PHARMACY TEAM GUIDE TO GERD
L. Austin Fredrickson, MD, FACP
Dr. Fredrickson is an associate professor of internal medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board- certified in general internal medicine and practices rural primary care.
Topic Overview
Gastroesophageal reflux disease, or GERD, remains a pervasive problem, affecting up to 30% of the population. Pharmacists are readily accessible health providers able to assist patients in selecting optimal short-term GERD treatments and thus should have a thorough understanding of available over- the-counter treatment options and be able to select appropriate agents specific to each patient. Pharmacists should also be able to recognize GERD alarm symptoms and refer patients to their healthcare provider when appropriate. This continuing education course will provide a thorough review of the diagnosis and treatment of GERD, with a focus on nonpharmacologic and pharmacologic treatment strategies. Patient counseling points and tips for pharmacy technicians will also be discussed.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-043-H01-P
Pharmacy Technician 0669-0000-24-044-H01-T
Credits: 1.5 contact hour(s) (0.15 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $5.99
Estimated time to complete activity: 1.5 contact hour(s) (0.15 CEU(s)), including Course Test and course evaluation
Release Date: March 29, 2024 Expiration Date: March 29, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
How to Earn Credit: From March 29, 2024, through March 29, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Describe the pathophysiology of gastrointestinal reflux disease (GERD)
Recognize alarm symptoms of GERD
Identify nonpharmacologic strategies for the management of GERD
Describe possible drug interactions in individuals with GERD
The following individuals were involved in developing this activity: L. Austin Fredrickson, MD, and Pamela Sardo, PharmD, BS. Pamela Sardo and L. Austin Fredrickson have no conflicts of interest or financial relationships regarding the subject matter discussed. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Pharmacy Team Guide to GERD Introduction
Gastroesophageal reflux disease is a common gastrointestinal disease encountered by healthcare providers. Pharmacists are readily accessible health providers able to assist patients in selecting optimal short-term GERD treatments. This requires a thorough understanding of available over-the- counter treatment options and assisting in selecting appropriate agents for each patient. Pharmacists should also be able to recognize GERD alarm symptoms and refer patients to their healthcare provider when appropriate. This continuing education course will review the diagnosis and treatment of GERD, focusing on nonpharmacologic and pharmacologic treatment strategies. Patient counseling points and tips for pharmacy technicians will also be discussed.
Etiology and Epidemiology
Gastroesophageal reflux disease, or GERD, is a chronic gastrointestinal disorder that results in regurgitation of gastric contents into the esophagus.1 GERD has long been one of the most common gastrointestinal diseases encountered by healthcare providers. Clinicians' knowledge regarding the differing presentations of GERD, new diagnostic modalities, and approaches to patient management has evolved and changed in recent years.2 A patient- centered approach that considers lifestyle changes, pharmacologic modalities, and surgical and endoscopic options is key to optimizing outcomes. Changes to management approaches are summarized in the 2021 American College of Gastroenterology (ACG) Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease.2
GERD is highly prevalent in the United States (US), and the most recent data finds approximately 20% of adults have GERD.3 Given that many patients either do not seek treatment or attempt to self-treat using nonprescription
medications, these rates likely underestimate the true prevalence of this condition. It has been reported that up to 50% of all adults will report symptoms of reflux at some point.4 One meta-analysis found women have slightly higher rates of GERD symptoms compared to men.5 Pregnancy and NERD (nonerosive reflux disease) contribute to this higher prevalence.6
The development of GERD is associated with numerous risk factors. These include older age (over age 50), excessive body weight (high body mass index), smoking, anxiety, depression, and low physical activity.7,8 Patients who are obese have a 2.5 times increased risk of developing GERD.9 Additional risk factors include consumption of alcohol, certain foods, such as spicy foods, coffee, and peppermint, certain medications, and respiratory disease.10 Table 1 lists drugs that may have adverse effects on the esophagus.10 Pharmacists should review medication lists to determine if patients are taking prescription, over-the-counter (OTC), or herbal products that may cause or worsen GERD.
