SHAPING FUTURES: PHARMACY’S ROLE IN PEDIATRIC OBESITY
KELSEY GIARA, PharmD, RPh
Kelsey Giara is a New Hampshire-based pharmacist and freelance medical writer. She writes about a variety of healthcare topics for various publications with significant experience in continuing medical education, needs assessments and grant writing, and medical communications.
Topic Overview
Recent studies indicate that nearly one in five children and adolescents in the United States are affected by obesity, setting the stage for a potential health crisis. As obesity rates rise in the pediatric population, so do other medical conditions and chronic diseases. They include asthma, sleep apnea, fatty liver disease, gallstones and gallbladder disease, cardiovascular diseases, joint problems, menstrual abnormalities, metabolic diseases, and skin diseases. These conditions were more commonly seen in adulthood in prior decades. Not surprisingly, pediatric obesity leads to obesity in adulthood. Pharmacists and pharmacy technicians with a deep understanding of the diagnosis and screening, physical and mental burden, and available treatment options for obesity can make a significant difference in care and outcomes for this vulnerable patient population.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-187-H01-P
Pharmacy Technician 0669-0000-23-188-H01-T
Credits: 2 contact hours of continuing education credit
Type of Activity: Application
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 contact hours, including Course Test and course evaluation
Release Date: November 18, 2023 Expiration Date: November 18, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From November 18, 2023, through November 18, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Discuss the growing prevalence and burden of pediatric obesity
Describe the immediate and long-term risks of obesity in childhood and adolescence
Demonstrate the pharmacy team’s role in optimizing care for pediatric patients with obesity
Disclosures
The following individuals were involved in developing this activity: Kelsey Giara, PharmD, PharmD, RPh, and Pamela Sardo, PharmD, BS. Pamela Sardo was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
In a world where video screens are replacing playgrounds and convenient, fast foods trump nutrition, the prevalence of pediatric obesity has reached staggering proportions and is expected to continue rising. Managing and treating pediatric obesity is challenging because of the increasing prevalence and because it involves addressing emotional and physical conditions. As part of a collaborative healthcare team, pharmacists and pharmacy technicians can help young people with obesity reduce their weight and improve their health, leading to a better quality of life and future.
Prevalence of Pediatric Obesity
Recent studies indicate that nearly one in five children and adolescents in the United States (U.S.) are affected by obesity, setting the stage for a potential health crisis.1 Obesity prevalence increases with age. In 2015–2016, about 13.9%, 18.4%, and 20.6% of children aged 2 to 5 years, 6 to 11 years, and 12 to 19 years had obesity, respectively.2
Evidence also suggests that despite efforts to tackle this issue, obesity’s incidence is still increasing.3 The coronavirus disease-19 pandemic significantly amplified obesity’s effect on children. The pandemic period was associated with a doubling in the rate of BMI increase compared to pre- pandemic.2 Major disparities are also noted among children and adolescents with obesity, including lower parental education level, lower income, less access to healthier food options and safe physical activity opportunities, and greater incidence of adverse childhood experiences.2 Obesity prevalence also varies across ethnic and racial groups, with non-Hispanic Black children, Mexican American youth, and American Indian and Alaska Native children and adolescents experiencing higher rates of obesity compared to non-Hispanic white counterparts.2
Often, individuals shy away from addressing obesity in children for fear of introducing self-esteem issues or even disordered eating (e.g., anorexia, bulimia, binge/emotional eating). However, studies indicate the opposite.
While obesity and self-guided dieting put youth at high risk of weight fluctuation and disordered eating, supervised, evidence-based weight management decreases the incidence of eating disorders (EDs) immediately and for up to 6 years post-treatment.2 Pharmacists and pharmacy technicians should be well versed in updated guidelines and recommendations for obesity management in pediatric patients to improve care and outcomes for this vulnerable population.
Obesity Diagnosis and Screening in Pediatrics
Defining overweight and obesity in children requires consideration of body mass index (BMI).4,5 Body mass index is a measurement of physical characteristics of the human body calculated by dividing a person’s weight (in kilograms) by the square of their height (in meters).
The BMI works well in adult populations; however, using BMI to measure childhood obesity is challenging, given that a child’s body shape changes as the child progresses through normal growth.6 Body mass index only considers weight and height, which fails to differentiate between fat and fat-free mass (i.e., muscle and bone) and could exaggerate obesity measurements in large, muscular children. Clinicians often use BMI, waist circumference, and skin- fold thickness in practice. While these are less accurate than research methods, they are reasonable methods of identifying risk. Several other methods measure a person’s percentage of body fat: underwater weighing (densitometry), multi-frequency bioelectrical impedance analysis, and magnetic resonance imaging; however, they are not readily used in practice.6 Despite its limitations, BMI is the most suitable clinical tool for screening excess adiposity and diagnosing overweight or obesity. Annual BMI measurement during well-child visits is recommended for tracking childhood overweight and obesity, though it may miss short-term weight changes.2
The Centers for Disease Control and Prevention (CDC) has a BMI calculator specific to pediatric patients called the BMI Percentile Calculator for Child and Teen.5 The CDC’s BMI Percentile Calculator for Child and Teen may be found at https://www.cdc.gov/healthyweight/bmi/calculator.html.
Given that pediatric patients are actively growing, the ranges of height, weight, and BMI considered “normal” or “healthy” vary by age and sex.4 Before age 2, providers do not assess BMI; rather, they compare the infant’s weight and length percentiles separately.7 For pediatric patients aged 2 years and older, providers consider BMI relative to others of the same sex and age, expressed as a percentile.4,7 This percentile represents the percentage of children in the reference population (i.e., those of the same age and sex) who have a lower BMI than the child being assessed. For example, if a child’s BMI falls at the 75th percentile, it means that the child’s BMI is higher than 75% of children of the same age and gender. Table 1 lists percentiles and BMIs used to diagnose pediatric patients with overweight or obesity.
