physician.
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy.
Topic Overview
Pressure injuries (PI) are localized damage to either skin or soft tissue because of pressure or pressure in combination with shear that is either intense, prolonged, or both. Damage to the epithelial or subcutaneous tissues, including muscle and fat, may result in an intact or open wound. They often occur when an internal stiff anatomical structure (like a bone) contacts a stiff external support surface (like a mattress) for long periods. These injuries are a significant global health issue, causing pain, reduced quality of life, and substantial financial burdens. While patients of all ages can be affected, the geriatric population and those residing in long-term care facilities are most likely affected. Effective prevention and treatment of PI requires a coordinated approach involving numerous healthcare team members and an in-depth understanding of PI, risk identification, staging, management, and monitoring strategies. Collaborative care approaches support shared decision-making, enabling team members to combine their expertise in wound care, nutrition, mobility, and patient education to tailor care plans. Interprofessional problem- solving can help ensure timely intervention, enhance patient outcomes, and reduce the economic and personal burdens associated with PI.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-186-H01-P
Pharmacy Technician 0669-0000-24-187-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Course Test and course evaluation
Release Date: December 30, 2024 Expiration Date: December 30, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
Secondary Audiences: Other healthcare professionals, such as nurses, physicians, or others who may be part of a healthcare team, may be interested in this educational topic. Healthcare-team approaches to patient care are discussed in this activity. No state board or professional organization has evaluated this activity to determine whether it meets the continuing education requirements of nurses, physicians, or other professions not listed under the “Target Audience” described above. Always verify with individual employers or supervisors whether they will accept this educational activity upon completion.
How to Earn Credit: From December 30, 2024, through December 30, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Recall risk factors for the development of pressure injuries
Explain staging systems used to classify the severity of pressure injuries
Describe strategies for the prevention and management of pressure injuries
Recall how to monitor patients with pressure injuries
Disclosures
The following individuals were involved in developing this activity: Liz Fredrickson, PharmD, BPCS, Austin Fredrickson, MD, FACP, and Pamela Sardo, PharmD, BS. Pamela Sardo, Liz Fredrickson, and Austin Fredrickson have no conflicts of interest or financial relationships regarding the subject matter discussed. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Under Pressure: Prevention and Management of Pressure Injuries Introduction
Pressure injuries are skin or soft tissue damage requiring prevention and treatment. Prevention and treatment of pressure injuries improve when a coordinated approach involving numerous healthcare team members is used. An in-depth understanding of pressure injuries, their risk, staging, management, and monitoring strategies are also needed. Collaborative care approaches support shared decision-making, enabling team members to combine their expertise in wound care, nutrition, mobility, and patient education to tailor care plans. Interprofessional problem-solving can help ensure timely intervention, enhance patient outcomes, and reduce the economic and personal burdens associated with pressure injuries.
Defining Pressure Injuries
Pressure injuries (PI) are localized skin or soft tissue damage caused by pressure or pressure combined with shear, which is either intense, prolonged, or both.1,2 Damage may occur to the epithelial or subcutaneous tissues, including muscle and fat, resulting in an intact or open wound.1,2 In many cases, they occur when an internal stiff anatomical structure (like a bone) contacts a stiff external support surface (like a mattress) for long periods.1 These injuries are a significant global health issue, causing pain, reduced quality of life, and substantial financial burdens.3 While patients of all ages can be affected, the geriatric population and those residing in long-term care facilities are most likely to be affected.1
Classification of Pressure Injuries
The Prevention and Treatment of Pressure Ulcers/Injuries Clinical Practice Guidelines were last published in 2019 (with updates expected in 2025) and offer clinicians a comprehensive guide to best practices for
preventing and treating PI.3 These guidelines formally define pressure injuries as localized damage to the skin and/or underlying tissue due to pressure or pressure in combination with shear.3 Within the medical community, the term PI is preferred. However, they also may be referred to as “ulcers,” “decubitus ulcers,” “pressure sores,” or “bed sores”.5 Given this ambiguity, it is essential for healthcare providers to understand both the definitions of PI as well as how to classify these injuries.1
Staging pressure injuries assists healthcare providers in determining the amount of tissue damage that has occurred.6 The National Pressure Injury Advisory Panel (NAIAP) revised this staging system (Table 1) after receiving inquiries from healthcare providers attempting to stage and diagnose PI.6,7 Figure 1 illustrates the tissues involved in PI.
