PARKINSON’S DISEASE: A COLLABORATIVE APPROACH TO ADDRESSING NON-MOTOR SYMPTOMS
Faculty:
Kimberly Valenta, MD
Kimberly Valenta is a freelance medical writer and editor. She studied chemistry at Mount Holyoke College and medicine at Northwestern University. After completing her anesthesiology residency, she joined the faculty at Stanford University, where she cared for patients and taught medical students and residents. In 2020, she transitioned to writing and editing full-time. She holds a certificate in medical writing and editing from the University of Chicago and is an active member of the American Medical Writers Association.
Becca Resnik, RN
Becca Resnik received her nursing degree from Chattanooga State Community College. She has an MA in Translation Studies from the University of Birmingham, United Kingdom, and a BS in Nuclear Engineering Technology from Excelsior University, Albany, New York. Becca Resnik also has a Medical Writing Certificate from the University of Connecticut School of Pharmacy. Becca Resnik maintains an active Registered Nurse license.
Pamela Sardo, PharmD, BS
Pamela Sardo is a freelance medical writer, pharmacist licensed in 3 states, and the founder/principal at Sardo Solutions. She received her BS from the University of Connecticut and a PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, pharmaceutical manufacturing, and managed healthcare across broad therapeutic classes and disease states.
Topic Overview:
Parkinson’s disease (PD) is often identified by its motor symptoms; however, they represent only part of the disease burden. Non-motor symptoms (NMS) are now recognized as central features of PD. These symptoms may occur before motor signs appear, develop alongside them, or progress independently. Non-motor symptoms affect nearly every aspect of daily life, including mood, sleep, memory and thinking, autonomic regulation, pain, and sensory perception. This course focuses on NMS and highlights opportunities for pharmacists to support patients and contribute to interdisciplinary care.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-25-062-H01-P
Pharmacy Technician 0669-0000-25-063-H01-T
Credits: 3 contact hour(s) (0.3 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $8.99
Estimated time to complete activity: 3 contact hour(s) (0.3 CEU(s)), including Course Test and course evaluation
Release Date: May 19, 2025 Expiration Date: May 19, 2028
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
Secondary Audiences: Other healthcare professionals, such as nurses, physicians, or others who may be part of a healthcare team, may be interested in this educational topic. Healthcare team roles and approaches to patient care are discussed in this activity. No state board, professional organization, or credentialing body has evaluated this activity to determine whether it meets the continuing education requirements of nurses, physicians, or other professions not listed under the “Target Audience” section above. Always verify with individual employers or supervisors whether they will accept this educational activity upon completion.
How to Earn Credit: From May 19, 2025, through May 19, 2028, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Recognize non-motor symptoms associated with Parkinson’s disease, including those that emerge during the prodromal phase
Distinguish pharmacologic strategies used to manage non-motor symptoms
Describe nonpharmacologic interventions that improve non-motor symptoms and promote quality of life
Identify interdisciplinary opportunities to support recognition, patient education, and referrals
Disclosures
The following individuals were involved in developing this activity: Kimberly Valenta, MD, Becca Resnik, RN, and Pamela Sardo, PharmD, BS. Kimberly Valenta, Becca Resnik, and Pamela Sardo have no conflicts of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2025: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Parkinson's Disease: A Collaborative Approach to Addressing Non-Motor Symptoms
Introduction
Parkinson’s disease (PD) is often identified by its motor symptoms. These include bradykinesia, which refers to slowness of movement; resting tremor, which is a rhythmic shaking that occurs when the muscle is relaxed; rigidity, or muscle stiffness; and postural instability, which affects balance and increases fall risk. While these features form the basis for clinical diagnosis, they represent only part of the disease burden. This course focuses on non-motor symptoms (NMS) and highlights opportunities for healthcare teams to support patients and contribute to interdisciplinary care.
Emergence of Non-motor Symptoms
Non-motor symptoms are now recognized as central features of PD. These symptoms may occur before motor signs appear, develop alongside them, or progress independently. Non-motor symptoms affect nearly every aspect of daily life, including mood, sleep, memory and thinking, autonomic regulation, pain, and sensory perception.1
Historically, these symptoms were considered secondary or late-stage complications. However, evidence now shows that NMS often emerges years before a PD diagnosis is made.2 For example, constipation, sleep changes, or depression may precede motor symptoms by a decade or more.
The burden of NMS is considerable. These symptoms are linked to lower quality of life, increased caregiver stress, higher rates of hospitalization and institutionalization, and worse overall health outcomes.3 In many cases, symptoms such as fatigue, pain, or anxiety may have a greater impact on daily life than tremor or stiffness.
Despite their impact, NMS often go unrecognized. This may occur because patients do not report them, or because clinicians attribute them to aging, medication side effects, or other chronic conditions.4 Lack of awareness about the significance of these symptoms in PD remains a barrier to care.
Family physicians can play an important role in identifying and treating nonmotor symptoms of PD, such as neuropsychiatric symptoms, such as depression and sleep disorders, and they can help recognize and treat psychosis and dementia. They can manage common autonomic symptoms such as orthostatic hypotension and constipation. Nurses often perform the initial assessment when a patient arrives at a healthcare facility. Through comprehensive assessment and interview skills, nurses can serve as an early line of defense in discovering NMS in a patient.
Pharmacists are well-positioned to help close this gap. During medication reviews, counseling sessions, or routine check-ins, pharmacists can recognize patterns that suggest NMS involvement. They can recommend pharmacologic and non-pharmacologic strategies, identify potential medication-related contributors, and communicate findings with the rest of the care team.5 Referrals to physiotherapy, occupational therapy, speech language therapy, and exercise groups are recommended to help preserve function.6
Epidemiology of Non-Motor Symptoms
Non-motor symptoms are nearly universal in PD. In one large multicenter study, 99.7% of people with PD reported at least one non-motor symptom, with a mean of almost eight symptoms per person.7 These symptoms are present across all stages and tend to increase in number and severity as the disease progresses. They affect nearly every major body system and functional area, including mood, sleep, gastrointestinal, cardiovascular, urinary, and cognitive function. Pain, fatigue, and sensory changes are also common and frequently underrecognized. This wide- ranging symptom burden highlights the importance of routine assessment and interdisciplinary management throughout the course of the disease.
Clinical Presentation
Parkinson’s disease is typically recognized by its motor symptoms, including bradykinesia (slowness of movement), resting tremor, rigidity, and postural instability. These signs are linked to the loss of dopaminergic neurons in the substantia nigra.6 However, NMS is also a core feature of the disease and may be even more disabling, particularly in later stages.1,3
Non-motor symptoms can appear at any point during the disease course. Some develop years before diagnosis and may offer early diagnostic clues during the prodromal phase. These include symptoms like constipation, REM sleep behavior disorder, vague shoulder pain, anxiety, depression, and hyposmia (reduced sense of smell).2,4,8 Others emerge later, either as the disease progresses or during treatment.