Table 1
Pediatric BMI Categories2,4
| BMI Category | Associated Percentile or BMI |
Underweight |
< 5th percentile |
Healthy weight |
5th percentile to < 85th percentile |
Overweight |
85th percentile to < 95th percentile |
Obesity |
≥ 95th percentile |
Class 2 Obesity* |
≥ 120% to < 140% of the 95th percentile OR BMI ≥ 35 kg/m2 to < 40 kg/m2 |
Class 3 Obesity* |
≥ 140% of the 95th percentile OR BMI ≥ 40 kg/m2 |
*Also referred to as severe obesity. BMI, body mass index.
Causes of Childhood Obesity
Obesity’s causes are complex and multifactorial; individuals’ genetics, lifestyle choices, and medication use all contribute.1,6 Studies show that having an overweight mother and living in a single-parent household are associated with pediatric overweight and obesity.6 Social determinants of health, including childcare and school environments, neighborhood design, food security, and access to safe, convenient physical activity, also greatly impact the development of overweight and obesity in this population.1,6
Increased obesity is largely a result of an imbalance between energy intake and expenditure, but increasing evidence shows that genetics are a strong predictor of obesity risk. Some studies suggest that BMI is 40% to 70% inherited, but less than 5% of childhood obesity cases are genetic.2,6 Additionally, people who are obese tend to have lower basal metabolic rates (i.e., metabolism at rest) than those of a healthy weight. Various dietary habits contribute to the development of obesity, including fast food consumption, sugary beverages, snacking, and portion sizes:6
Fast food restaurant menus often feature meals with a substantial calorie count but limited nutritional content. Some families, particularly those with both parents employed outside the home, choose fast food establishments because their children prefer them, and they offer a combination of convenience and affordability.6
Often, individuals only consider soda as a sugary drink and fail to recognize that juice and other sweetened beverages fall into this category, too.6 These are all less filling and consumed quicker than food, resulting in higher caloric intake.
Over the past decade, portion sizes have drastically increased, as has frequent snacking on high-calorie foods like chips, baked goods, and candy.6 These create energy imbalances leading to weight gain and, consequently, obesity.
Other lifestyle factors contributing to obesity include activity level, environmental influences, and socio-cultural factors:6
A sedentary lifestyle is one of the most significant risk factors for obesity. “Screen time” is a term used to describe watching TV, and using or viewing computers, videos or video games, mobile phones, and other digital devices. Television (TV) and screen use have increased drastically in recent years; each additional hour of TV per day is associated with a 2% greater risk of childhood obesity.6 Additionally, children who watch TV tend to consume more of the advertised goods, including sweetened cereals, sugary beverages, and salty snacks.6 Studies indicate that screen time greater than 2 hours per day is associated with a 42% higher risk of overweight and obesity.2
Opportunities to be physically active and safe environments to do so have decreased in recent years. Parents are more likely to drive their children to school than they used to be, and children who live in unsafe areas or who lack access to safe, well-lit walking routes have less opportunity for physical activity.6
In today’s society, people tend to use food as a reward, to control others, and as part of socialization.6 This encourages unhealthy relationships with food, thus increasing the risk of obesity.
Medications commonly implicated in pediatric weight gain include glucocorticoids, sulfonylureas, insulin, thiazolidinediones, antipsychotics, tricyclic antidepressants, and antiepileptic drugs.2 Second-generation antipsychotics (e.g., aripiprazole, clozapine, risperidone, quetiapine) are associated with rapid weight gain and comorbidities (e.g., diabetes, dyslipidemia).
The intricate pathophysiology of childhood obesity introduces significant challenges to effective treatment. Understanding the multifaceted factors
contributing to obesity in children complicates the development of tailored interventions and hinders successful outcomes.
Defining the Burden of Pediatric Obesity
Children and adolescents with obesity are at increased risk for many serious diseases and health conditions compared to those with a healthy weight. They also suffer significant mental health consequences.
Physical Health Consequences
As obesity rates rise, so do other medical conditions and chronic diseases. Pediatric obesity increases the risks of the following:6,8
breathing problems (e.g., asthma, sleep apnea)
fatty liver disease
gallstones and gallbladder disease
cardiovascular diseases (e.g., hypertension, hypercholesterolemia)
joint problems (e.g., osteoarthritis, musculoskeletal pain, impaired balance)
menstrual abnormalities (e.g., polycystic ovarian syndrome [PCOS])
metabolic diseases (e.g., glucose intolerance, insulin resistance, type 2 diabetes mellitus [T2DM])
obesity in adulthood
skin conditions
Until recently, many of these diseases were found only in adults, but now they are notably present in pediatric patients with obesity.6 While most are preventable and can disappear when a child reaches a healthy weight, some maintain negative consequences through adulthood. Obesity also increases the risk of developing some forms of cancer.6,8
Diabetes, sleep apnea, and cardiovascular disease are the most common health problems associated with childhood obesity.6 The incidence of diabetes among pediatric patients with diabetes is greater among children
aged 10 years or older, those in early pubertal stages, and those with a family history of T2DM.2
Mental Health Impact
Children and adolescents with obesity are at increased risk of mental illness (e.g., anxiety, depression), low self-esteem, worse quality of life, and social problems.8 Psychiatric comorbidities are common in young people with obesity and include a range of mood, anxiety, substance use, somatoform (physical symptoms unexplained by an underlying medical condition), and eating disorders. Studies report elevated lifetime rates for mood (42.6%), anxiety (40.4%), substance use (36.2%), somatoform (14.9%), and eating disorders (17.0%) compared with the general population.9
The most consistently reported psychiatric condition related to obesity is depression.9 Children 18 years and younger with obesity are 32% more likely to have or develop depression compared to those of healthy weight.2 The highest prevalence of depression (44%) is seen among females with obesity.