Table 1
National Pressure Injury Advisory Panel Staging System7
| Stage | Description |
| Stage 1 Pressure Injury | Non-blanchable erythema of intact skin. Intact skin with a localized area of non-blanchable erythema, which may appear differently in darkly pigmented skin. The presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visual changes. Color changes do not include purple or maroon discoloration; these may indicate deep tissue pressure injury. |
| Stage 2 Pressure Injury | Partial-thickness skin loss with exposed dermis. Partial- thickness loss of skin with exposed dermis. The wound bed is viable, pink or red, moist, and may also present as an intact or ruptured serum-filled blister. Adipose (fat) is not visible, and deeper tissues are not visible. Granulation tissue, slough, and eschar are not present. Commonly, Stage 2 PI results from adverse microclimate and shear in the skin over the pelvis and shear in the heel. It should not describe moisture- associated skin damage (MASD) such as incontinence- associated dermatitis (IAD), intertriginous dermatitis (ITD), medical adhesive-related skin injury (MARSI), or traumatic wounds. |
| Stage 3 Pressure Injury | Full-thickness skin loss. Full-thickness loss of skin, in which adipose (fat) is visible in the ulcer and granulation tissue and epibole (rolled wound edges) are often present. Slough and/or eschar may be visible. Depth of tissue damage varies by location; areas of significant adiposity can develop deep wounds. Undermining and tunneling may occur. Fascia, muscle, tendon, ligament, cartilage, and/or bone are not exposed. If slough or eschar obscures the extent of tissue loss, this is an Unstageable Pressure Injury. |
| Stage 4 Pressure Injury | Full-thickness skin and tissue loss. Full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage, or bone in the ulcer. Slough and/or eschar may be visible. Epibole (rolled edges), undermining, and/or tunneling often occur. Depth varies by anatomical location. If slough or eschar obscures the extent of tissue loss, this is an Unstageable Pressure Injury. |
| Unstageable Pressure Injury | Obscured full-thickness skin and tissue loss. Full- thickness skin and tissue loss, in which the extent of tissue damage within the ulcer cannot be confirmed because it is obscured by slough or eschar. If slough or eschar is removed, a Stage 3 or Stage 4 pressure injury will be revealed. Stable eschar (dry, adherent, intact without erythema or fluctuation) on the heel or ischemic limb should not be softened or removed. |
| Deep Tissue Pressure Injury | Persistent non-blanchable deep red, maroon, or purple discoloration. Intact or non-intact skin with a localized area of persistent, non-blanchable deep red, maroon, or purple discoloration or epidermal separation revealing a dark wound bed or blood-filled blister. Pain and temperature changes often precede skin color changes. Results from intense and/or prolonged pressure and shear forces at the bone-muscle interface. It may evolve rapidly to reveal the extent of tissue injury or resolve without tissue loss. Do not use deep tissue pressure injuries (DTPI)* to describe vascular, traumatic, neuropathic, or dermatologic conditions. |
*Defined as purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear

Figure 1 Pressure Injury Staging
Etiology and Epidemiology
Epidemiology
While there has been a decrease in pressure injuries over the last twenty years, they remain a significant global health issue, causing pain, reduced quality of life, and substantial financial burdens for many individuals and their families.2,3 Their prevalence in healthcare settings ranges widely, with acute hospitals reporting a global point prevalence of 14.8% and an incidence of 6.3%.3 The estimated prevalence varies within healthcare settings around the globe and has been estimated to be as high as 72.5% in some settings.3 In the United States (US), an estimated 3 million PI are evaluated and treated annually.2 Vulnerable populations, such as those in critical or palliative care, neonates, and individuals with spinal cord injuries, face higher risks.3 While efforts have led to a gradual decline in prevalence within general acute care, pressure injuries still contribute to increased morbidity, mortality, extended hospital stays, and readmissions.3 It has been estimated that the US healthcare system spends nearly 27 billion dollars annually on hospital- associated PI.3 Costs per case vary greatly and are influenced by location.3
Risk Factors for the Development of Pressure Injuries
Pressure injuries result from a complex interplay of risk factors, including modifiable and non-modifiable factors.3 The risk factors that lead to PI can be broadly categorized into two groups: exposure to damaging mechanical boundary conditions (the type, magnitude, time, and duration of the mechanical load) and the susceptibility and tolerance of the patient.3 Key contributors include immobility, advanced age, and chronic conditions such as diabetes mellitus, vascular diseases, and neurological disorders, which impair tissue perfusion and wound healing.3 Populations at increased risk include those with spinal cord injuries, individuals undergoing prolonged surgical procedures, and patients in critical care or palliative settings.3 Poor nutritional status, obesity, and conditions that cause localized pressure, such as medical devices, also increase susceptibility to these injuries.3 Table 2 presents common risk factors for pressure injuries.