Table 1
Medications that Promote or Worsen GERD10,11
| Decreased Lower Esophageal Sphincter Pressure | Direct Irritant to the Esophageal Mucosa |
| Nitrates | Aspirin |
| Anticholinergic agents | Bisphosphonates |
| Dihydropyridine calcium channel blockers | NSAIDs |
| Aminophylline | Iron |
| Barbiturates | Quinidine |
| Caffeine | Potassium chloride |
| Dopamine | |
| Estrogen | |
| Nicotine | |
| Tetracycline |
Pathogenesis
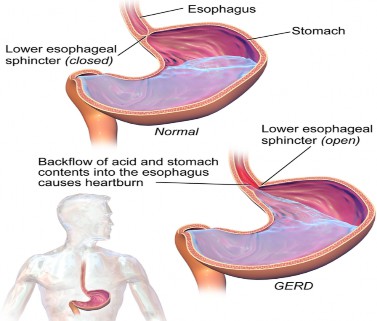
GERD is a disorder of the lower esophageal sphincter (LES) (Figure 1).8 Key to the development of GERD is when gastric contents are abnormally
refluxed into the esophagus, oral cavity, and/or the lungs.2 A host of factors can contribute to the development of GERD that may be physiologic or pathologic in nature.2,8 Transient lower esophageal sphincter relaxation (TLESR) is the most common cause.2,8 These are short moments of lower esophageal sphincter inhibition that occur independent of swallowing and tend to occur more frequently after eating.2,8 Esophageal distention, vomiting, belching, and retching can also relax the LES.10 Other contributing factors include reduced LES pressure, hiatal hernias, impaired esophageal clearance, decreased salivary production, and delayed gastric emptying.2,10 Because of this complex and multifaceted pathophysiology, the ACG guidelines suggest GERD is approached not as a single disease but one with multiple presentations and diagnostic considerations.2
Figure 1
Lower Esophageal Sphincter12
Certain substances, including gastric acid, pepsin, bile acid, and pancreatic enzymes, can cause damage to the esophagus when reflux occurs.10 Thus, factors such as the volume and composition of refluxate and how long the esophagus is exposed to the refluxate can determine the severity
of GERD.10 While routine screening for Helicobacter pylori is not recommended as part of diagnosing and managing GERD, the role of this bacteria is not entirely clear. More research is needed to elucidate this.10
Clinical Presentation and Diagnosis Clinical Presentation
Many patients with GERD present with the hallmark symptom of “heartburn,” or substernal burning discomfort.2 This pain typically rises up toward the neck.2 Symptoms of regurgitation are also present, which may occur with or without an accompanying bitter taste.2 Heartburn and regurgitation are the most specific and sensitive symptoms.2 While heartburn is the most common symptom, patients may also present with “atypical” symptoms as well.2 These are often referred to as extraesophageal (EE) symptoms and include noncardiac chest pain, chronic cough, asthma, laryngitis, tonsilitis, sore throat, excessive phlegm and throat clearing, hoarse voice, odynophagia, and dental erosion.2 The latter may occur as the result of the flow of gastric contents into the larynx and hypopharynx.13 Extraesophageal symptoms can be challenging for clinicians because they can result from multiple other causes.2
Pharmacists should be aware of alarm symptoms associated with GERD. Alarm symptoms can suggest a more serious, underlying issue such as malignancy.2 These symptoms include dysphagia (difficulty swallowing), odynophagia (painful swallowing), anemia, bleeding, and unintended weight loss.2 If a patient presents to a pharmacy for OTC treatment of GERD and one or more of these symptoms is present, they should be referred to their PCP for evaluation.2
Diagnosis
There is no gold standard for diagnosing GERD.2 Clinicians should consider the patient’s presenting symptoms, endoscopic findings, and response to therapeutic management when confirming the diagnosis.2 Patients
who present with symptoms of heartburn, especially when related to the timing of meals, are likely to have GERD.8 In fact, a clinical history is considered the best diagnostic tool, and clinicians should take care to ascertain both a patient’s symptoms and risk factors for GERD.10