Medications used to treat mental health conditions (e.g., selective serotonin reuptake inhibitors, antipsychotics) can also cause weight gain, further complicating this relationship.9
Experts have described obesity as “one of the most stigmatizing and least socially acceptable conditions in childhood.”10 Pediatric patients with obesity face significant hardships, including negative stereotypes, discrimination, bullying, and social marginalization.6 They tend to have fewer friends than children of a healthy weight, resulting in less social interaction and play and more time spent in sedentary activities. In addition to weight- based harassment, youth with obesity are at increased risk for sexual harassment and harassment based on race/ethnicity, socioeconomic status, and gender.2 Racism is also associated with an increased prevalence of obesity.2
Research shows that individuals as young as 2 years old experience weight-related discrimination.11 They frequently encounter exclusion from various activities, especially competitive ones requiring physical exertion.6 Children who are overweight frequently struggle to participate in physical activities due to their slower pace compared to their peers and difficulty in managing breathlessness. These social challenges, in turn, erode their self- esteem, diminish their self-confidence, and contribute to negative body image.
Collectively, these adverse consequences of overweight and obesity can have profound and detrimental effects on children and adolescents. This can also trigger a vicious cycle wherein children and adolescents protect themselves from bullying and stigma by retreating to safe places, such as their homes, where they often seek comfort in food.6
This can also extend to impact academic performance; children who are overweight and obese are four times more likely to report problems at school than those of a healthy weight.10 Additionally, these children—particularly those with chronic health conditions like diabetes and asthma—are more prone to frequent school absences, further impacting academic performance.
Managing Pediatric Obesity
The American Academy of Pediatrics (AAP) compiled its first comprehensive guideline for the evaluation and treatment of pediatric obesity in 2023.2 Importantly, these guidelines only apply to patients aged 2 years and older because it is difficult to define and measure excess fat in patients younger than 2 years. The AAP notes that guidelines for the prevention of obesity are forthcoming and more appropriately applied to this younger population.
Lifestyle and Dietary Changes
As discussed, lifestyle and dietary factors greatly contribute to the development and worsening of pediatric obesity. As discussed, lifestyle and dietary factors greatly contribute to the development and worsening of
pediatric obesity. Promoting healthier habits supports positive outcomes for children and adolescents with obesity. Dietary and lifestyle modifications are crucial to mitigate the challenges posed by pediatric obesity. The figure below shows AAP-recommended behavior and lifestyle strategies. Other strategies with less evidence include avoidance of breakfast skipping, use of screen- based physical activity (exergames), and getting the appropriate amount of sleep for age.2
Evidence-Based Lifestyle Strategies for Pediatric Weight-Loss2
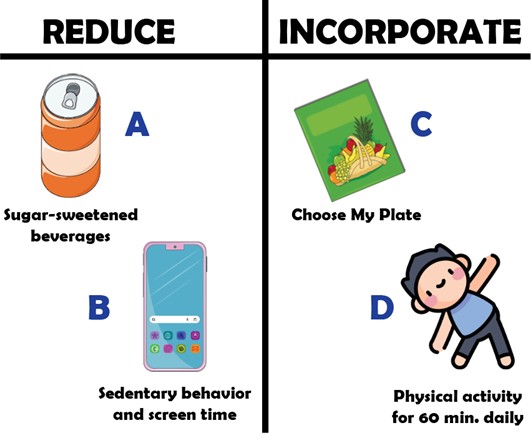
A) Higher intake of carbonated beverages, sweetened beverages, soda, sports drinks, and fruit drinks is associated with greater weight gain. B) AAP recommends no screen time before 18 months of age, a 1-hour limit for ages 2–5 years, and a goal of appropriate, not-excessive use without a defined upper limit in older children. C) MyPlate (www.choosemyplate.gov) is the US Department of Agriculture’s broad set of recommendations for healthy eating for Americans. D) Moderate-to-vigorous aerobic exercise for 60 minutes per day is associated with improved body weight in children and adolescents. (Figure partly generated using Servier Medical Art, provided by Servier, licensed under a Creative Commons Attribution 3.0 unported license and Freepik.
Specialized Care is Crucial
The AAP guidelines recommend prompt Intensive Health Behavior and Lifestyle Treatment (IHBLT) programs for pediatric patients with obesity.2 This involves multidisciplinary, intensive care from a multidisciplinary treatment team of primary care providers with training in obesity, dieticians, exercise specialists, and behavioral health professionals. Patients undergoing IHBLT receive longitudinal treatment, either inpatient or outpatient, ideally 26 or more contact hours for 3 to 12 months. Treatment can be individual, group- based, or a combination of both. Evidence is strongest for in-person treatment, but growing evidence suggests the utility of virtual therapy.2
Factors contributing to the effectiveness of IHBLT include active family engagement and sustained participation, which can enhance treatment outcomes.2 Pharmacists should explain the reasons for referrals, encourage active family participation, and schedule follow-up visits to monitor progress. It's important to manage expectations, as outcomes can vary widely among children. While some may not experience BMI improvement, those who do can expect modest declines of 1% to 3% in BMI percentile.2
Parental Influence
When advising patients and caregivers about nutrition and physical activity, pharmacists should note that children learn by modeling others.6 Availability of and repeated exposure to healthy foods is crucial to developing preferences. Evidence also suggests that families who eat meals together consume more healthy foods, whereas eating out or watching television while eating is associated with higher fat intake.6
Different parental feeding methods also affect children's attitudes towards food choices and their overall dietary habits. The AAP describes four general parenting styles related to feeding:2