Table 2
Common Risk Factors for Pressure Injuries3
| Activity and mobility limitations |
| Skin status |
| Perfusion, circulation, and oxygenation factors |
| Nutrition indicators |
| Moisture |
| Body temperature |
| Older age |
| Sensory perception limitations |
| Blood markers |
| General and mental health status |
| Individuals in the operating room |
| Critically ill individuals |
| Neonates and children |
Pathophysiology
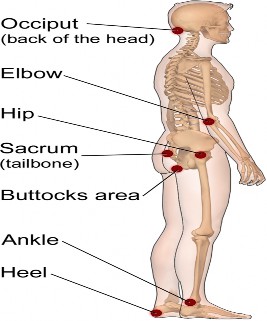
Four main factors contribute to the development of PI: pressure, friction, shearing forces, and moisture, and they may be caused by one or a combination of any of these factors.3,8 Pressure is defined as normal force per unit surface area of the skin or underlying tissue.3 When pressures on soft tissues exceed normal capillary pressure (12 to 32 mm Hg), oxygenation decreases, compromising microcirculation and leading to tissue damage.8 If unrelieved, pressure injuries can develop within 3 to 4 hours, commonly over areas like the sacrum, ischial tuberosities, trochanters, malleoli, and heels.8 Common sites are illustrated in Figure 2. The presence of moisture (like from perspiration) can result in both tissue breakdown and maceration, while friction (defined as phenomena that relate to interface properties and sliding surfaces with respect to each other) may lead to ulceration and erosion of the skin.3,8 Shearing forces are forces that are parallel to the skin and occur when a patient is placed on an inclined surface.3,8 While these forces are not directly responsible for PI, they can exacerbate these injuries by causing more damage to supporting tissues.8
Figure 2
Common Pressure Injury Sites9
The mechanism of injury varies depending on the tissues, and tissue tolerance varies based on type, microclimate, perfusion, health status, and comorbidities.3 While often affecting the skin, PI can also occur within mucous membranes, commonly due to medical devices exerting prolonged pressure.3 Injury mechanisms involve cell deformation, inflammation, and ischemia- reperfusion injury, leading to cascading damage at the cellular and tissue levels.3
Clinical Presentation and Assessment Risk Assessment for Pressure Injuries
A thorough assessment is essential for identifying individuals at high risk of pressure injuries and implementing targeted preventive measures. Through a collaborative care approach, the healthcare team should evaluate factors contributing to the duration, type, and magnitude of pressure, as well as patient-specific elements affecting susceptibility, such as mobility, activity levels, skin integrity, perfusion, and comorbidities.2,3 By leveraging diverse expertise, clinicians can stratify risk based on clinical significance, paying close attention to conditions like acute illness, prolonged immobility, or existing PIs, which predispose patients to further tissue breakdown.2,3
The use of validated risk assessment tools provides a structured, evidence-based framework for evaluating factors like friction, shear, and moisture.2,3 However, interprofessional clinical judgment remains crucial for interpreting these findings and addressing unique patient needs. For example, in patients with spinal cord injuries, the team can collaboratively design advanced interventions, such as employing pressure redistribution surfaces and implementing frequent repositioning schedules tailored to their specific limitations.2,3 Evidence-based guidelines should be integrated with individualized assessments to develop prevention plans that prioritize modifiable risks, enhance tissue tolerance, and reduce the incidence of PIs.
In addition to considering risk factors, clinicians should also conduct a thorough skin assessment.2,3 This should involve checking any bony prominences that may be in contact with medical devices (like a splint) and assessing the skin for integrity, erythema, firmness, moisture, pain, and discomfort.2,3 It is recommended to document pictures of identified PI to track and monitor patient progress.2 Together, these factors assist clinicians in staging pressure injuries.2,3 Conducting these assessments guides the clinical staging of PIs and promotes a shared decision-making process involving patients and caregivers when appropriate.