Once present, NMS may follow different patterns. Some fluctuate in response to medication timing, worsening during “off” periods when dopaminergic effects wear off. Others remain constant throughout the day and may not respond to dopaminergic therapy at all. In some cases, medications used to manage motor symptoms can worsen non-motor symptoms. For example, dopamine agonists are associated with hallucinations and impulse control disorders.9
Early symptoms such as constipation, REM sleep behavior disorder, anxiety, depression, and hyposmia may offer important diagnostic clues, particularly during risk assessment in the prodromal phase.2,4,8 As PD advances, the burden of NMS often increases and can surpass that of motor symptoms. These complications contribute to reduced independence, caregiver strain, and increased need for coordinated, multidisciplinary care.3
Categories of Non-Motor Symptoms in Parkinson’s Disease
Non-motor symptoms in PD span multiple functional domains and vary widely in onset, severity, and impact. Some symptoms emerge early, even before motor signs appear, while others develop later in the disease course. The International Parkinson and Movement Disorder Society-Non-Motor Symptoms Scale, or MDS- NMS, categorizes these symptoms across multiple domains to support systematic assessment and management.10 The following sections provide an overview of each major symptom domain, along with estimated prevalence and clinical relevance.
Autonomic Symptoms
Autonomic dysfunction is common in PD and can affect multiple organ systems, including gastrointestinal, cardiovascular, urinary, sexual, and thermoregulatory functions. These symptoms often appear early and may worsen as the disease progresses. Although frequently underrecognized, autonomic symptoms can significantly affect quality of life and may complicate medication management.7,11
Gastrointestinal symptoms are among the most frequent. Constipation often begins in the prodromal phase and may precede diagnosis by several years. Gastroparesis, or delayed gastric emptying, occurs in the majority of patients and can impair levodopa absorption, contributing to fluctuations in motor response. Sialorrhea (drooling) is another common symptom. It results from impaired swallowing rather than excessive saliva production and may lead to social discomfort, skin irritation, or aspiration.11
Cardiovascular symptoms, such as orthostatic hypotension, are also prevalent. Orthostatic hypotension is defined as a sustained drop in systolic blood pressure of at least 20 mmHg or diastolic pressure of at least 10 mmHg within three minutes of standing. It affects approximately 30% to 40% of people with Parkinson’s disease. Symptoms include dizziness, fatigue, and cognitive slowing. In some cases, orthostatic hypotension leads to fainting and increases the risk of falls.7,11 Nurses should institute fall precautions for all patients with PD and should instruct these patients to change positions slowly.12
Urinary symptoms result primarily from detrusor overactivity, including urgency, frequency, nocturia, and urge incontinence. Some patients also report incomplete bladder emptying. These symptoms can be socially limiting, contribute to poor sleep, and are often cited among the most bothersome by patients.7
Many individuals with Parkinson’s disease also report sexual dysfunction. This may involve reduced libido, difficulty with arousal, erectile dysfunction, or vaginal dryness. Thermoregulatory problems, including excessive sweating, heat intolerance, dry eyes, or excessive tearing, are also part of the autonomic profile.11
Table 1
Prevalence of Autonomic Dysfunction in Parkinson’s Disease7,11
| Symptom | Estimated Frequency |
| Gastrointestinal dysfunction | 72% |
| Constipation | 33–48% |
| Sialorrhea (drooling) | 32–74% |
| Weight loss | 50% |
| Gastroparesis (slow gastric emptying) | 70–100% |
| Cardiovascular dysfunction | - |
| Orthostatic hypotension | 30–40% |
| Postprandial hypotension | 30% |
| Supine hypertension | 34% |
| Urinary dysfunction | 74% |
| Nocturia | 42% |
| Urinary frequency | 42% |
| Urinary urgency | 57% |
| Incomplete bladder emptying | 25% |
| Sexual dysfunction | 40% |
| Reduced sexual drive | 31% |
| Reduced arousal | 29% |
Psychiatric Symptoms
Psychiatric symptoms are common in Parkinson’s disease and may occur at any stage of the illness. These symptoms can affect mood, behavior, perception, and motivation, and often substantially impact quality of life. They may contribute to social withdrawal, caregiver distress, and increased risk of institutionalization.3
Depression and anxiety are among the most frequently reported psychiatric symptoms. Each affects approximately 30% to 35% of individuals with Parkinson’s disease. Depression may be underdiagnosed, as symptoms can overlap with motor slowing or apathy. Anxiety often presents as generalized worry but may also take the form of panic attacks, social phobia, or agoraphobia. Both conditions are treatable but often overlooked in routine clinical care.3
Psychosis tends to occur later in the disease course and is often associated with cognitive impairment or the use of dopaminergic medications. Minor psychosis may begin with subtle illusions or the feeling of a presence in the room. Over time, patients may develop visual hallucinations, non-visual hallucinations, or fixed delusions. Visual hallucinations are reported in up to 30% of patients, while non- visual hallucinations occur in up to 35%. Delusions are less common but can be particularly disruptive and distressing for families.3
Apathy is also a frequent and often misunderstood symptom. It refers to a loss of motivation that is not accompanied by sadness. Apathy affects approximately 35% to 40% of patients and can interfere with daily functioning and social engagement. It may be mistaken for depression, but the two are distinct and may require different management strategies.3
Impulse control disorders are another important psychiatric concern in Parkinson’s disease. These behaviors include compulsive gambling, shopping, eating, or sexual activity. They occur in about 15% of individuals treated with dopamine agonists and can lead to serious social and financial consequences if not identified early.3
Table 2
Prevalence of Psychiatric Symptoms in Parkinson’s Disease3
| Symptom | Estimated Frequency |
| Depression | 30–35%, up to 60% in advanced disease |
| Anxiety | 30–35% |
| Psychosis | Up to 60% cumulative prevalence |
| Minor psychosis | 25–40% |
| Visual hallucinations | 15–30% |
| Non-visual hallucinations | Up to 35% |
| Delusions | 4% |
| Apathy | 35–40% |
| Impulse control disorders | 15% |
Cognitive Symptoms
Cognitive impairment is a common and progressive feature of PD. Associated changes may affect memory, attention, language, executive function, or visuospatial abilities. Cognitive symptoms can appear early in the disease course, even before motor signs are diagnosed, and tend to worsen over time.13
At the time of diagnosis, an estimated 10% to 20% of individuals with PD already have measurable cognitive deficits. About 25% meet criteria for mild cognitive impairment, which is defined as a decline in cognitive function that does not yet interfere with daily activities. The presence of mild cognitive impairment is associated with a higher risk of developing dementia in subsequent years.13
Dementia is a later-stage complication that involves a global decline in cognitive abilities affecting independent function. It contributes significantly to disability, caregiver burden, and long-term care needs. In a recent longitudinal study, the probability of developing dementia increased steadily with disease duration: 9%
to 27% at 10 years, approximately 50% at 15 years, and 74% at 20 years. The median time to dementia from diagnosis was 15 years.13
Several risk factors are associated with faster cognitive decline. These include older age at PD onset, male sex, and lower levels of education. Identifying early cognitive symptoms is important for care planning, medication review, and safety considerations.13
Table 3
Estimated Probability of Dementia by Disease Duration in Parkinson’s Disease13
| Cognitive Outcome | Frequency Estimate |
| Mild cognitive impairment | ~25% at diagnosis |
| Dementia by 5 years | 3–12% |
| Dementia by 10 years | 9–27% |
| Dementia by 15 years | ~50% |
| Dementia by 20 years | ~74% |
| Dementia by ≥25 years | ~90% |
Sleep Disturbances
Sleep disturbances are common in PD and can begin early, often before a formal diagnosis is made. These problems may arise from disease-related changes in brain regions that regulate sleep and arousal, motor symptoms, medications, or coexisting psychiatric conditions. Sleep disturbances can significantly impair quality of life and contribute to daytime fatigue, mood changes, and poor motor symptom control.14
Insomnia is the most frequently reported sleep disorder in PD. It typically involves difficulty staying asleep, often due to nighttime motor symptoms, anxiety, or fragmented sleep architecture. REM sleep behavior disorder (RBD) is also common. It is a parasomnia in which individuals physically act out vivid dreams, sometimes resulting in injury to themselves or a bed partner. RBD may precede motor symptoms by several years and is recognized as an early clinical feature of PD.14
Excessive daytime sleepiness affects approximately 25% of people with PD. It is characterized by persistent drowsiness or sudden episodes of falling asleep during the day. Excessive daytime sleepiness may result from poor nighttime sleep or dopaminergic medications, particularly dopamine agonists. Restless legs syndrome is another contributor to sleep disruption. It involves an urge to move the legs, usually at night, and is often accompanied by uncomfortable sensations. Dopaminergic fluctuations or low iron levels may worsen restless legs syndrome.14
Sleep-disordered breathing, including obstructive sleep apnea, does not appear to be more common in PD than in the general population. However, when present, it can further disrupt sleep and contribute to fatigue, poor concentration, and increased cardiovascular risk.14
Table 4
Prevalence of Sleep Disturbances in Parkinson’s Disease14
| Sleep Disorder | Estimated Frequency |
| Insomnia | 41% |
| REM sleep disorder | 25% |
| Excessive daytime sleepiness | 25% |
| Restless legs syndrome | 16% |
| Sleep-disordered breathing | 12% |
Sensory and Other Symptoms
In addition to cognitive, psychiatric, autonomic, and sleep-related changes, people with PD commonly experience symptoms that affect sensory perception, energy levels, and weight.