The diagnosis of GERD can be made when a patient presents with classic symptoms and then responds to acid suppression therapy.8 Response to proton pump inhibitor (PPI) as a diagnostic tool has a sensitivity of 97% and a specificity of 54%.2,14,15 Clinicians may also consider evaluating the patient for GERD complications.8 An esophagogastroduodenoscopy (EGD) is the most common diagnostic test used to evaluate a patient for GERD complications and assess for mucosal injury.8 An EGD provides clinicians with a direct visualization of the esophageal mucosa (Figure 2).8 Patients with typical GERD symptoms tend to have normal EGD findings; however, underlying erosive esophagitis could be missed for those taking PPIs.2 EGDs are useful in determining if esophagitis, strictures, or Barrett’s esophagus is present.8
Figure 2. EGD16

Ambulatory pH monitoring can also be conducted and is considered the gold standard for diagnosing acid reflux.8 With ambulatory pH monitoring, acid reflux events are tracked and correlated with a patient’s symptoms.8 This test has a sensitivity of 96% and a specificity of 96%.8 Conversely, barium esophagrams are considered poor screening tests for GERD, with a sensitivity of 26% and specificity of 50%.8 This is because barium reflux does not
correlate well with acid reflux in symptomatic patients.8 Indications for endoscopy are listed in Table 2.8
Persistent or progressive GERD symptoms despite appropriate therapy |
| Presence of dysphagia or odynophagia |
| Unexplained weight loss of more than 5% |
| Presence of GI bleeding and strictures |
| Screening for Barrett’s esophagus in high-risk patients |
| Placement of wireless pH monitoring |
Prior to endoscopic or surgical antireflux procedures or after procedures in those with recurrent symptoms |
Table 2 Indications for Endoscopy10
Finally, there has been a newly approved device used to evaluate GERD.2 This involves the use of a catheter-based balloon that is lined by sensors used to measure mucosal impedance during endoscopy.2 This method may have utility as an adjunct to endoscopy for GERD diagnosis.2
Management Strategies for GERD
The goals of treating GERD are to 1) reduce the patient’s symptoms while improving overall quality of life, 2) decrease the frequency and recurrence of reflux, 3) heal the injured mucosa, and 4) prevent complications.10 With these goals in mind, treatments should be aimed at
1) decreasing the acidity of refluxate, 2) decreasing gastric volume available to be refluxed, 3) improving gastric emptying, 4) increasing LES pressure,
5) enhancing esophageal acid clearance, and 6) protecting the esophageal mucosa. The initial treatment strategy is dependent on the patient’s presenting symptoms, including symptom frequency and the presence of any complications.2 Treatment should be done in a shared decision-making model with the patient.2
Nonpharmacologic (Lifestyle Changes)
Lifestyle modifications are often recommended as part of the initial treatment strategy for patients with GERD. Recommendations include weight loss for patients who are overweight, avoiding tobacco and alcohol, avoiding late-night meals and snacking, staying upright after meals, and avoiding foods that worsen or trigger reflux symptoms.2 There is limited data to fully support many of these recommendations due to study size and a lack of data that focuses on only nonpharmacologic interventions.2 Literature does support elevating the head of the bed or sleeping on a wedge to improve nocturnal GERD symptoms.17,18 Additionally, a large cohort study found cessation of smoking also improved GERD symptoms.19
Data regarding diet is mixed. In some laboratory studies, coffee, caffeine, citrus, and spicy food were not found to affect LES pressure.20,21 However, a more recent article found six servings of tea, coffee, or soda were associated with increased symptoms compared to zero servings per day.22 The timing of food intake can also play a role. Going to bed or lying down less than three hours after eating has been associated with an increase in GERD symptoms.23 The ACG lifestyle recommendations are summarized in Table 3.2
Table 3
Summary of Lifestyle Recommendations2
| Lifestyle modification | Strength of evidence | Recommendable? |
| Avoid fatty meals | Equivocal | Yes |
| Avoid carbonated beverages | Moderate | Yes |
| Select decaffeinated beverages | Equivocal | Not generally |