Several scales, such as the Norton Scale and the Braden Scale, have been developed to predict the risk of pressure injury development. The Norton Scale (Table 5) evaluates five criteria—physical condition, mental condition, activity, mobility, and incontinence—while the Braden Scale assesses six categories: sensory perception, moisture, activity, mobility, nutrition, and friction/shear.3,8 Although these scales are considered standard care, studies have not demonstrated a reduction in pressure injuries compared to skilled clinical assessment alone.8 However, combining a risk assessment scale with skilled clinical evaluation is recommended for comprehensive patient care.8
| Criterion | Score 4 | Score 3 | Score 2 | Score 1 |
| Physical condition | Good | Fair | Poor | Very bad |
| Mental condition | Alert | Apathetic | Confused | Stupor |
| Activity | Ambulant | Walk with help | Chair bound | Bed bound |
| Mobility | Full | Slightly impaired | Very limited | Immobile |
| Incontinent | Not | Occasionally | Usually/Urine | Doubly |
Table 5 Norton Scale8
Note: Calculated as the sum of the scores in all five areas. A score < 14 indicates a high risk of pressure ulcer
Prevention and Treatment Strategies
Prevention strategies involve skin care regimens, nutritional regimens, and repositioning and mobilization plans.2,3 These strategies are most effective through an interprofessional, collaborative care approach for wound care, nutrition, mobility, and patient education.4
By leveraging the unique expertise of each team member, including dietitians, nurses, physical therapists, pharmacists, and physicians, prevention plans can be tailored to meet the patient's comprehensive needs. Teams can develop and execute prevention strategies that address the complex interplay of risk factors by fostering open communication, shared decision-making, and mutual respect. These strategies, which illustrate the value of collaborative care in reducing pressure injury incidence and improving patient outcomes, will be described in detail below.
Prevention Strategies: Skin Care
Maintaining skin integrity is foundational in preventing pressure injuries.3 Proper nutrition and hydration both play a vital role in skin health.3 Managing skin conditions such as eczema and incontinence-associated dermatitis is critical to maintaining the skin's protective function and overall integrity.3 Implementing a tailored skin care regimen is essential for patients, and this should include keeping the skin clean and appropriately hydrated, cleansing promptly after incontinence, avoiding alkaline soaps (pH of 9.5- 10.5) and cleansers, and using barrier products to protect the skin from excessive moisture.2,3 Patients should also be counseled to avoid vigorous rubbing or massaging of the skin during cleansing, drying, or applying barrier products, as this can damage the skin and increase the risk of pressure injuries.2,3
Fatty acid creams have shown potential in reducing the incidence of PI and are among the topical agents used to support prevention strategies.8 These products are believed to work by decreasing frictional forces and promoting healthy skin maintenance.8 Evidence from two randomized studies
suggests that fatty acid creams can effectively lower the risk of PI development.8 In contrast, other topical agents containing ingredients like silicone, dimethyl sulfoxide, and zinc have been explored with limited success.8 Some of these products have shown little benefit or, in certain cases, even detrimental effects.8
Prevention Strategies: Pressure Redistribution
Pressure redistribution includes frequent repositioning, maintaining a low bed incline, and optimal patient positioning, and is critical in minimizing the risk of PI.3,10 Healthcare providers should consider factors such as a patient’s body weight, body habitus, and functional status when considering pressure redistribution and the use of beds and chairs.3 Traditionally, it has been recommended to reposition a patient every 2 hours; however, recent National Pressure Injury Advisory Panel guidelines have removed this specific interval due to insufficient evidence.3,10 A randomized study comparing 2-hour versus 3-hour repositioning on a standard hospital mattress revealed a non- significant 7% reduction in pressure injury incidence in the 2-hour group.10 Further analysis indicated that stage 2 to 4 pressure injuries developed in 14% of the 2-hour group versus 24% of the 3-hour group.10 Additionally, cost- effectiveness analyses suggest that alternating 2- and 4-hour repositioning is only marginally more effective than continuous 4-hour repositioning and may not justify the increased resource use.10
Consideration of the support surface itself is also important, and these can be classified as either static or dynamic.3 Static surfaces, like standard foam mattresses, offer limited protection against pressure injuries, while high- specification foam and medical-grade sheepskin provide better support.3 Dynamic surfaces, such as alternating pressure mattresses, can off-load high- pressure areas without requiring caregiver involvement.3 The angle of bed elevation significantly influences pressure injury risk.3,10 A lower head-of-bed elevation is recommended to reduce shear and frictional forces.10 The 30° lateral tilt position—where pillows support the patient laterally, avoiding direct pressure on bony prominences—has shown advantages over supine or 90° lateral positions.10