Authoritative: responsive and warm with high expectations
Authoritarian: not responsive but with high expectations
Permissive or indulgent: responsive and warm but lenient with few rules
Negligent: not responsive with few rules
Studies show that the authoritative style of parenting is the preferred method for protecting against excessive weight gain.2,6 Under authoritative feeding, parents determine which foods are offered, allowing the child to choose, and providing the rationale for healthy options are associated with positive cognitions about healthy foods and healthier intake. Children from authoritative parenting homes tend to eat more healthy foods, be more physically active, and have healthier BMI compared with children raised in homes of other parenting styles.2
Authoritarian feeding, conversely, tends to initiate the opposite of its desired effect. Complete restriction of “junk food” is associated with an increased desire for unhealthy food, thus increased weight and BMI.6 Also, an authoritarian parent may not respond to a child’s cues for energy intake, negating the child’s ability to self-regulate their own energy intake and increasing the likelihood of overindulging when presented with the opportunity to eat.2
Pharmacologic Treatments
While IHBLT has the strongest evidence of effectiveness in the pediatric population, providers may offer children aged 8 to 11 years obesity pharmacotherapy to aid in weight loss.2 Pharmacists and pharmacy technicians should be familiar with the safe and effective use of weight-loss pharmacotherapy in this population. Most are used off-label for this indication; only two medications, phentermine, and orlistat, are FDA-approved for use in adolescent obesity.12 The AAP emphasizes that providers should never use pharmacotherapy alone for weight loss, and referral for IHBLT is still vital.2
FDA-Approved Therapies
Gastric and pancreatic lipases are enzymes involved in dietary fat digestion. Orlistat, an intestinal lipase inhibitor, blocks these enzymes’ activity to prevent the breakdown and absorption of fat consumed in the diet.2 Instead, undigested fat is excreted through the feces, leading patients to absorb fewer calories, thus introducing a calorie deficit that contributes to weight loss. Orlistat is U.S. Food and Drug Administration (FDA) approved for long-term treatment of obesity in individuals 12 years and older at 120 mg three times daily.2 However, the drug’s adverse events (AEs) — steatorrhea (fatty, bulky, foul-smelling stools), fecal urgency, and flatulence — greatly limit the drug’s tolerability and use in the pediatric population. Orlistat may also cause a deficiency of fat-soluble vitamins, so patients should take a daily multivitamin containing vitamins A, D, E, K, and beta-carotene.12,13
Phentermine, a central norepinephrine uptake inhibitor, also non- selectively inhibits serotonin and dopamine reuptake and reduces appetite.2 This drug is FDA-approved for short-course therapy (3 months) in adolescents aged 16 years and older. Patients take 7.5 mg, 15 mg, 30 mg, or 37.5 mg once daily for weight loss. While the drug’s AEs — elevated blood pressure, dizziness, headache, irritability, insomnia, tremor, dry mouth, and stomachache — are dose-dependent, effectiveness is not.2,12
Pharmacy teams should note that phentermine is a controlled substance, as it carries risks for dependence and abuse. Counsel patients and caregivers to do the following:
Understand the medication: Educate themselves about the prescribed medication, its purpose, and potential risks.
Monitor behavior and physical changes: Watch for sudden behavioral shifts or physical symptoms.
Secure medications: Keep the medication in a secure location to prevent unauthorized access.
Communicate openly: Maintain open dialogue with your child about their medication and encourage reporting of concerns.
Seek professional help: If misuse is suspected, contact a healthcare provider promptly for guidance and intervention.
Glucagon-like peptide-1 (GLP-1) is a hormone heavily involved in regulating blood sugar levels, hunger sensations, and satiety (the sensation of fullness). Glucagon-like peptide-1 receptors in the central nervous system are located in the hypothalamus, which is involved in regulating food intake.14 Initially developed to treat T2DM, GLP-1 receptor agonists, including dulaglutide, exenatide, liraglutide, and semaglutide, are also effective for weight loss. They decrease appetite and hunger sensations, delaying gastric emptying (the stomach's food release) and enhancing satiety following meals.14
Liraglutide is FDA-approved for long-term obesity treatment in children aged 12 years and older weighing more than 60 kg and with an initial BMI corresponding to 30 kg/m2 for adults by international cut-offs, regardless of the presence of T2DM.2 A recent randomized controlled trial found daily liraglutide injections, administered via daily injections, to be more effective than placebo in promoting weight loss among patients aged 12 years and older with obesity who did not respond to lifestyle interventions.15 This study reported a significant difference in body weight loss, approximately 4.5 kg, or a 5% BMI reduction after 1 year of treatment.
The recommended liraglutide starting dose is 0.6 mg subcutaneously daily for 1 week, and patients increase the dose in weekly intervals to a maximum maintenance dose of 3.0 mg per day.2,16 If pediatric patients do not tolerate an increased dose during dose escalation, providers should lower the dose back down to the previous level. Dose escalation for pediatric patients may take up to 8 weeks.16 Adverse events may include nausea and vomiting, with a slightly elevated risk of medullary thyroid cancer in patients with a family history of multiple endocrine neoplasia (inherited disorders causing endocrine tumors). Notably, two formulations of liraglutide exist, but only one (brand name Saxenda) is FDA-approved for pediatric patients.