Pain is one of the most frequently reported NMS in PD. Prevalence estimates vary widely, ranging from 24% to over 85%, depending on disease stage, assessment methods, and population studied.15 Pain may begin early in the disease, sometimes before motor symptoms appear, and becomes more common as the disease progresses. Musculoskeletal pain is the most frequently reported subtype and may result from rigidity, postural changes, or joint abnormalities. Other types of pain include dystonic pain, radicular or neuropathic pain, central pain, and orofacial pain. Pain is often linked to motor complications, depression, and poor sleep, and may fluctuate in intensity depending on medication timing or disease stage.15
Fatigue is also common, affecting approximately half of patients. It may be physical, mental, or both, and can occur even without exertion. Fatigue often overlaps with depression, sleep problems, or medication side effects. It may be difficult to treat and is one of the most disabling symptoms for many patients.7
Hyposmia is another early symptom. It is reported in up to 75% of individuals with Parkinson’s disease and may appear years before motor signs develop. Although it may seem minor, hyposmia can interfere with appetite, enjoyment of food, and safety awareness, such as detecting smoke or rotten food.7
Weight loss is also observed in many individuals with PD, particularly in later stages. Contributing factors may include reduced appetite, swallowing difficulties, gastrointestinal dysmotility, increased energy expenditure from tremor or dyskinesia, and depression. Weight loss may impact medication response and overall frailty.11 Nurses should counsel patients with PD and their caregivers to record weekly weights, which can reveal the need for alterations to the diet or prescriptions.12
These symptoms are often overlooked during routine clinical visits, but can significantly impact a patient's comfort and function. Pharmacists can help identify medication-related contributors, support non-drug interventions, and refer patients for further evaluation when appropriate. In addition to being underreported, many of these symptoms vary in intensity throughout the day, making them harder to detect.
Fluctuations in Motor and Non-Motor Symptoms
Like motor symptoms, NMS may fluctuate in response to medication timing or disease progression. These subtle changes may go unrecognized unless patients are asked about specific patterns.
Motor fluctuations refer to alternating periods of better and worse motor function in response to dopaminergic therapy. These fluctuations often develop after several years of treatment and reflect changes in medication absorption, receptor sensitivity, or disease progression. Motor function is typically better during “on” periods and worse during “off” periods.3
Non-motor fluctuations are similar changes that affect symptoms such as anxiety, cognitive function, fatigue, pain, or autonomic features like urinary urgency. These symptoms may worsen during “off” periods and improve during “on” periods. For example, a patient might feel more anxious or have difficulty concentrating when their motor symptoms reappear.
However, not all NMS follow this pattern. Some symptoms, such as apathy, confusion, or orthostatic intolerance, may fluctuate independently of motor function and do not always respond to dopaminergic medications.9
The relationship between motor and non-motor fluctuations is not fully understood. Some symptoms improve when medications are active, while others may be unaffected or even worsened. This variability is more common in advanced stages of the disease.9,16
Non-motor fluctuations are common but often overlooked. Because they change throughout the day, they can be hard to detect unless patients are asked about specific patterns. Tracking tools like symptom diaries or mobile apps can help identify these fluctuations and guide individualized treatment adjustments.9
Improving Recognition in Practice
Non-motor symptoms are often underreported. Patients may not recognize that symptoms like fatigue, constipation, or apathy are related to PD. They may also assume that nothing can be done or feel reluctant to discuss symptoms like
depression, hallucinations, or urinary urgency. Clinicians can improve recognition by using validated tools during routine assessments.5
Available tools include:
The MDS Non-Motor Rating Scale (MDS-NMS)
The Non-Motor Symptoms Questionnaire (NMSQ)
The Non-Motor Fluctuation Assessment (NoMoFA) Questionnaire
These tools support more consistent evaluation and documentation of symptoms that can otherwise be overlooked.
Pathophysiology of Non-Motor Symptoms
The pathophysiology of PD is not completely understood, but it is complex and involves multiple systems. Genetics and the environment are also considered contributors. There are several hypotheses to describe the pathophysiology. One ‘gut-brain-axis’ hypothesis suggests that PD originates in the gut, with pathologic processes spreading from cell-to-cell transmission.17
The transmission proceeds through the sympathetic and parasympathetic nervous systems to the substantia nigra and central nervous system (CNS). This hypothesis proposes that misfolded α-synuclein, a key protein in PD, is transported from the enteric nervous system to the brain, contributing to motor and nonmotor symptoms.17
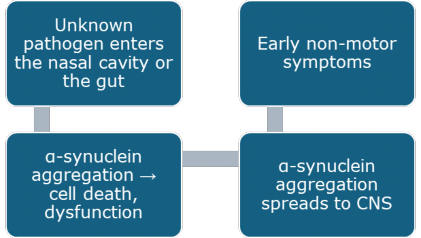
Braak’s hypothesis states that PD begins when unknown pathogens or microbial products enter the body through the nasal cavity or gut.18 These pathogens or products may trigger α-synuclein aggregation in the olfactory bulb or enteric nervous system.18 The aggregation of α-synuclein leads to cell death and dysfunction.
The pathology in the nervous system then spreads from the vagus nerve to the brainstem and higher brain regions, including the substantia nigra. This progression is associated with the early appearance of nonmotor symptoms such as olfactory impairment (hyposmia) and constipation, which often precede motor symptoms.18 Olfactory dysfunction is associated with α-synuclein
accumulation in the olfactory bulb, while constipation arises from impaired gastrointestinal motility due to enteric nervous system involvement.18 Critics of this hypothesis suggest that genetic and environmental factors also contribute to the progression of PD.
Researchers believe neuroinflammation increases the effects.19 Changes in the immune system that occur with aging may exacerbate PD by promoting chronic inflammation.19 When misfolded α-synuclein interacts with cells, pro- inflammatory cytokines are released.19 The neuroinflammation processes can accelerate neurodegeneration and disrupt neural networks, contributing to nonmotor symptoms like cognitive decline, sleep disturbances, and autonomic dysfunction.