Prevention Strategies: Nutrition
Nutrition is critical in preventing and treating pressure injuries, as all organ systems rely on adequate macronutrients and micronutrients for growth, repair, and tissue maintenance.3 Malnutrition, which includes deficiencies, excesses, or imbalances in energy, protein, and other nutrients, adversely affects tissue structure, body function, and clinical outcomes.3 Clinicians may identify malnutrition by uncovering unintended weight loss, muscle mass depletion, and decreased functional status.3 Both undernourished and well-nourished individuals can develop pressure injuries under certain conditions, with older adults facing heightened risk due to factors like anorexia of aging, which leads to reduced appetite, weight loss, and altered metabolic states.3 Notably, even individuals with obesity may suffer from poor nutritional status.3 Research has demonstrated that individuals with inadequate nutritional intake or unintended weight loss face higher risks of pressure injury severity and delayed healing.3 To mitigate these risks, nutritional screening is essential for individuals at risk of pressure injuries, focusing on accurate assessments and targeted interventions, such as tailored diets and specific supplements, to improve prevention and healing outcomes.3
Treatment Strategies
Effective management of pressure injuries requires a comprehensive, interprofessional approach to assessment and treatment. This collaborative care process should involve integrating the expertise of various healthcare team members to develop strategies that promote healing, prevent complications, and address the patient's physical and psychosocial needs. The healthcare team should perform regular evaluations of healing progression, dressing condition, and pain levels, and clinicians can use tools such as the Pressure Ulcer Scale for Healing (PUSH) and the Bates-Jensen Wound Assessment Tool to monitor and document progress.2,3,8 These assessments benefit from the combined input of nurses, physicians, and wound care specialists to ensure a holistic approach tailored to each patient.2,3,8
Psychosocial support for patients and caregivers is essential to enhance adherence to treatment plans and address the emotional impact of pressure injuries. Social workers, mental health counselors, and patient navigators can collaborate to provide resources, counseling, and education to mitigate stress and improve coping strategies. By fostering team-based care, shared decision-making, and ongoing communication, interprofessional teams can ensure that treatment strategies are patient-centered, comprehensive, and adaptable to the dynamic needs of individuals with pressure injuries.
Wound site management focuses on cleansing to remove debris and support healing without damaging healthy tissue.2,3,8 Protecting surrounding skin with dressings or barriers helps prevent irritation and infection, and surgical debridement may be needed.2,3,8 Nutritional optimization, including adequate protein and calorie intake, is also vital for tissue repair and healing.2,3,8 While supplements such as zinc and vitamin C may aid recovery, currently available evidence remains mixed, particularly in individuals with existing deficiencies.2,3,8 Microbial mitigation involves managing bacterial growth, with systemic antibiotics reserved for confirmed infections like cellulitis or osteomyelitis.2,3,8 Table 6 details standard wound dressings.2
Table 6 Wound Dressings2
| Dressing | Injury type | Guidance for use |
| Hydrogels | Noninfected Stage 2 injuries with minimal drainage | Preferred for dry wound beds that would benefit from autolytic debridement Barrier protection may be added around the wound to reduce the risk of maceration |
| Moist gauze | Alternative dressing for any injury type | Use when other wound dressing types are not an option Associated with slower wound healing Costly in professional time, as frequent visits for dressing changes are needed |
| Films | Secondary dressing for any injury type | Avoid the use over enzymatic debriding agents |
| Calcium alginate | Stage 3 and 4 injuries with moderate exudate | Avoid use in dry wound beds; can maintain a physiologic environment |
| Foams | Stage 2 and greater pressure injuries with moderate or heavy exudate | Use in deep injuries, with additional use of filler dressings to occupy empty space Requires secondary dressing to extend the duration of use |
| Hydrocolloids | Noninfected Stage 2 injuries | Must be removed carefully from fragile skin because removal can cause trauma; does not require frequent dressing changes |
| Calcium alginate gels | Injuries with or at risk of biofilms | Prevents and destroys biofilms |
| Honey | Injuries with or at risk of biofilms | Prevents biofilm growth and extension of colonization |
| Iodine | Injuries with or at risk of biofilms | Prevents biofilm growth and destroys active biofilms Avoid in patients with iodine allergies or kidney and thyroid dysfunction Contraindicated for extensive burns |