| Avoid citrus | Weak | Yes, if citrus triggers symptoms |
| Eat smaller meals | Weak | Yes |
| Lose weight | Equivocal | Yes |
| Avoid alcoholic beverages | Weak | Not generally |
| Stop smoking | Weak | Yes |
| Avoid excessive exercise | Weak | Yes |
| Sleep with head elevated | Equivocal | Yes |
| Sleep on the left side | Unequivocal | Yes |
Pharmacologic Strategies
Medications are the cornerstone of treatment for GERD. Broadly, pharmacologic treatments are used to either neutralize or reduce gastric acid.10 Pharmacologic therapy includes patient-directed therapy, with the use of nonprescription antacids, histamine-2 receptor antagonists (H2RAs) or PPIs, prescription-strength acid suppression therapy, or treatment with promotility medications.10
Patient-Directed Therapy
Patients who present with mild, intermittent symptoms are candidates for patient-directed therapy.10 If symptoms last beyond a two-week span, the patient should then seek further medical attention.10 Pharmacists should be able to triage patients presenting to pharmacies seeking self-care for GERD symptoms. If any of the following are present, patients should be referred to their primary care provider: severe or nocturnal heartburn for more than three months; symptoms of GERD despite taking prescription-strength acid suppression therapy; or the presence of alarm symptoms.10
Numerous OTC options are available for patient-directed therapy, including antacids and alginic products.10 Antacids are available in many formulations and work by maintaining an intragastric pH of more than four, and all have approximately equal efficacy.10 Alginic acid is a component of some antacid products and works to form a viscous solution that stays on the surface of gastric contents and provides a protective barrier for the esophagus.10 Alginate products may be useful for patients with once-daily PPI therapy who have residual symptoms.10,24 Patients should be counseled to use antacids only for milder GERD symptoms, and those who are taking antacids chronically require further evaluation.10 Pharmacists should review patients’ current medication lists with pharmacy team members to ensure the use of antacids does not interact with other therapies because drug interactions are within the pharmacy technician's scope of practice. Clinically significant drug interactions include tetracycline, ferrous sulfate, isoniazid, sulfonylureas, and quinolone antibiotics.10 The specific interaction will depend on the dose,
dosage schedule, and formulation of the antacid.10 Examples of antacid products are detailed in Table 4.10
| Medication | Dose | Comments |
| Magnesium hydroxide/aluminu m hydroxide with simethicone | 10-20 mL as needed or after meals and at bedtime | If symptoms are unrelieved with lifestyle modifications and nonprescription medications after two weeks, patients should seek medical attention; do not exceed 16 teaspoons per 24 hours. |
| Antacid/alginic acid | 2-4 tablets or 10-20 mL after meals and at bedtime | Note: The content of alginic acid varies greatly among products; the higher the alginic acid, the better (at least 500 mg). |
| Calcium carbonate | 500 mg, 2-4 tablets as needed |
Table 4 Antacid Therapy10
Patients also have the option to utilize nonprescription H2RAs, including cimetidine, famotidine, and nizatidine, and PPIs (esomeprazole, omeprazole, omeprazole with sodium bicarbonate, and lansoprazole).10 Histamine-2 receptor antagonists exert their effect via competitive inhibitor of histamine at H2 receptors in the gastric parietal cells, which leads to inhibition of gastric acid secretion.10 These agents are useful when taken prior to meals and have beneficial effects on GERD symptoms related to exercise.10 They have a longer duration of action but a shorter onset of action compared to antacids.10
Proton pump inhibitors work by blocking gastric acid secretion via inhibiting H+/K+ adenosine triphosphate in gastric parietal cells.10 This results in antisecretory effects that are long-lasting.10 Nonprescription PPIs are
available as short-term therapies.10 Nonprescription H2RAs and PPIs are detailed in Table 5.