Early manifestations like hyposmia and constipation reflect peripheral pathology, while inflammation and neuronal damage are associated with systemic nonmotor symptoms. Figure 1 depicts the hypothesis for environmental triggers of non-motor symptoms.
Figure 1
Hypothesis for Environmental Triggering of PD Non-motor Symptoms18
Diagnosis of PD: The Role of Non-Motor Symptoms
Parkinson’s disease is defined by the International Parkinson and Movement Disorder Society (MDS) as a clinical motor syndrome accompanied by neurodegeneration in the substantia nigra and pathological accumulation of alpha- synuclein.20 In clinical practice, diagnosis is based on established criteria and expert evaluation. At present, no biomarker can definitively confirm the diagnosis in a living patient.
The MDS Clinical Diagnostic Criteria follow a two-step approach. The first step is to confirm the presence of parkinsonism. This is defined as bradykinesia with asymmetrical onset, along with either rest tremor or rigidity. The second step is to assess the likelihood of PD as the cause of parkinsonism by weighing supportive features, diagnostic red flags, and absolute exclusion criteria. Based on this assessment, individuals may be classified as having clinically established or clinically probable PD.2
Non-Motor Symptoms as Diagnostic Features
Non-motor symptoms are increasingly recognized as helpful diagnostic clues, especially in the early stages of disease. Several symptoms may appear years before the onset of motor signs. These include constipation, reduced sense of smell, REM sleep behavior disorder, depression, and vague musculoskeletal discomfort, often in the shoulder or neck.4
Two NMS are included among the MDS supportive diagnostic criteria:2
Hyposmia, which can be confirmed with olfactory testing
REM sleep behavior disorder, which may be identified through clinical history or sleep studies
On the other hand, the absence of any NMS within five years of motor onset is considered a red flag. This finding decreases confidence in the diagnosis of PD.2
Non-motor symptoms can also help distinguish PD from atypical parkinsonian syndromes. For example, multiple system atrophy and progressive supranuclear palsy often present with early autonomic dysfunction, vertical gaze abnormalities, or
symmetrical motor symptoms. These features are not typical of PD and may suggest an alternative diagnosis.21
Table 5
Summary of MDS Clinical Diagnostic Criteria2
| Step | Criteria | Details |
| Step 1 | Confirm parkinsonism | Requires bradykinesia plus either rest tremor or rigidity. Onset should be asymmetric. |
| Step 2 | Assess for PD vs other causes of parkinsonism | Use supportive criteria, red flags, and absolute exclusion criteria. |
| Supportive Criteria (increases diagnostic certainty of PD) | Clear and sustained levodopa response Development of levodopa- induced dyskinesia Rest tremor of a limb Hyposmia REM sleep behavior disorder | Presence of ≥2 supports a diagnosis of clinically established PD. |
| Reg Flags (weakens confidence in PD diagnosis) | Early postural instability Rapid progression or early wheelchair use Severe early autonomic dysfunction No NMS after 5 years Bilateral symmetric onset | Can be offset by multiple supportive criteria. |
| Absolute Exclusion Criteria (rule out PD) | Cerebellar signs (e.g., ataxia) Vertical gaze palsy Early severe dementia Cortical sensory loss, apraxia, or aphasia Parkinsonism due to medications or vascular causes | Presence excludes PD diagnosis. |
Diagnostic Challenges
Parkinson’s disease is often misdiagnosed or diagnosed late. On average, there is a delay of nearly ten years between the onset of symptoms and the establishment of a formal diagnosis.4 Early NMS are often misattributed to aging, mood disorders, or gastrointestinal conditions.
Because NMS often appear first and may not be disclosed unless directly asked about, they are frequently overlooked. A careful review of early symptoms such as constipation, insomnia, fatigue, or changes in mood can improve diagnostic accuracy, particularly when these symptoms are viewed in context with motor findings and risk factors.5
Pharmacologic Management of Non-Motor Symptoms
Managing the non-motor symptoms of PD presents a challenge to physicians because identifying the symptoms, differentiating possible contributions from medication, and uncovering the patient’s emotional state are required.22
Treatment goals vary from person to person, emphasizing the need for personalized approaches. There is no reason to postpone symptomatic treatment.4 In some cases, pharmacologic therapy is first-line; however, in other cases, lifestyle or nonpharmacologic approaches are first-line. It is also important to consider nonmotor symptoms, polypharmacy, comorbidities, and caregiver burden, which can increase hospitalization risk.6
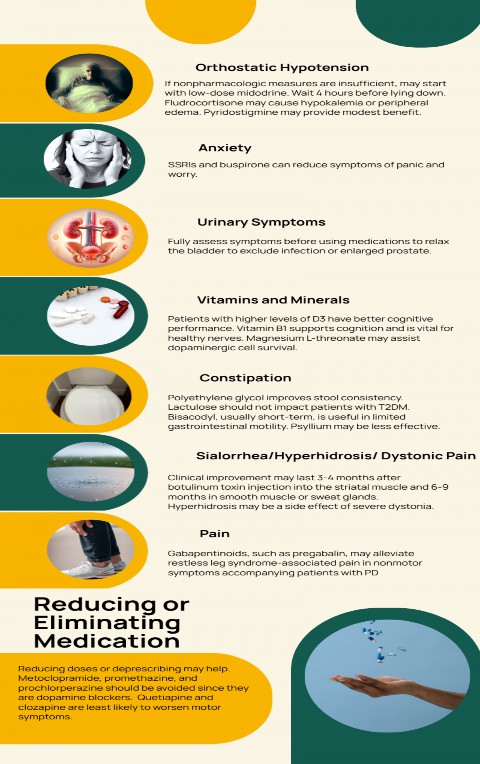
Table 6 provides treatment options for a broad range of NMS. Figure 2 provides information to supplement Table 6.