Wound dressings impregnated with silver salts or metals | Injuries with or at risk of biofilms | Breaks down active biofilm; avoid in patients with silver sensitivity Must be changed more often if there is heavy exudate |
Effective pain management and wound bed preparation are also essential components of comprehensive PI.2,3 Collaborative efforts among healthcare professionals ensure that pain assessments and interventions are patient-centered and address the multifaceted needs of individuals. Comprehensive pain assessments should be tailored to each patient and use tools that consider factors such as character, intensity, duration, and changes in pain over time.2,3 These evaluations should incorporate input from multiple team members, including nurses, physicians, and physical therapists, to
holistically address physical, neurological, and psychosocial factors. Non- verbal cues are especially critical for individuals unable to communicate their pain verbally, and team members must work together to interpret these signals accurately.2,3
Interprofessional collaboration is key in implementing pain management strategies and should include professional education on pain-relief techniques and care coordination to optimize analgesia administration.2,3 Pharmacists and pain specialists can guide the appropriate use of medications, while nurses and occupational therapists can integrate these strategies into daily care routines. For wound care procedures, topical opioids or analgesics may be applied to minimize procedural pain and enhance patient comfort, with the care team ensuring proper administration and monitoring for effectiveness.2,3 A team-based approach can help ensure that pain management and wound bed preparation are practical and aligned with the patient's preferences and overall treatment goals. By leveraging the strengths of an interprofessional team, healthcare providers can enhance comfort, promote healing, and improve the quality of life for individuals with pressure injuries.
Management of chronic wounds requires vigilance to address systemic and spreading infections.2,3 Clinicians should assess for signs like erythema, wound breakdown, induration, and systemic symptoms such as lethargy or confusion.2,3 Evidence-based strategies, such as antimicrobial treatments and moisture-retentive dressings, play a pivotal role in addressing these challenges.2,3 Advanced therapies, including biofilm management and infection control, complement comprehensive wound care practices to enhance healing outcomes.2,3
Emerging therapies offer additional options for managing severe pressure injuries.2 Electrical stimulation, low-frequency ultrasound, and vacuum-assisted closure can support healing in higher-stage wounds.2 Biological dressings, including collagen matrix products, show promise in improving healing and reducing inflammation, though cost and availability may limit their use.2 Continued research is needed to validate the efficacy of these treatments and integrate them into standard care practices.2
Patient Education
Evidence indicates that patient education and lifestyle programs can play a role in pressure injury prevention and management, though results are mixed.3 Some studies have shown reduced pressure injury recurrence rates and improved self-care skills following multifaceted education programs, with benefits lasting up to 24 months.3 However, other studies found no significant reduction in pressure injuries or improved quality of life compared to standard care.3 Education programs have demonstrated short-term improvements in patient knowledge and preventive behaviors, but translating these gains into sustained behavioral changes and reduced injury rates remains inconsistent.3 Variability in outcomes may stem from differences in program delivery, content, intensity, participant characteristics, and follow-up duration.3
Healthcare providers should integrate patient education into routine care, tailoring approaches to individual needs.3 This includes considering cognitive and psychological status, education level, literacy, and physical abilities.3 Multiple delivery methods, such as verbal instructions, written materials, internet resources, and telephone support, enhance engagement and retention.3 Engaging caregivers in education and skills training is crucial, especially for populations at high risk, like individuals with spinal cord injuries.3 Programs should emphasize self-management, reinforce skills periodically, and use evidence-based resources to promote long-term adherence.3 Additionally, addressing psychological barriers, such as depression or low motivation, is essential to maximize the impact of education and lifestyle interventions.3
Resources
International Guideline for the Prevention and Treatment of Pressure Ulcers/Injuries
Academy of American Family Physicians
Summary
Pressure-induced skin injuries, commonly known as pressure injuries or bed sores, are local skin or soft tissue damage caused by pressure or pressure combined with shear. They are a significant concern in acute and long-term care settings and can lead to severe complications if not managed properly.