| Medication | Dose | Comments |
| Cimetidine | 200 mg | If symptoms are unrelieved with lifestyle modifications and nonprescription medications after two weeks, the patient should seek medical attention. |
| Famotidine | 10-20 mg | |
| Nizatidine | 75 mg | |
| Esomeprazole | 20 mg | If symptoms are unrelieved with lifestyle modifications and nonprescription medications after two weeks, the patient should seek medical attention. |
| Lansoprazole | 15 mg | |
| Omeprazole | 20 mg | |
| Omeprazole/sodium bicarbonate | 20 mg/1,100 mg |
Table 5 Nonprescription H2RAs and PPIs
Acid Suppression Therapy
Both PPIs and H2RAs are also available as prescription-strength products for the treatment of GERD. In general, PPIs are superior regarding symptom relief and healing rates.2
PPIs
Dexlansoprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, and omeprazole (with or without bicarbonate) are available as prescription PPIs.10 All agents within this class of medication have similar efficacy rates.25 The acid-suppression potencies of the PPIs can be standardized to omeprazole equivalents (OEs), with omeprazole having an OE of one.2 These are detailed in Table 6.2
Table 6 Omeprazole Equivalencies2
| PPI | OE |
| Pantoprazole | 0.23 |
| Lansoprazole | 0.90 |
| Omeprazole | 1.00 |
| Esomeprazole | 1.60 |
| Rabeprazole | 1.82 |
Proton pump inhibitors are typically prescribed for 8-12 weeks, as healing tends to peak within that time frame.2 While the standard course of therapy is once-daily dosing, twice-daily PPI dosing may be needed in patients who do not respond to once-a-day therapy.2,10 Patients should be counseled to take their PPI 30-60 minutes before the largest meal of the day (with the exception of dexlansoprazole, which can be taken without regard to meals), and adherence to this regimen should be assessed prior to increasing the dose.2,10 Dexlansoprazole is a dual delayed-release PPI that is absorbed in the duodenum and then the small bowel.2 Bedtime dosing is not encouraged as this is less effective than taking the medication before a meal.2
If twice-daily dosing is initiated, patients should take the second dose 10-12 hours after the first dose and prior to a meal or snack.2,10 Alternatively, a different PPI could be started for patients who only partially respond to therapy.2,10 Notably, more than one switch is not recommended per ACG.2 If patients respond to short-course therapy, the PPI can be discontinued or titrated to the lowest effective dose.2,26
Common side effects of PPIs include headache, diarrhea, nausea, and abdominal pain.2,10 Outside of these adverse effects, there is growing concern related to the safety of PPI use.2,10 More serious side effects associated with their use include community-acquired pneumonia with short-term use and enteric infections, vitamin B12 deficiency, hypomagnesemia, and bone fractures with long-term use.2,27,28 Currently, no data supports taking vitamin B12, calcium, or magnesium above recommended doses, and screening of serum creatinine, magnesium, and vitamin B12 is also not standard of care.2
Long-term use of PPIs may also put patients at risk of chronic kidney disease due to acute interstitial nephritis, diabetes, and hypomagnesemia.27 In one study, CKD occurred in 3.68% of patients on PPIs over five years.29 The development of PPI-induced hepatic encephalopathy is also a risk.29
Pharmacists should counsel patients on potential drug interactions and thoroughly review medication lists to avoid such issues. PPIs interact with ketoconazole and itraconazole as they decrease the absorption of these medications.2 PPIs also inhibit CYP2C19, more specifically omeprazole, and thus can decrease the effectiveness of clopidogrel by preventing the conversion from the prodrug to active metabolite.30
H2RAs
Cimetidine, famotidine, and nizatidine are available in prescription- strength doses to treat mild-to-moderate GERD.2,10 All agents have similar efficacy.10 Numerous factors can affect the efficacy of these drugs, including the severity of GERD, the dosage regimen selected, and the duration of therapy.10 Higher doses of H2RAs could be trialed for patients who remain symptomatic, but there is less evidence to support this, and these regimens are often more expensive for patients compared to PPIs.2,10
Patients on these regimens should be monitored for side effects and screened for potential drug interactions.10 Cimetidine can interact with numerous medications, including theophylline, warfarin, phenytoin, nifedipine, and propranolol.10 This agent should not be utilized if patients take one or more of these medications.10 Common side effects associated with H2RAs include headache, fatigue, dizziness, and constipation or diarrhea.10
Table 7 reviews the prescription-strength H2RAs and PPIs. It reviews their recommended dosages and discusses guidelines depending on a patient’s symptoms and response to medication therapy.