Table 6
Pharmacologic and Non-pharmacologic Management of Non-motor Symptoms in Parkinson’s Disease22-26
| NMS Symptom | Non-Pharmacologic Therapies | Pharmacologic Therapies |
| Neuropsychiatric Symptoms | ||
| Depression/Anxiety | CBT, exercise, social support, mindfulness- based stress reduction, mindfulness-based cognitive therapy, Qigong, dance, and music therapy | SSRI: citalopram, escitalopram, paroxetine, fluoxetine, or sertraline SNRIs: venlafaxine TCA: desipramine, nortriptyline Benzodiazepines: clonazepam (panic disorder) |
| Apathy | CBT, music therapy | AChEI: rivastigmine Piribedil, a D2/D3 dopamine agonist |
Psychosis - Hallucinations/Delusions | Environmental modifications, caregiver support, and reduce nighttime stimulation | Pimavanserin, a serotonin 5-HT 2A/C inverse agonist and antagonist Atypical antipsychotics: clozapine, quetiapine AChEI: rivastigmine, donepezil NMDA antagonist: memantine |
| Impulse Control and Related Disorders | Psychoeducation, CBT, caregiver support | Reduce dopamine agonists Amantadine (conflicting evidence) |
| Cognition Impairment/Dementia | Cognitive training, mental stimulation, sleep optimization, dance, and music therapy | AChEI: rivastigmine, donepezil (off-label) NMDA antagonist: memantine (off-label) |
| Autonomic Symptoms | ||
| Orthostatic Hypotension | Dietary modifications (increased salt), hydration, compression | Mineralocorticoid: fludrocortisone α-1 adrenergic agonist |
| garments, physical exercise, and elevate the head of bed | and vasopressor: midodrine AChEI: pyridostigmine NE precursor: droxidopa NRI: ampreloxetine Review antihypertensives, diuretics, and PD medication | |
| Lower Urinary Tract Symptoms | Scheduled voiding, pelvic floor exercises | Antimuscarinic: oxybutynin, trospium Beta-3 agonist: mirabegron Botulinum toxin |
| Sexual Problems | Schedule sexual activity when medications are working best | PDE5 inhibitor for ED: sildenafil Female decreased libido and dryness: HRT, estrogen cream, lubrication |
| Constipation | Hydration, fiber, small meals, regular exercise | Fiber supplements: psyllium Laxatives: polyethylene glycol, bisacodyl Probiotics Secretagogue: lubiprostone 5-HT4 agonist: prucalopride |
| Sialorrhea (Drooling) | Posture, chewing gum, and reminders to swallow | Botulinum toxin Anticholinergics: glycopyrrolate sublingual atropine drops, ipratropium bromide spray |
| Sleep and Related Disorders | ||
| REM Sleep Behavior Disorder | Sleep hygiene, sleep environment safety modifications, and treatment of comorbid sleep disorders | Melatonin Benzodiazepines: clonazepam |
| Insomnia | CBT-I (first line), regular exercise, sleep hygiene, avoid naps and caffeine late in the day | Sedative-hypnotics: eszopiclone, zolpidem, zaleplon Melatonin Antidepressants: doxepin, trazodone |
| Excessive Daytime Sleepiness | Activity pacing, bright light therapy, and physical activity | Stimulants: methylphenidate, modafinil Caffeine |
| Fatigue | Energy conservation techniques, Qigong, short naps in early afternoon, regular exercise, hydration, and address underlying contributors | Stimulants: modafinil, methylphenidate MAO-B inhibitors: safinamide, rasagiline Antidepressant: doxepin |
| Other | ||
| Musculoskeletal Pain | Exercise, stretching, PT, massage, hot/cold therapy, yoga | Analgesics: acetaminophen, NSAIDs Adjust PD medications |
| Neuropathic Pain | Mindfulness, TENS (transcutaneous electrical nerve stimulation), PT, CBT | Gabapentin, pregabalin Antidepressants: duloxetine, amitriptyline, venlafaxine |
| Dystonic Pain | Stretching, PT, acupuncture, and massage | Botulinum toxin Optimize levodopa timing Anticholinergics: trihexyphenidyl, benztropine |
| Central Pain | Meditation, distraction techniques, exercise, CBT, sleep optimization | Dopaminergic therapy NMDA antagonist: amantadine Antidepressants: TCAs, SSRIs, SNRIs |
AChEI, acetylcholinesterase inhibitor; CBT, cognitive behavioral therapy; ED, erectile dysfunction; HRT, hormone replacement therapy; NRI, ;OAB, overactive bladder; PT, physical therapy; SNRIs, selective serotonin–norepinephrine reuptake inhibitors; SSRIs, selective serotonin-reuptake inhibitors; TCAs, tricyclic antidepressants
Figure 2
Pharmacologic Management of Nonmotor Symptoms in PD22-24
Non-Pharmacologic Management of Non-Motor Symptoms
Pharmacologic treatment often provides only partial relief for NMS in PD. In some cases, symptoms such as orthostatic hypotension, psychosis, or fatigue may worsen with dopaminergic medications. These limitations have led to greater interest in non-pharmacologic strategies that directly target quality of life, function, and independence.3,25
Many of these therapies are not supplemental but are foundational to care. When coordinated across disciplines, they help address overlapping symptoms and support patients holistically.
Physical Therapy and Exercise
Exercise benefits both motor and non-motor symptoms. It improves sleep, mood, fatigue, and cognition.1,27,28 Supervised, structured, and regular activity is most effective.1,28 Programs may include:
Aerobic training, such as walking, swimming, or cycling. These activities support autonomic regulation and sleep quality.
Strength training, especially when tailored to the individual. This helps reduce fatigue and preserve independence.
Balance and gait training to prevent falls and reduce fear of movement.
Group classes such as Tai Chi or dance. These combine physical movement with social connection and cognitive engagement.
Occupational Therapy
Occupational therapy supports daily function. It helps people adapt to fatigue, apathy, or cognitive decline through appropriate activity pacing, assistive devices, and environmental changes. Interventions can improve energy conservation, task completion, and roles at home and in the community. Participation in meaningful activities, such as hobbies or social groups, can also improve mood and reduce the impact of NMS, like depression or isolation.29
Speech and Swallowing Support
Speech-language pathologists manage communication and swallowing issues.
For dysarthria, treatments like Lee Silverman Voice Treatment (LSVT LOUD) can improve vocal volume and clarity30
For dysphagia, targeted strategies can reduce the risk of aspiration and support nutrition and hydration31
Although speech and swallowing are technically motor symptoms, they are included in the MDS Non-Motor Symptom Scale because they are often underrecognized and undertreated.
Nutrition and Diet
Dietary changes can address constipation, fatigue, medication absorption, and systemic inflammation. A Mediterranean or MIND-style diet has been associated with better outcomes in PD.32 Recommendations include:
Emphasizing fruits, vegetables, whole grains, fish, legumes, and healthy fats
Minimizing processed foods and added sugars
Staying well hydrated to reduce constipation and support blood pressure
Adjusting protein intake timing to improve levodopa absorption
Dietitians help adapt these recommendations to fit cultural preferences, swallowing issues, and medication schedules. When nurses provide patient counseling regarding dietary changes, they should ensure that the caregiver responsible for purchasing groceries and planning and preparing meals is present.
Mental Health and Cognitive Interventions
Cognitive behavioral therapy (CBT) is one of the most studied and effective non-pharmacologic interventions for NMS in PD. It has been shown to reduce depression, anxiety, apathy, and insomnia, and can improve coping skills and reduce social withdrawal.1,3 Cognitive behavioral therapy may be delivered in person or via telehealth and can be adapted for individuals with mild cognitive impairment.
Cognitive behavioral therapy for insomnia (CBT-I) is considered a first-line treatment for sleep initiation and maintenance problems.1,27 This approach is often effective without the need for medication and may be particularly useful when fatigue, anxiety, or other overlapping symptoms are present. Referral to a sleep specialist may be appropriate when symptoms persist despite treatment or when obstructive sleep apnea is suspected.
Additional non-pharmacologic strategies for mood and cognitive symptoms include supportive counseling, mindfulness-based approaches, and structured group therapy. These interventions may be used alone or in combination with pharmacologic treatment to enhance daily functioning and quality of life.
Complementary and Creative Therapies
Complementary therapies are increasingly used alongside traditional treatments. These include:
Yoga, Tai Chi, Qigong, and mindfulness may reduce symptoms of anxiety, depression, and sleep disturbance. These therapies also support relaxation, balance, energy regulation, and pain management.1,33
Acupuncture, which has been studied for motor and NMS may provide benefits for pain, sleep quality, and mood.33
Music and dance therapy may enhance mood, social connection, executive function, and motor performance.33
These interventions may also be delivered through community-based programs, which promote social engagement and help reduce fatigue, apathy, and isolation. Although more research is needed to standardize protocols and confirm long-term effects, these therapies offer a low-risk, patient-centered addition to care.
Self-Management Strategies
Patient-led behaviors play a key role in managing NMS. These strategies can be initiated independently or with guidance from a health professional.