Course Test
Which of the following is considered a risk factor for developing pressure injuries?
Hypermobility
Younger age
Regular exercise
Poor nutritional status
Which description best matches a Stage 2 pressure injury?
Non-blanchable erythema of intact skin
Partial-thickness skin loss with exposed dermis*
Full-thickness skin and tissue loss with exposed muscle or bone
Full-thickness skin loss with slough or eschar obscuring tissue damage
What is a key principle of managing pressure injuries?
Vigorous massage of affected skin to promote circulation
Regular debridement of necrotic tissue and controlling microbial burden
Restricting fluid intake to prevent edema
Avoiding all skin care products to minimize irritation
Which tool is commonly used to monitor healing progression in patients with pressure injuries?
Bates-Jensen
Pressure Ulcer Scale for Healing (PUSH)
Norton Scale
Glasgow Coma Scale
Which of the following is a modifiable risk factor for developing pressure injuries?
Advanced age
Immobility
Spinal cord injury
Sensory perception limitations
What role does moisture play in the development of pressure injuries?
It prevents skin maceration
It reduces the risk of pressure injuries by hydrating the skin
It can cause tissue breakdown and increase susceptibility to pressure injuries
It does not affect the development of pressure injuries
Which stage of pressure injury is characterized by non-blanchable erythema of intact skin?
Stage 1
Stage 2
Stage 3
Deep tissue pressure injury
Which of the following is a recommended practice to prevent skin damage during wound care?
Vigorous scrubbing of the wound
Use of alkaline soaps for cleansing
Use of barrier products to protect skin from moisture
Skipping dressing changes to minimize disruption
What should healthcare providers monitor regularly to assess the progression of a pressure injury?
Patient weight only
Dressing condition, healing progression, and pain levels
Skin temperature
Blood pressure
Interprofessional collaboration is key in implementing pain management strategies for pressure pain that
should include professional education on pain-relief techniques and care coordination to optimize analgesia administration
provides team-based treatment goals that do not consider the patient's preferences.
directs and orders the patient to make lifestyle changes.
excludes dietitians because pressure pain is an environmental condition that is not impacted by diet.
References
Kottner J, Cuddigan J, Carville K, et al. Pressure ulcer/injury classification today: An international perspective. J Tissue Viability. 2020;29(3):197-203. doi:10.1016/j.jtv.2020.04.003
Visconti AJ, Sola OI, Raghavan PV. Pressure Injuries: Prevention, Evaluation, and Management. Am Fam Physician. 2023;108(2):166- 174.
Kottner et al. Prevention and treatment of pressure ulcers/injuries: International Clinical Practice Guideline 2019. https://static1.squarespace.com/static/6479484083027f25a6246fcb/t/6 553d3440e18d57a550c4e7e/1699992399539/CPG2019edition-digital- Nov2023version.pdf. Accessed December 5, 2024.
Interprofessional education Collaborative. IPEC Core Competencies. Accessed December 5, 2024.
Pressure Injury Prevention and Wound Management. Fragility Fracture Nursing: Holistic Care and Management of the Orthogeriatric Patient [Internet]. Hertz K, Santy-Tomlinson J, editors. Cham (CH): Springer; 2018.
Pressure ulcers get new terminology and staging definitions. Nursing. 2017;47(3):68-69. doi:10.1097/01.NURSE.0000512498.50808.2b
National Pressure Injury Advisory Panel Staging System. Available at: https://cdn.ymaws.com/npuap.site- ym.com/resource/resmgr/npuap_pressure_injury_stages.pdf. Accessed December 5, 2024.
Mervis J. MERCK Manual. Pressure Injuries. (Bedsores; Pressure Ulcers; Decubitus Ulcers; Decubiti; Pressure Sores). Available at: https://www.merckmanuals.com/professional/dermatologic- disorders/pressure-injury/pressure-injuries. Accessed December 5, 2024.
BruceBlaus. Pressure Ulcer Sites.png. Wikimedia Commons. Published July 18, 2017.
https://commons.wikimedia.org/wiki/File:Pressure_Ulcer_Sites.png. Accessed December 5, 2024.
Mervis JS, Phillips TJ. Pressure ulcers: Prevention and management. J Am Acad Dermatol. 2019;81(4):893-902. doi:10.1016/j.jaad.2018.12.068
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary
from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.