Semaglutide, the newest GLP-1 receptor agonist, demonstrates promising results in adults with obesity, and the FDA approved the drug’s use in adolescence in December 2022.17 In the phase 3 STEEP TEENS placebo- controlled trial, patients in the semaglutide arm experienced a significant BMI decrease (16.1%) compared to a 0.6% BMI increase seen in the placebo group.17 The trial also showed that 77% of patients using semaglutide achieved a BMI reduction of 5% or more compared to only 20% of those in the placebo arm. Adverse events such as nausea, vomiting, diarrhea, headache, and abdominal pain were similar to those seen in adults, but adolescents were also more likely to experience gallbladder problems, including gallstones, low blood pressure, rash, and itching compared to adult studies.17
Patients inject semaglutide subcutaneously once weekly on the same day each week, at any time of the day, with or without meals.18 Patients start at 0.25 mg once weekly for 4 weeks, then increase the dose in 4-week intervals until they reach the 2.4 mg weekly maintenance dose. Semaglutide is also available in an oral formulation, but the oral formulation is not approved in pediatric or non-T2DM cases of obesity.19
Off-Label Therapies
Topiramate is a carbonic anhydrase inhibitor approved for children 2 years and older with epilepsy and for headache prevention in children aged
12 years and older. The drug also suppresses appetite through unclear mechanisms and is FDA-approved for binge eating disorder in adults.2 Providers should use the drug with caution in children, as topiramate’s major AE is cognitive slowing, which can interfere with academic concentration and other aspects of daily life. The drug can also cause birth defects if a patient falls pregnant, so reliable birth control is critical for adolescents using the drug.2
Phentermine and topiramate are available as a combination product approved for weight loss in adults, and recent data suggests it may have promising utility in adolescence. One study evaluated the combination in
adolescents aged 12 to 17 who had a documented history of struggling to lose or maintain weight during a lifestyle modification program, with a mean age of 14 years and a mean BMI of 37.8 kg/m2.20 Those who received the high- dose treatment (15 mg/92 mg) had a BMI percent change of -10.44 at 56 weeks, while the mid-dose group (7.5 mg/46 mg) had a change of -8.11, compared to the placebo group. Additionally, treatment led to improved cholesterol levels, and there were no significant differences in AEs between the treatment and placebo groups in the high- and mid-dose ranges.20
Many individuals use metformin, an antidiabetic agent used in patients
10 years and older, off-label for various other indications, including prediabetes, PCOS, and prevention of weight gain when using atypical antipsychotic drugs.2 Metformin decreases glucose production in the liver, decreases intestinal glucose absorption, and increases insulin sensitivity, thus reducing blood glucose levels. Studies show that adolescents taking metformin ER (extended-release) 2000 mg daily reduced BMI by about 1 kg/m2 compared to a slight BMI increase shown in teens in a lifestyle-only program.21
Metformin is available in immediate- and extended-release formulations and the recommended starting dose is 500 mg once or twice daily. Providers can gradually increase up to a maximum daily dose of 2500 mg.2 Gastrointestinal AEs such as bloating, nausea, flatulence, and diarrhea, are most common and dose-dependent (i.e., higher dose leads to more AEs). Given its limited and inconsistent efficacy, providers should consider metformin as a supplementary option when combined with IBHLT, particularly when other indications for use apply.2
Exenatide, a GLP-1 receptor agonist administered through weekly injections, is FDA-approved for children aged 10 to 17 years with T2DM. Studies have demonstrated varying degrees of BMI reduction (ranging from 0.9 to 1.18 kg/m2) in children as young as 8 years.2 However, it is also associated with significant AEs, including nausea, hypoglycemia, diarrhea, and other gastrointestinal upset.22 The drug is not approved for patients with obesity without T2DM.
Melanocortin 4 (M4) receptors in the brain regulate hunger, satiety, and energy expenditure.2 Setmelanotide, an M4 receptor agonist, is FDA-approved for chronic weight management in patients 6 years and older with monogenic or syndromic obesity due to genetic medical conditions.23 Patients with the indicated genetic conditions experience hyperphagia, a feeling of extreme, insatiable hunger. The daily dose is 1 to 3 mg subcutaneously once daily, and results in weight loss of 12% to 25% over 1 year in a small, uncontrolled study of patients with these rare deficits.2 Setmelanotide may cause skin hyperpigmentation, injection site reactions, nausea, headache, diarrhea, abdominal pain, vomiting, depression, and spontaneous penile erection. The drug is not indicated for use in patients with general obesity.23
Providers use lisdexamfetamine. Lisdexamfetamine is a stimulant indicated for attention-deficit/hyperactivity disorder (ADHD) in children 6 years and older and binge eating disorder in adults. It is used off-label for children with obesity.2 The drug’s mechanism of action for weight loss is like that of phentermine’s. The AAP indicates that insufficient evidence exists for lisdexamfetamine use for weight loss in pediatric patients, but pharmacists should recognize that some providers may still prescribe it for this purpose.2 Notably, lisdexamfetamine is also a controlled substance and carries risks for dependence similar to phentermine.
Metabolic and Bariatric Surgery
The most severe forms of pediatric obesity — those that fall into class 2 severe obesity or worse — represent an “epidemic within an epidemic.”2 Large, well-designed prospective observational studies have compared adolescents who undergo bariatric surgical treatment to nonsurgical controls. Data suggest that weight loss surgery is safe and effective for pediatric patients.2 Eligibility for weight loss surgery relies heavily on shared decision-making between the surgery team, the patient, and the patient’s caregivers, but initial criteria include the following:2
Class 2 obesity: clinically significant disease, including (but not limited to) T2DM, nonalcoholic fatty liver disease, gastroesophageal
reflux disease, obstructive sleep apnea, cardiovascular disease risks (hypertension, hyperlipidemia, insulin resistance), and depressed health-related quality of life
Class 3 obesity: comorbid conditions not required, but commonly present
Among pediatric patients who undergo metabolic or bariatric surgery, up to 15% and 8% experience minor and major perioperative risks, respectively.2 Up to one-quarter of patients require subsequent procedures within 5 years of original surgery. Vitamin deficiencies are common following weight loss surgery, requiring long-term monitoring and potential intervention.2 While surgery is not appropriate for all patients with severe obesity, evidence shows that those who do undergo these procedures experience good outcomes and improved quality of life.24
The Pharmacy Team’s Role in Pediatric Obesity
Every child deserves the opportunity to begin their life in good health. As trusted healthcare professionals, pharmacists and pharmacy technicians can make a transformative impact in the lives of young people with obesity. Managing weight-loss pharmacotherapy is an unmistakable role for pharmacy teams, but it can also impact many other aspects of care for this patient population.
Drug Utilization Review
Pharmacists conducting drug utilization review (DUR) for pediatric patients who are overweight or obese should recognize medications used for comorbid conditions that could be contributing to weight gain, including those mentioned above. They can also delegate much of the data collection and analysis portion of DUR to pharmacy technicians who possess good word processing and spreadsheet skills.