Daily routine supports sleep regulation and improves medication effectiveness4
Sleep hygiene includes consistent sleep and wake times, a dark and quiet environment, and limiting caffeine and alcohol
Symptom tracking helps identify patterns, especially non-motor fluctuations5
Light physical activity supports mood, sleep, and fatigue1
Mindfulness or relaxation practices help reduce anxiety and improve sleep3
Hydration and dietary fiber support bowel regularity and help manage orthostatic symptoms11,32
Social connection improves motivation and may reduce fatigue and cognitive decline1
Mobile apps or journals can reinforce routines and improve adherence to self- care plans.5
Clear, consistent encouragement from the care team can help patients feel confident in adopting these practices. For instance, nurses can use regular assessment interviews as an opportunity to help the patient set goals related to self- management strategies and to determine whether to supplement or modify these strategies.
Coordinating Interdisciplinary Care
Effective non-pharmacologic care depends on teamwork. Therapists, nurses, dietitians, and mental health professionals all contribute to recognizing and managing NMS.5
Yet many patients do not receive this support. Nearly 40% of people with PD never see a neurologist, and far fewer are referred to physical, occupational, or speech therapy.34 Improving access to interdisciplinary services remains a critical goal in PD care.35
Practical Summary: Managing Non-Motor Symptoms
Pharmacologic and non-pharmacologic strategies often work best when used together. The table below provides an overview of both treatment types for common NMS. Consider this a framework for counseling and collaborative care discussions.
Pause and Ponder
Which non-motor symptoms associated with Parkinson’s disease have you seen in your patients?
Which treatments are being prescribed for those non-motor symptoms?
Advanced and Emerging Therapies for Non-Motor Symptoms of PD
Pharmacologic treatment of PD has traditionally focused on dopamine replacement to manage motor symptoms. However, this approach is often insufficient for NMS. In some cases, dopaminergic therapy can worsen issues such as orthostatic hypotension, hallucinations, or impulse control behaviors. A new generation of therapies is moving beyond dopamine to target the complex pathways involved in mood regulation, cognitive function, autonomic stability, and inflammation.
Pharmacologic Therapies Targeting Non-Motor Pathways
New medications are being developed to act on non-dopaminergic systems such as the serotonergic, cholinergic, glutamatergic, and noradrenergic pathways. These pathways are implicated in non-motor symptoms like depression, apathy, fatigue, and cognitive decline.36
Serotonergic agents are under investigation for depression and psychosis.
Noradrenergic therapies may help with fatigue and orthostatic hypotension.
Cholinergic modulation is being explored for memory and attention.
Glutamatergic drugs are being studied for apathy and mood symptoms.
Examples of investigational therapies include:
SAGE-718 is an NMDA receptor modulator that may improve working memory and executive function in mild cognitive impairment.
BHV-4157 (troriluzole) is a glutamate reuptake enhancer being studied for anxiety in Parkinson’s.
Safinamide is an MAO-B inhibitor with additional effects on glutamate release, which has shown promise in treating apathy and depressive symptoms25
Deep Brain Stimulation and Non-Motor Symptoms
Deep brain stimulation is widely used to treat motor fluctuations, but it may also improve some non-motor symptoms. Benefits have been reported in sleep quality, pain, and urinary urgency. These effects may result from modulation of basal ganglia circuits that influence motor and autonomic function.37
However, outcomes for mood and cognition are mixed. Deep brain stimulation can worsen depression, apathy, or executive dysfunction in some patients, particularly if these symptoms are present before surgery.37
Microbiome and Inflammation-Based Approaches
There is growing interest in the gut–brain axis and its role in PD. Alterations in the gut microbiome may contribute to constipation, systemic inflammation, and the misfolding of α-synuclein.4,11,38
Non-drug approaches such as dietary changes and probiotic use have shown benefits for gastrointestinal symptoms. For example, probiotics may improve constipation in Parkinson’s.11
Immunomodulatory agents are also under investigation:38
Ambroxol may improve lysosomal function and reduce the accumulation of neurotoxic proteins.
Sargramostim may modulate immune response and slow neurodegeneration.
These therapies reflect a broader shift toward modifying disease mechanisms, not just managing symptoms.
Non-Invasive Neuromodulation
Repetitive transcranial magnetic stimulation (rTMS) targets the prefrontal cortex and is being studied for symptoms like depression, apathy, and cognitive impairment. Results are mixed, and more research is needed to define optimal stimulation protocols and duration of benefit.25
Other techniques, including transcranial direct current stimulation (tDCS) and vagus nerve stimulation, are still in early stages of development. These approaches are not yet part of routine care but may offer new tools for treatment-resistant symptoms in the future.25
Case Study
A 61-year-old male patient, Mr. T, came to the clinic with his daughter, describing recent vomiting. The daughter explained to the physician that she believes the cause of vomiting is food poisoning from a spoiled leftover hamburger that he brought home from a restaurant. She states she opened his refrigerator and could smell a horrible odor. She told her father about the odor, but Mr. T told her, “There is no odor in the refrigerator and nothing wrong with that burger, so I ate it. Leave me alone. I’m tired.”
She also said that after he vomited, he mentioned, “I don’t care if I sit by the toilet with an upset stomach all day, because I have no friends and no one would notice or care.” She also told the doctor that she had asked him if he had any diarrhea from the probable food poisoning. He replied to her, “I don’t have diarrhea. I haven’t pooped in days and my poops are very hard.”
She added that he has always been energetic and kind, but has been exhausted and grumpy, and forgets to take his blood pressure medicine.
The physician thoughtfully assimilated these comments and asked if the loss or change in his ability to smell may be associated with smoking, or if he had fallen, had a head injury, or had sinus disorders. Mr. T answered “No” to all of those questions.
The physician asked more questions to dig deeper into the likely presence of depression using the Patient Health Questionnaire-9 (PHQ-9). The physician determined that the patient is experiencing symptoms of depression.
The physician asked about the patient’s bowel movement frequency and gut transit time. Based on the daughter’s recall of Mr. T’s comments, constipation was diagnosed.
The physician also inquired about complaints of urinary urgency, frequency, incontinence, or incomplete emptying. Mr. T admitted, “I haven’t been sleeping well and will get up several times during the night because I suddenly need to pee. Then I’ll watch TV, go back to bed, and suddenly need to get up again to pee again. My body is a mess.”
The doctor prescribed:
Mirabegron 25 mg once daily.39
Escitalopram 10 mg, take ½ tablet a day for 2 weeks, then increase to 1 tablet daily, for depression.
Drinking at least 6 glasses of water per day to help minimize constipation.
Mr. T resisted, saying, “I can’t. That will make me pee more.”
The doctor then added:
Eat more fiber
Eat small meals
Walk and exercise
Get over-the-counter psyllium, mix the recommended amount on the package with at least 8 ounces of liquid, such as water or juice, and drink it immediately
The doctor was beginning to suspect prodromal PD due to the presence of hyposmia, constipation, sleep disturbances, possible cognitive decline, and mood changes.
The doctor informed Mr. T, “I expect you to feel better soon with these instructions and prescriptions. Let me know if you don’t feel better soon, or if something isn’t working. I also believe something else may be going on with you. I am considering the whole picture of your medical history and your symptoms, and will give you a neurologic exam while you are here. Your disturbed sleep, loss of smell, and having to urinate frequently, along with forgetting and feeling no one
cares, makes me want to confirm there is no underlying cause of all of this happening to you at the same time.”