Table 7
Prescription-strength H2RAs and PPIs10
| Prescription-strength H2RAs | ||
| Medication | Dose | Notes |
| Cimetidine (off- label use) | 400 mg four times daily or 800 mg twice daily | For typical symptoms, treat empirically with prescription- strength acid suppression therapy. If symptoms recur, consider maintenance therapy. Note: Most patients will require standard doses for maintenance therapy. |
| Famotidine | 20 mg twice daily | |
| Nizatidine | 150 mg twice daily | |
| Prescription-strength PPIs | ||
| Dexlansoprazole | 30 mg once daily for four weeks | For typical symptoms, treat empirically with prescription- strength acid suppression therapy. Patients with moderate-to-severe symptoms should receive a PPI as initial therapy. If symptoms recur, consider maintenance therapy. |
| Esomeprazole | 20-40 mg once daily | |
| Lansoprazole | 15 mg once daily | |
| Omeprazole | 20 mg once daily | |
| Omeprazole/sodium bicarbonate | 20 mg once daily | |
| Pantoprazole (Off- label use) | 40 mg once daily | |
| Rabeprazole | 20 mg once daily | |
Healing of erosive esophagitis or treatment of patients with moderate-to-severe symptoms or complications (individualized lifestyle modifications + high-dose H2RAs or PPIs or antireflux surgery) | ||
| Individualized lifestyle modifications | Lifestyle modifications should be individualized for each patient. | |
| PPIs (up to twice daily for up to 8 weeks) | ||
| Dexlansoprazole | 60 mg daily | For extraesophageal or alarm symptoms, obtain an endoscopy with a biopsy to evaluate mucosa. If symptoms are relieved, consider maintenance therapy. PPIs are the most effective maintenance therapy for patients with extraesophageal symptoms, complications, and erosive disease. Start with twice-daily |
| Esomeprazole | 20-40 mg daily | |
| Lansoprazole | 30 mg once or twice daily | |
| Omeprazole | 20 mg once or twice daily | |
| Rabeprazole | 20 mg once or twice daily | |
| Pantoprazole | 40 mg once or twice daily | |
PPI therapy if reflux chest syndrome is present. Patients not responding to pharmacologic therapy, including those with persistent extraesophageal symptoms, should be evaluated via manometry and/or ambulatory reflux monitoring. | ||
| High-dose H2RAs (for 8-12 weeks) | ||
| Cimetidine | 400 mg four times daily or 800 mg twice daily | Note: If high-dose H2RA is needed, may consider using PPI to lower cost, increase convenience, and increase tolerability. Note: Four times daily H2RA is considered off-label use for nizatidine. |
| Famotidine | 20-40 mg twice daily | |
| Nizatidine | 150 mg two to four times daily | |
Promotility agents
Certain promotility medications can be used adjunctly in patients who have a known motility defect, such as LES incompetence.10 This group includes metoclopramide and bethanechol.2 Both agents are associated with significant side effects, and there is little data supporting their effectiveness as acid suppression therapies.2,10
Mucosal protectants
Sucralfate is a nonabsorbable aluminum salt of sucrose octasulfate. While it can be used to manage radiation esophagitis or nonacid reflux GERD, it is not particularly useful in treating acid reflux.2
Maintenance Therapy
Long-term acid reflux therapy may be required for a subset of patients, including those with moderate-to-severe GERD, erosive disease, or Barrett’s esophagus.2
Surgical and Endoscopic Interventions
Patients who require indefinite PPI therapy but prefer to avoid long-term medication use or patients who are nonresponders to medication therapy may benefit from surgical or endoscopic interventions.2 Antireflux surgery is recommended if patients have severe reflux esophagitis, large hiatal hernias, or persistent or troublesome GERD symptoms.2 It is critical to identify the cause of refractory GERD symptoms prior to surgery.2 Details regarding antireflux surgeries and endoscopic treatments are detailed in Table 8.2,13
Table 8. Surgical and Endoscopic Interventions2,13
| Antireflux Surgeries | |
| Fundoplication | The gold standard of antireflux procedure. It improves LES pressure and decreases esophagus exposure to acid. |
| Magnetic sphincter augmentation | Less invasive option. It improves LES function and reduces the retrograde flow of acid into the esophagus. |
| Endoscopic Treatments | |
Transoral incisionless fundoplication | It is considered for patients without severe reflux esophagitis or hiatal hernias larger than 2 cm who prefer to avoid antireflux surgery. |
| Radiofrequency | It is not recommended per ACG guidelines |
Tips for Pharmacy Technicians
Pharmacy technicians are important members of the healthcare team. Oftentimes, patients may come to the pharmacy seeking treatment for GI- related symptoms, and pharmacy technicians can assist pharmacists in identifying patients who may have GERD or be candidates for referral. Pharmacy technicians can also recognize when patients may or may not be adherent to GERD therapies and assist pharmacists in recognizing and helping these patients.