Pharmacists should also recognize the possibility of altered drug absorption in patients who take some weight-loss therapies or undergo surgical weight-loss procedures and consult trusted guidelines to determine if adjustments are needed (e.g., American Society for Metabolic and Bariatric Surgery). GLP-1 receptor agonists can delay gastric emptying, also referred to as gastroparesis. This means that food and drugs stay in the stomach longer, which can lead to slower absorption of orally administered drugs. Drugs differ in their sensitivity to delayed gastric emptying, so pharmacists should be cognizant of taking this into account for any other medications patients are taking.
Pharmacy technicians should be aware that orlistat is available over the counter (OTC) in a lower dose.25 They should refer patients buying orlistat OTC (brand name Alli) to a pharmacist to assess the product’s safety and appropriateness. The drug also alters the absorption of many other drugs, so careful DUR is needed for patients taking orlistat to prevent drug interactions and potential adverse effects. Pharmacy technicians can also remind all patients using orlistat, prescription, or OTC, of the importance of supplementing with a daily multivitamin to replace fat-soluble vitamins lost through the stool.12,25
Another consideration for pharmacists is the need for dose adjustments of other drugs for patients with obesity. Many drugs utilize weight-based dosing in pediatrics, but differing body composition compared to those of a healthy weight may affect drug pharmacokinetics (i.e., absorption, distribution, metabolism, and excretion) in youth with obesity.26 Lipophilic (fat-soluble) drugs may have a larger volume of distribution (Vd) in patients with excess fat, while hydrophilic (water-soluble) drugs may have increased Vd due to increased lean body mass, blood volume, and decreased total body water percentage. Fatty infiltrates of the liver may lead to decreased hepatic drug clearance, thereby affecting loading doses, dosage intervals, plasma half-lives, and times to reach steady-state concentration.26
The Pediatric Pharmacy Advocacy Group recommends the following for weight-based dosing in pediatrics:26
For patients who weigh less than 40 kg, use weight-based dosing.
For patients who weigh 40 kg or more, use weight-based dosing unless this exceeds the recommended adult dose for the specific indication.
Pharmacists can flag the profiles of patients whose doses should be monitored as they lose weight, and technicians can ask the patient or parent if the patient’s weight has changed significantly since they last visited the pharmacy. For patients approaching 40 kg from either direction, pharmacy technicians can also gently remind them that they need a current weight. Additionally, pharmacy technicians can make note of the availability of a good scale in the pharmacy to obtain a current weight when patients and parents are unsure.
Referrals for Specialized Care
Current practice patterns indicate a delay in intensive obesity treatment for months to years in the pediatric population, but the AAP guidelines recommend IHBLT as soon as possible.2 Pediatricians and family medicine providers can deliver patient-centered, non-stigmatizing nutrition and activity counseling for children of all weight classifications, but they should never employ watchful waiting or delay IHBLT for children who have already developed obesity. Ultimately, treatment delays reduce the likelihood of treatment success for pediatric patients with obesity, so sooner is better.2 Pharmacy teams should recognize pediatric patients with obesity who are not being treated by specialty clinics and refer patients to an expert.
Counseling and Education
Weight-related discussions can be sensitive but avoiding them may delay care and harm the patient-provider relationship. Evidence suggests that having conversations about obesity can facilitate more effective treatment.2
Motivational Interviewing
Motivational Interviewing (MI) is a patient-centered counseling approach that aims to identify and reinforce a patient's intrinsic motivation for change, as opposed to a traditional prescriptive approach.2 Motivational Interviewing guides families to select a behavior for change based on their own priorities and feasibility. It does not impose specific goals but celebrates successful changes in chosen behaviors, which can range from dietary improvements to physical activity or other relevant aspects. As patients enter adolescence, the emphasis in MI transitions from parental motivation alone to patient motivation with or without concurrent parental motivation.2
Motivational Interviewing involves four key processes:2
Engaging: In the initial stages of getting to know the patient, establish a collaborative role and an understanding of patient issues using open-ended questions, affirmations, nonjudgmental graphics, and empathy.
Focusing: Early and when the desire to change weight status is expressed, identify appropriate and productive strategies to employ for weight loss. Control gradually shifts from caregivers to patients, necessitating increased patient involvement in readiness assessments, particularly during adolescence.
Evoking: When behavior change is desired, empower patients and families by recognizing diverse motivations beyond health, such as athletic performance or self-image, through evaluating values, goals, and barriers to readiness.
Planning: When embarking on change, assess patient knowledge and available resources, offering support and guidance in choosing strategies. Also, clinicians should provide aid to patients in addressing setbacks and relapses, assisting patients in getting back on track with appropriate approaches given the challenges of obesity treatment.
Non-Stigmatizing Language
Perhaps the most important aspect of counseling patients and caregivers about obesity is respecting pediatric patients’ autonomy (i.e., independence and freedom to make choices) and safeguarding their emotional well-being. Pharmacists and pharmacy technicians should follow two general rules for respectfully addressing BMI and weight-related issues:2
Ask permission: Request consent to engage in a conversation regarding the patient's BMI and/or weight, respecting their autonomy and comfort level in discussing this topic.
Be respectful: Use non-stigmatizing language (i.e., avoiding negative judgment or bias) to maintain an open dialogue, including person- first language (i.e., prioritizes individual qualities before disabilities or conditions) and neutral terms. Table 2 lists examples of these concepts.
Table 2
Non-Stigmatizing Language in Pediatric Obesity Care2
| SAY THIS | NOT THAT |
| First-Person Language | |
Child with obesity My patient is affected by obesity | Obese child My patient is obese |
| Neutral Terms | |
Unhealthy weight Gaining too much weight for age | Obese Morbidly obese Large Fat Chubby |
Discussing BMI with children, adolescents, and families, even when using non-stigmatizing language and preferred terms, can still trigger strong emotional reactions like sadness or anger. Recognizing and validating these emotions while emphasizing the need to focus on the child’s health can strengthen healthcare relationships, build trust, and support ongoing care.