The neurologic exam was normal, as Mr. T is in the prodromal stage. Mr. T returned in 4 weeks for follow-up, telling the doctor, “I feel better.” The doctor will continue to watch out for signs of PD and will continue to screen for other NMS of PD, such as orthostatic hypotension.
Summary
Non-motor symptoms are a core part of PD. They may begin years before motor symptoms and can progress independently. Common NMS include depression, anxiety, apathy, cognitive decline, autonomic dysfunction, pain, fatigue, and sleep disturbances. These symptoms often impact daily life more than motor features and contribute significantly to caregiver burden and health care use.
Pharmacologic treatments are available for many NMS, but their effectiveness is variable. In some cases, dopaminergic medications may worsen symptoms such as psychosis, orthostatic hypotension, or impulse control disorders. A symptom- specific approach is often required, using agents such as antidepressants, cholinesterase inhibitors, antipsychotics, laxatives, and stimulants. Medication strategies are most effective when paired with non-drug interventions.
Non-pharmacologic therapies are essential to managing NMS. Exercise, physical and occupational therapy, cognitive behavioral therapy, diet, and sleep hygiene can improve mood, cognition, fatigue, and autonomic function. Creative and complementary practices such as mindfulness, music, and dance support emotional well-being and social connection. These approaches are not optional extras but are central to person-centered care.
Patient-led strategies such as establishing daily routines, tracking symptoms, staying physically active, and maintaining hydration can reinforce treatment goals. These behaviors are accessible and sustainable, especially when supported by the care team.
New treatments are being developed to target the biological mechanisms behind NMS. These include drugs that affect serotonergic, noradrenergic, and glutamatergic systems and therapies focused on the gut microbiome and brain
stimulation techniques. Although still in development, these approaches reflect a growing effort to address the underlying causes of PD rather than focusing only on symptom management.
When NMS are recognized early and addressed consistently, people with PD experience better daily function, improved quality of life, and greater satisfaction with care. A coordinated approach that combines medication, therapy, and lifestyle strategies is essential for effective, whole-person management.
Course Test
Which of the following options most accurately describes non- motor symptoms associated with Parkinson’s disease?
Drooling, shuffling gait, and hiccups
Constipation, depression, and sexual dysfunction
Resting tremor, restless leg syndrome, and gout
Apathy, glaucoma, and infections
Which statement below is not accurate regarding non-motor symptoms in individuals with Parkinson’s disease?
Some non-motor symptoms develop years before diagnosis and may offer early diagnostic clues during the prodromal phase.
Non-motor symptoms include constipation, REM sleep behavior disorder, vague shoulder pain, anxiety, and depression.
Some non-motor symptoms fluctuate in response to medication timing, worsening during “off” periods.
Non-motor symptoms include small handwriting due to bradykinesia and rigidity, which impairs fine motor control.
Which of the following statements is accurate regarding depression in patients presenting with Parkinson’s disease?
Depression is among the most frequently reported symptoms.
Depression affects 70-90% of these patients.
Slow gait is often mistaken for depression.
Impulse control disorders are often confused with depression.
Which medications are prescribed to Parkinson’s patients presenting with non-motor symptoms of orthostatic hypotension?
Oxybutynin, trospium
Lubiprostone, probiotics
Midodrine, fludrocortisone
Botulinum toxin, ipratropium
Which statement below correctly describes a pharmacologic strategy used in the treatment of Parkinson’s disease non-motor symptoms?
After botulinum toxin injections into striated muscles, clinical improvement may last 3–4 months
Topical salicylate cream alleviates restless leg syndrome
Psyllium is the most effective treatment for constipation
Midodrine and pyridostigmine are prescribed for anxiety
Which pharmacologic therapies are prescribed to treat Parkinson’s patients presenting with insomnia?
Glycopyrrolate, atropine drops, ipratropium
Rivastigmine, memantine, clozapine
Mirabegron, oxybutynin, diuretics
Eszopiclone, zolpidem, melatonin
Which physical therapy and exercise interventions are recommended for patients with non-motor symptoms in Parkinson’s disease?
Deep breathing exercises
Aerobic and strength training
Lee Silverman Voice Treatment
Dietary changes and meal planning
Which option below is not used to improve quality of life factors such as mood and cognitive symptoms in Parkinson’s patients?
Structured group therapy
Mindfulness-based approaches
Hydration and dietary fiber
Supportive counseling
Which group of interdisciplinary professionals is most likely to care for individuals with non-motor symptoms associated with Parkinson’s disease?
Speech or occupational therapist, dietitians, mental health professionals
Speech therapists, podiatrists, manicurists, and optometrists
Dermatologists, gastroenterologists, hair stylists, podiatrists
Dentists, radiologists, anesthesiologists, and immunologists
Which statement describes possible reasons for the delay in referral of individuals with Parkinson’s disease non-motor symptoms to specialists?
The Non-Motor Symptoms Questionnaire (NMSQ) frequently provides inaccurate data
There are critics of Braak’s hypothesis that unknown pathogens enter the body through the nasal cavity or the gut
The International Parkinson and Movement Disorder Society merged with the College of Rheumatology
The symptoms vary in intensity throughout the day, are hard to detect, and are underreported
References
Zhang Y, Liu S, Xu K, et al. Non-pharmacological therapies for treating non- motor symptoms in patients with Parkinson's disease: a systematic review and meta-analysis. Front Aging Neurosci. 2024;16:1363115. Published 2024 Apr
26. doi:10.3389/fnagi.2024.1363115
Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord. 2015;30(12):1591-1601. doi:10.1002/mds.26424
Weintraub D, Aarsland D, Chaudhuri KR, et al. The neuropsychiatry of Parkinson's disease: advances and challenges. Lancet Neurol. 2022;21(1):89-
102. doi:10.1016/S1474-4422(21)00330-6
Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021;397(10291):2284-2303. doi:10.1016/S0140-6736(21)00218-X
Bhidayasiri R, Panyakaew P, Trenkwalder C, et al. Delivering patient-centered care in Parkinson's disease: Challenges and consensus from an international panel. Parkinsonism Relat Disord. 2020;72:82-87. doi:10.1016/j.parkreldis.2020.02.013
Frank C, Chiu R, Lee J. Parkinson disease primer, part 1: diagnosis. Can Fam Physician. 2023;69(1):20-24. doi:10.46747/cfp.690120
Rodriguez-Blazquez C, Schrag A, Rizos A, Chaudhuri KR, Martinez-Martin P, Weintraub D. Prevalence of Non-Motor Symptoms and Non-Motor Fluctuations in Parkinson's Disease Using the MDS-NMS. Mov Disord Clin Pract. 2020;8(2):231-239. Published 2020 Dec 21. doi:10.1002/mdc3.13122
Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson's disease. Lancet Neurol. 2021;20(5):385-397. doi:10.1016/S1474- 4422(21)00030-2
Boura I, Poplawska-Domaszewicz K, Spanaki C, et al. Non-Motor Fluctuations in Parkinson's Disease: Underdiagnosed Yet Important. J Mov Disord. 2025;18(1):1-16. doi:10.14802/jmd.24227
Chaudhuri KR, Schrag A, Weintraub D, et al. The movement disorder society nonmotor rating scale: Initial validation study [published correction appears in Mov Disord. 2020 Oct;35(10):1892. doi: 10.1002/mds.28266.]. Mov Disord. 2020;35(1):116-133. doi:10.1002/mds.27862
Chen Z, Li G, Liu J. Autonomic dysfunction in Parkinson's disease: Implications for pathophysiology, diagnosis, and treatment. Neurobiol Dis. 2020;134:104700. doi:10.1016/j.nbd.2019.104700
Ignatavicius DD. Concepts of care for patients with problems of the central nervous system: the brain. In: Ignatavicius DD, Rebar CR, Heimgartner NM, eds. Medical-Surgical Nursing: Concepts for Clinical Judgment and Collaborative Care. 11th ed. Elsevier; 2024:(Ch) 39.