Summary
Gastroesophageal reflux disease, or GERD, is a chronic gastrointestinal disorder that results in regurgitation of gastric contents into the esophagus. GERD has long been one of the most common gastrointestinal diseases encountered by healthcare providers. In recent years, clinicians' knowledge regarding the differing presentations of GERD, new diagnostic modalities, and approaches to patient management has evolved and changed. A patient- centered approach that considers lifestyle, pharmacologic, surgical, and endoscopic management is key to optimizing outcomes. Changes to management approaches are summarized in the 2021 American College of Gastroenterology (ACG) guidelines for GERD.
Pharmacists are readily accessible health providers who can assist patients in selecting optimal short-term GERD treatments. Thus, pharmacists should have a thorough understanding of available over-the-counter treatment options and be able to select appropriate agents specific to each patient. Pharmacists should also be able to recognize GERD alarm symptoms and refer patients to their healthcare provider when appropriate.
Course Test
What is the primary physiologic cause of GERD for most patients?
Decreased gastric acid production
Esophageal distention
Transient lower esophageal sphincter relaxation (TLESR)
Hiatal hernias
What is a risk factor associated with the development of GERD?
High physical activity
Increased salivary production
Older age
Nonsmokers
Which symptoms are most specific and sensitive for GERD?
Noncardiac chest pain and nausea
Chronic cough and dyspnea
Heartburn and regurgitation
Odynophagia and incontinence
Which of the following symptoms of GERD should raise concern for a more serious underlying issue such as malignancy?
Weight gain
Chronic cough
Dysphagia
Sore throat
Which of the following approaches works best to reduce GERD symptoms and the frequency of reflux, heal GERD injury, and prevent complications?
Decreasing LES pressure
Increasing gastric volume available for reflux
Slowing gastric emptying
Enhancing esophageal acid clearance
What is the safest, most cost-effective diagnostic tool for GERD for the majority of patients who do not have alarm features?
Barium esophagram
Clinical history
Ambulatory pH monitoring
Wireless pH monitoring
Which of the following lifestyle modifications is generally recommended for managing GERD?
Avoid carbonated beverages
Consuming caffeinated beverages
Weight gain
Larger meals
What is the recommended course of action for patients with mild, intermittent GERD symptoms who do not respond to self-care measures within two weeks?
Quadruple the dose of antacids
Continue self-care measures for another twelve weeks
Seek further medical attention
Switch to calcium carbonate
Which of the following promotility medications is not effective at suppressing acid and can cause significant side effects?
Metoclopramide
Omeprazole
Esomeprazole
Cimetidine
Which scenario would a pharmacy technician likely refer to a pharmacist?
The patient presents to the pharmacy counter with a glaucoma eye drop prescription and Tums
The patient presents to the pharmacy counter with a tetracycline prescription and TUMS (calcium carbonate)
The patient presents to the pharmacy counter with a gallon of milk and iron tablets
The patient presents to the pharmacy counter with an insulin prescription and a jar of instant coffee.
References
Shaqran TM, Ismaeel MM, Alnuaman AA, et al. Epidemiology, Causes, and Management of Gastro-esophageal Reflux Disease: A Systematic Review. Cureus. 2023;15(10):e47420. Published 2023 Oct 21. doi:10.7759/cureus.47420
Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol. 2022;117(1):27-56. doi:10.14309/ajg.0000000000001538
El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014 Jun;63(6):871-80.
Locke GR, 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ., 3rd Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County,
Minnesota. Gastroenterology. 1997;112:1448–1456.
Kim YS, Kim N, Kim GH. Sex and gender differences in gastroesophageal reflux disease. J Neurogastroenterol Motil. 2016;22(4):575–588. doi: 10.5056/jnm16138
Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Gut. 2018;67:430–440
Eusebi LH, Ratnakumaran R, Yuan Y, et al. Global prevalence of and risk factors for gastro-oesophageal reflux symptoms: A meta- analysis. Gut. 2018;67(3):430–440. doi: 10.1136/gutjnl-2016-313589
Clarrett DM, Hachem C. Gastroesophageal Reflux Disease (GERD). Mo Med. 2018;115(3):214-218.