Pediatric Patient Autonomy
Although it is uncommon for children to accompany parents when the parent is picking up the child’s prescriptions, pharmacists should make use of chances to counsel school-aged kids directly. By the age of 5 to 7, most children can comprehend simple medication instructions, and their involvement in counseling is significant.27 This becomes especially crucial in scenarios where parents may not be available to advocate for them, such as at school.
When counseling pediatric patients, follow these rules:
use open-ended questions (i.e., without yes/no answers) to determine the child’s cognitive level
be aware of facial expressions, gestures, and tone of voice
avoid medical jargon, and use words with few syllables and short sentences with a mixture of text and illustration
recognize that a reasonable attention span is two to three minutes per year of age (i.e., a 7-year-old may be unable to focus longer than 15 minutes)28
Inventory Management
Pharmacy teams should ensure the availability of pediatric medication doses for weight-loss medications. Pharmacy technicians are often tasked with inventory management in the pharmacy and should be cognizant of keeping an adequate stock of these therapies. When patients initiate new therapies for weight loss, ensure the pharmacy maintains adequate stock to prevent
therapy interruptions, thus helping patients maintain adherence and persistence to weight-loss treatment.
Importantly, GLP-1 receptor agonists for obesity management have lengthy and complex titration schedules. When a patient initiates one of these therapies, ensure the pharmacy has the next dose in stock in advance of scheduled dose increases.
Summary
Pediatric obesity is an ongoing and worsening epidemic. Obesity is a multifaceted issue with many contributing and exacerbating factors. As obesity rates rise in the pediatric population, so do other medical conditions and chronic diseases that were more commonly seen in adulthood historically. They also suffer significant mental health consequences. Not surprisingly, pediatric obesity leads to obesity in adulthood.
Maintaining an open, respectful dialogue with patients and caregivers about pediatric obesity is a crucial skill. Pharmacists and pharmacy technicians with a deep understanding of the condition’s diagnosis and screening, physical and mental burden, and available treatment options can broach this difficult topic and make a significant difference in care and outcomes for this vulnerable patient population.
Course Test
Which of the following is TRUE about obesity’s prevalence in the pediatric population?
Prevalence increases with age, affecting more than 20% of those aged 12 to 19 years
The COVID-19 pandemic slowed the rate of BMI increase in children and adolescents
Obesity affects children and adolescents of all races and ethnicities equally
Children with obesity are more likely to come from high-income families with access to junk food
Which of the following BEST describes obesity diagnosis in children and adolescents?
Pediatric providers must use magnetic resonance imaging to confirm an obesity diagnosis
For patients aged 2 years and older, providers compare BMI relative to others of the same sex and age
Providers utilize BMI alone for patients aged 2 years and younger to diagnose obesity
Providers reserve the “severe obesity” classification for patients with BMI ≥ 85th percentile
Which of the following is TRUE regarding comorbidities in pediatric patients with obesity?
Children younger than 10 years old with obesity are at greatest risk of developing T2DM
Fatty liver disease is the most common comorbidity associated with pediatric obesity
Even if a child with obesity reaches a healthy weight, their comorbidities will not resolve
Many diseases previously found only in adults are now common in pediatric patients with obesity
Which of the following BEST describes the relationship between obesity and mental health?
Anxiety is the most consistently reported psychiatric comorbidity related to obesity
Male adolescents with obesity experience the greatest incidence of depression
Treating a patient’s depression with a selective serotonin reuptake inhibitor helps with weight loss
Pediatric patients with obesity are 32% more likely to have or develop depression
Which of the following is TRUE about eating disorders (EDs) in pediatric patients with obesity?
Discussing a patient’s obesity diagnosis with them will encourage the development of an ED
Self-guided dieting puts youth with obesity at high risk of weight fluctuation and disordered eating
Patients with obesity have double the lifetime rate of EDs compared to the general population
All pediatric patients with obesity are also considered to have a binge eating disorder
A 40-year-old female patient at a diabetes clinic struggles with obesity. She tells you that her 15-year-old son is starting to gain weight, and the pediatrician says he is in the 86th percentile. She wants to start encouraging him to eat healthier and maintain a healthy weight. Which of the following is the BEST suggestion?
Suggest that she consult with the IHBLT clinic for early obesity intervention
Offer a wide range of food options and model good behavior during family meal times
Completely stop buying “junk food” and do not allow him to eat it
Use “junk food” only as a reward for good grades or other desired behaviors
Lily, a 14-year-old female, presents to the pediatrician with nervousness and, upon questioning, reveals bullying in school that is affecting her academic performance. Her BMI is 38 kg/m2, and she says that her weight is the focus of the bullying. Lily’s mom is single and has 2 jobs, so they stop for fast food several times a week on the way home from school. Lily’s screen time is from 7 pm to 11 pm daily while her mom works a second shift. Lily tried 3 months of self-guided dieting and lifestyle and exercise changes, only losing 2 pounds. Which of the following strategies is BEST to engage Lily in managing her obesity?
Speak only to Lily’s parents, not Lily directly, to avoid stigmatizing or offending her
Show Lily a movie about the danger of obesity since she enjoys screen time
Ask Lily for permission to talk directly to her about her weight- related issues
Use milder language like “chubby” or “large” rather than “fat” or “morbidly obese”
Continuing with Lily from question 7, Lily’s pediatrician referred her to an IHBLT clinic. The clinic decided that pharmacotherapy would be helpful to aid in Lily’s weight loss efforts. Which is the BEST option for first-line pharmacotherapy?
Orlistat with counseling about the potential for fatty, foul-smelling stools
Phentermine with counseling about the risks of dependence and abuse
Metformin with counseling about the potential for developing PCOS
Lisdexamfetamine with counseling that the drug should also help with academic focus
Continuing with Lily from question 7, which of the following is important to consider in managing Lily’s obesity?