Gallagher J, Gochanour C, Caspell-Garcia C, et al. Long-Term Dementia Risk in Parkinson Disease. Neurology. 2024;103(5):e209699. doi:10.1212/WNL.0000000000209699
Dodet P, Houot M, Leu-Semenescu S, et al. Sleep disorders in Parkinson's disease, an early and multiple problem. NPJ Parkinsons Dis. 2024;10(1):46. Published 2024 Feb 29. doi:10.1038/s41531-024-00642-0
Tai YC, Lin CH. An overview of pain in Parkinson's disease. Clin Park Relat Disord. 2019;2:1-8. Published 2019 Nov 28. doi:10.1016/j.prdoa.2019.11.004
Carpi M, Pierantozzi M, Cofano S, et al. Both Motor and Non-Motor Fluctuations Matter in the Clinical Management of Patients with Parkinson's Disease: An Exploratory Study. J Pers Med. 2023;13(2):242. Published 2023 Jan 29. doi:10.3390/jpm13020242
Klingelhoefer L, Reichmann H. Pathogenesis of Parkinson disease--the gut- brain axis and environmental factors. Nat Rev Neurol. 2015;11(11):625-636. doi:10.1038/nrneurol.2015.197
Rietdijk CD, Perez-Pardo P, Garssen J, van Wezel RJ, Kraneveld AD. Exploring Braak's Hypothesis of Parkinson's Disease. Front Neurol. 2017;8:37. Published 2017 Feb 13. doi:10.3389/fneur.2017.00037
Soraci L, et al. Toll-like receptors and NLRP3 inflammasome-dependent pathways in Parkinson’s disease: mechanisms and therapeutic implications. J Neurol. 2023;270(3):1346-1360. doi:10.1007/s00415-022-11491-3
Ben-Shlomo Y, Darweesh S, Llibre-Guerra J, Marras C, San Luciano M, Tanner
C. The epidemiology of Parkinson's disease. Lancet. 2024;403(10423):283-
292. doi:10.1016/S0140-6736(23)01419-8
Abdo WF, Borm GF, Munneke M, Verbeek MM, Esselink RA, Bloem BR. Ten steps to identify atypical parkinsonism. J Neurol Neurosurg Psychiatry. 2006;77(12):1367-1369. doi:10.1136/jnnp.2006.091322
Church FC. Treatment Options for Motor and Non-Motor Symptoms of Parkinson's Disease. Biomolecules. 2021;11(4):612. doi: 10.3390/biom11040612 .
Pieber TR, Svehlikova E, Mursic I, et. al. Blood glucose response after oral lactulose intake in type 2 diabetic individuals. World J Diabetes. 2021
;12(6):893-907. doi: 10.4239/wjd.v12.i6.893
Frank C, Chiu R, Lee J. Parkinson disease primer, part 2: management of motor and nonmotor symptoms. Can Fam Physician. 2023;69(2):91-96. doi: 10.46747/cfp.690291
Wamelen DJV, Rukavina K, Podlewska AM, Chaudhuri KR. Advances in the Pharmacological and Non-pharmacological Management of Non-motor Symptoms in Parkinson's Disease: An Update Since 2017. Curr Neuropharmacol. 2023;21(8):1786-1805. doi:10.2174/1570159X20666220315163856
Tanner CM, Ostrem JL. Parkinson's Disease. N Engl J Med. 2024;391(5):442-
452. doi:10.1056/NEJMra2401857
Amara AW, Memon AA. Effects of Exercise on Non-motor Symptoms in Parkinson's Disease. Clin Ther. 2018;40(1):8-15. doi:10.1016/j.clinthera.2017.11.004
Osborne JA, Botkin R, Colon-Semenza C, et al. Physical Therapist Management of Parkinson Disease: A Clinical Practice Guideline From the American Physical Therapy Association [published correction appears in Phys Ther. 2022 Aug 1;102(8):pzac098. doi: 10.1093/ptj/pzac098]. Phys Ther. 2022;102(4):pzab302. doi:10.1093/ptj/pzab302
Tofani M, Ranieri A, Fabbrini G, et al. Efficacy of Occupational Therapy Interventions on Quality of Life in Patients with Parkinson's Disease: A
Systematic Review and Meta-Analysis. Mov Disord Clin Pract. 2020;7(8):891- 901. Published 2020 Oct 2. doi:10.1002/mdc3.13089
Xu H, Bao Z, Liang D, et al. Speech and Language Therapy for Voice Problems in Parkinson's Disease: A Meta-Analysis. J Neuropsychiatry Clin Neurosci. 2020;32(4):344-351. doi:10.1176/appi.neuropsych.19020044
Gandhi P, Steele CM. Effectiveness of Interventions for Dysphagia in Parkinson Disease: A Systematic Review. Am J Speech Lang Pathol. 2022;31(1):463-
485. doi:10.1044/2021_AJSLP-21-00145
Rees J, Ryan J, Laws M, Devine A. A comprehensive examination of the evidence for whole of diet patterns in Parkinson's disease: a scoping review. Nutr Neurosci. 2024;27(6):547-565. doi:10.1080/1028415X.2023.2233727
Deuel LM, Seeberger LC. Complementary Therapies in Parkinson Disease: a Review of Acupuncture, Tai Chi, Qi Gong, Yoga, and
Cannabis. Neurotherapeutics. 2020;17(4):1434-1455. doi:10.1007/s13311- 020-00900-y
Pearson C, Hartzman A, Munevar D, et al. Care access and utilization among medicare beneficiaries living with Parkinson's disease. NPJ Parkinsons Dis. 2023;9(1):108. Published 2023 Jul 10. doi:10.1038/s41531-023-00523-y
Roberts AC, Rafferty MR, Wu SS, et al. Patterns and predictors of referrals to allied health services for individuals with Parkinson's disease: A Parkinson's foundation (PF) QII study. Parkinsonism Relat Disord. 2021;83:115-122. doi:10.1016/j.parkreldis.2020.11.024
Jing XZ, Yuan XZ, Luo X, Zhang SY, Wang XP. An Update on Nondopaminergic Treatments for Motor and Non-motor Symptoms of Parkinson's Disease. Curr Neuropharmacol. 2023;21(8):1806-1826. doi:10.2174/1570159X20666220222150811
Kurtis MM, Rajah T, Delgado LF, Dafsari HS. The effect of deep brain stimulation on the non-motor symptoms of Parkinson's disease: a critical review of the current evidence. NPJ Parkinsons Dis. 2017;3:16024. Published 2017 Jan 12. doi:10.1038/npjparkd.2016.24
Morris HR, Spillantini MG, Sue CM, Williams-Gray CH. The pathogenesis of Parkinson's disease. Lancet. 2024;403(10423):293-304. doi:10.1016/S0140- 6736(23)01478-2
Myrbetriq. Prescribing Information. Astellas Pharma US, Inc. April 2018.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace
those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2025: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.