Park S, Weg R, Enslin S, Kaul V. Ten things every gastroenterologist should know about antireflux surgery. Clin Gastroenterol
Hepatol. 2020;18:1923–1929. doi: 10.1016/j.cgh.2020.02.041
May D, Lavender DL, Rao SC. Gastroesophageal Reflux
Disease. In: DiPiro JT, Yee GC, Haines ST, Nolin TD, Ellingrod VL, Posey
L. eds. DiPiro’s Pharmacotherapy: A Pathophysiologic Approach, 12th Edition. McGraw Hill; 2023.
Tutuian R; Clinical Lead Outpatient Services and Gastrointestinal Function Laboratory. Adverse effects of drugs on the esophagus. Best Pract Res Clin Gastroenterol. 2010;24(2):91-97. doi:10.1016/j.bpg.2010.02.005
Wikicommons. GERD. https://commons.wikimedia.org/wiki/Category:Gastroesophageal_reflux
_disease#/media/File:GERD.png. Accessed January 4, 2024.
Smith W, Davila N. Gastroesophageal reflux disease: 2021 guideline updates and clinical pearls. Nurse Pract. 2023;48(7):24-25. doi:10.1097/01.NPR.0000000000000065
Cremonini F, Wise J, Moayyedi P, et al. Diagnostic and therapeutic use of proton pump inhibitors in non-cardiac chest pain: A metaanalysis. Am J Gastroenterol. 2005;100(6):1226–32.
Kahrilas PJ, Hughes N, Howden CW. Response of unexplained chest pain to proton pump inhibitor treatment in patients with and without objective evidence of gastro-oesophageal reflux disease. Gut. 2011;60(11):1473–8.
Wikicommons. EGD. https://commons.wikimedia.org/wiki/Category:Esophagogastroduodeno scopy#/media/File:Endoscopy_start.jpg. Accessed on January 4, 2024.
Katz LC, Just R, Castell DO. Body position affects recumbent postprandial reflux. J Clin Gastroenterol. 1994;18(4):280-283. doi:10.1097/00004836-199406000-00004
Khoury RM, Camacho-Lobato L, Katz PO, et al. Influence of spontaneous sleep positions on nighttime recumbent reflux in patients with gastroesophageal reflux disease. Am J Gastroenterol. 1999;94(8):2069–73.
Ness-Jensen E, Lindam A, Lagergren J, et al. Tobacco smoking cessation and improved gastroesophageal reflux: A prospective population-based cohort study: The HUNT study. Am J Gastroenterol 2014;109(2):171–7.
El-Serag HB, Satia JA, Rabeneck L. Dietary intake and the risk of gastro-oesophageal reflux disease: A cross sectional study in volunteers. Gut 2005;54(1):11–7.
Newberry C, Lynch K. The role of diet in the development and management of gastroesophageal reflux disease: Why we feel the burn. J Thorac Dis. 2019;11(Suppl 12):S1594–601.
Mehta RS, Song M, Staller K, et al. Association between beverage intake and incidence of gastroesophageal reflux symptoms. Clin Gastroenterol Hepatol. 2020;18(10):2226–33.e4
Ness-Jensen E, Hveem K, El-Serag H, et al. Lifestyle intervention in gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2016;14(2):175–82.e1–3
Reimer C, Lodrup AB, Smith G, et al. Randomised clinical trial: Alginate (Gaviscon Advance) vs placebo as add-on therapy in reflux patients with inadequate response to a once daily proton pump inhibitor. Aliment Pharmacol Ther. 2016;43:899–909. doi: 10.1111/apt.13567
Sandhu DS, Fass R. Current trends in the management of gastroesophageal reflux disease. Gut Liver. 2018;12(1):7–16. doi: 10.5009/gnl16615
Kim J, Blackett JW, Jodorkovsky D. Strategies for effective discontinuation of proton pump inhibitors. Curr Gastroenterol Rep. 2018;20(6):27. doi: 10.1007/s11894-018-0632-y
Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017;152(4):706-715. doi:10.1053/j.gastro.2017.01.031
Gyawali CP. Proton pump inhibitors in gastroesophageal reflux disease: Friend or foe. Curr Gastroenterol Rep. 2017;19:46. doi: 10.1007/s11894-017-0586-5
Vaezi MF, Yang YX, Howden CW. Complications of proton pump inhibitor therapy. Gastroenterology. 2017;153:35–48. doi: 10.1053/j.gastro.2017.04.047
Bouziana SD, Tziomalos K. Clinical relevance of clopidogrel-proton pump inhibitors interaction. World J Gastrointest Pharmacol Ther. 2015;6(2):17-21. doi:10.4292/wjgpt.v6.i2.17
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.