Any pharmacotherapy used is off-label and not well-studied in adolescence
Lily’s weight and body composition may affect how her body absorbs and metabolizes drugs
She must limit screen time to 1 hour daily, along with IHBLT and pharmacotherapy
She should try to skip breakfast whenever possible to accelerate weight loss
Paul is a 4-year-old male in the 98th BMI percentile. His mom and dad have demanding jobs, so they eat fast food about 3 times weekly. Paul’s favorite order is chicken nuggets with French fries and orange soda, and he watches TV or plays on his tablet for about 4 hours daily. At his most recent physical, Paul’s bloodwork showed that he is prediabetic. Which of the following is the BEST option to suggest to Paul’s parents?
Swap out some of Paul’s tablet time for 30 minutes daily of exergames
Encourage Paul to drink apple juice instead of orange soda
Seek assistance from an IHBLT clinic for weight loss as soon as possible
Make an appointment with a bariatric surgeon for a consultation
References
Centers for Disease Control and Prevention. Childhood overweight and obesity. CDC. Updated April 1, 2022. https://www.cdc.gov/obesity/childhood/index.html. Accessed October 19, 2023.
Hampl SE, Hassink SG, Skinner AC, et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics. 2023;151(2):e2022060640. doi:10.1542/peds.2022-060640
Okobi OE, Izundu IC, Evbayekha EO, et al. Obesity in the Pediatric Population of the National (Nationwide) Inpatient Sample (NIS), USA. Cureus. 2022;14(12):e33111. Published 2022 Dec 29. doi:10.7759/cureus.33111
Centers for Disease Control and Prevention. Defining child BMI categories. CDC. Updated March 21, 2023. https://www.cdc.gov/obesity/basics/childhood-defining.html. Accessed October 19, 2023.
Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. CDC. September 14, 2023. https://www.cdc.gov/healthyweight/bmi/calculator.html. Accessed October 19, 2023.
Sahoo K, Sahoo B, Choudhury AK, Sofi NY, Kumar R, Bhadoria AS. Childhood obesity: causes and consequences. J Family Med Prim Care. 2015;4(2):187-192. doi:10.4103/2249-4863.154628
Cuda SE, Censani M. Pediatric Obesity Algorithm: A Practical Approach to Obesity Diagnosis and Management. Front Pediatr. 2019;6:431. Published 2019 Jan 23. doi:10.3389/fped.2018.00431
Centers for Disease Control and Prevention. Consequences of obesity. CDC. Updated July 15, 2022. https://www.cdc.gov/obesity/basics/consequences.html. Accessed October 21, 2023.
Small L, Aplasca A. Child Obesity and Mental Health: A Complex Interaction. Child Adolesc Psychiatr Clin N Am. 2016;25(2):269-282. doi:10.1016/j.chc.2015.11.008
Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289(14):1813- 1819. doi:10.1001/jama.289.14.1813
Budd GM, Hayman LL. Addressing the childhood obesity crisis: a call to action. MCN Am J Matern Child Nurs. 2008;33(2):111-120. doi:10.1097/01.NMC.0000313419.51495.ce
Singhal V, Sella AC, Malhotra S. Pharmacotherapy in pediatric obesity: current evidence and landscape. Curr Opin Endocrinol Diabetes Obes. 2021;28(1):55-63. doi:10.1097/MED.0000000000000587
Xenical. Prescribing information. Genentech USA, Inc.; 2022.
Ard J, Fitch A, Fruh S, Herman L. Weight Loss and Maintenance Related to the Mechanism of Action of Glucagon-Like Peptide 1 Receptor Agonists. Adv Ther. 2021;38(6):2821-2839. doi:10.1007/s12325-021- 01710-0
Kelly AS, Auerbach P, Barrientos-Perez M, et al. A Randomized, Controlled Trial of Liraglutide for Adolescents with Obesity. N Engl J Med. 2020;382(22):2117-2128. doi:10.1056/NEJMoa1916038
Saxenda. Prescribing information. Novo Nordisk, Inc.; 2023.
details.html?id=151389. Accessed October 24, 2023.
Wegovy. Prescribing information. Novo Nordisk, Inc.; 2023.
Rybelsus. Prescribing information. Novo Nordisk, Inc.; 2020.
Kelly AS, Bensignor MO, Hsia DS, et al. Phentermine/Topiramate for the Treatment of Adolescent Obesity. NEJM Evid. 2022;1(6):10.1056/evidoa2200014. doi:10.1056/evidoa2200014
Wilson DM, Abrams SH, Aye T, et al. Metformin extended release treatment of adolescent obesity: a 48-week randomized, double-blind, placebo-controlled trial with 48-week follow-up. Arch Pediatr Adolesc Med. 2010;164(2):116-123. doi:10.1001/archpediatrics.2009.264
Tamborlane WV, Bishai R, Geller D, et al. Once-Weekly Exenatide in Youth With Type 2 Diabetes. Diabetes Care. 2022;45(8):1833-1840. doi:10.2337/dc21-2275
Imcivree. Prescribing information. Rhythm Pharmaceuticals; 2022.
Johnson VR, Northam KA, Smith JJ, Newsome FA, Gomez G, Stanford FC. Hearing Their Voices: Exploring the Patient Narratives of Adolescent and Young Adults Who Have Undergone Metabolic and Bariatric
Surgery-A Case Series. Med Res Arch.
2021;9(5):10.18103/mra.v9i5.2419. doi:10.18103/mra.v9i5.2419
Alli. Prescribing information. GlaxoSmithKline; 2017.
Matson KL, Horton ER, Capino AC; Advocacy Committee for the Pediatric Pharmacy Advocacy Group. Medication Dosage in Overweight and Obese Children. J Pediatr Pharmacol Ther. 2017;22(1):81-83. doi:10.5863/1551-6776-22.1.81
Carpenter DM, Abraham O, Alexander DS, Horowitz K. Counseling of children and adolescents in community pharmacies: Results from a 14- day observational study. J Am Pharm Assoc (2003). 2016;56(3):266- 269.e1. doi:10.1016/j.japh.2016.03.001
Brain Balance. Normal attention span expectations by age. https://www.brainbalancecenters.com/blog/normal-attention-span- expectations-by-age. Accessed October 24, 2023.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.