PARKINSON’S DISEASE: A COLLABORATIVE APPROACH TO ADDRESSING MOTOR SYMPTOMS
Faculty:
Kimberly Valenta, MD
Kimberly Valenta is a freelance medical writer and editor. She studied chemistry at Mount Holyoke College and medicine at Northwestern University. After completing her anesthesiology residency, she joined the faculty at Stanford University, where she cared for patients and taught medical students and residents. In 2020, she transitioned to writing and editing full-time. She holds a certificate in medical writing and editing from the University of Chicago and is an active member of the American Medical Writers Association.
Pamela Sardo, PharmD, BS
Pamela Sardo is a freelance medical writer, pharmacist licensed in 3 states, and the founder/principal at Sardo Solutions. She received her BS from the University of Connecticut and a PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, pharmaceutical manufacturing, and managed healthcare across broad therapeutic classes and disease states.
Kristina (Tia) Neu, RN
Kristina (Tia) Neu is a licensed Registered Nurse and author currently developing in-service training for healthcare professionals. She is a National Board-Certified Health & Wellness and Lifestyle Medicine Coach. Her work experience includes work in several areas of the healthcare profession, including psychiatric nursing, medical nursing, motivational health coaching, chronic case management, dental hygiene, cardiac technician, and surgical technician.
Topic Overview:
Parkinson's disease (PD) is a chronic, progressive neurodegenerative disorder characterized by motor and non-motor symptoms. Its rising prevalence and significant impact on patients, caregivers, and healthcare systems make it an important area of focus for a patient-centered, multidisciplinary approach to care. The exact cause of PD remains unknown, but in most cases, it is likely due to genetic and environmental factors. Motor symptoms are the hallmark of PD. The cardinal motor symptoms of PD are bradykinesia, rest tremor, rigidity, and postural instability. Individuals experience unique combinations of symptoms and rates of progression. A multi-pronged approach for patients, with pharmacological and non-pharmacological interventions, is important
because each patient is unique in clinical presentation, and symptom onset varies. Increasing awareness of characteristics, the pathophysiology of Parkinson’s disease and nonmotor symptoms, new treatment options, and roles of interprofessional team members should lead to improved patient understanding of their condition, improved quality of life, symptom control, and increased caregiver awareness.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-25-007-H01-P
Pharmacy Technician 0669-0000-25-008-H01-T
Credits: 3 contact hour(s) (0.3 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $8.99
Estimated time to complete activity: 3 contact hour(s) (0.3 CEU(s)), including Course Test and course evaluation
Release Date: February 13, 2025 Expiration Date: February 13, 2028
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
Secondary Audiences: Other healthcare professionals, such as nurses, physicians, or others who may be part of a healthcare team, may be interested in this educational topic. Healthcare team roles and approaches to patient care are discussed in this activity. No state board, professional organization, or credentialing body has evaluated this activity to determine whether it meets the continuing education requirements of nurses, physicians, or other professions not listed under the “Target Audience” section above. Always verify with individual employers or supervisors whether they will accept this educational activity upon completion.
How to Earn Credit: From February 13, 2025, through February 13, 2028, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
List the characteristic motor symptoms of Parkinson’s Disease
Apply a basic understanding of Parkinson’s disease pathophysiology to explain the rationale for drug selection.
Compare and contrast the different classes of medications used to treat motor symptoms
Identify opportunities for collaboration within the multidisciplinary care team to optimize patient outcomes
Disclosures
The following individuals were involved in developing this activity: Kimberly Valenta, MD, Pamela Sardo, PharmD, BS, and Kristina (Tia) Neu, RN. Kimberly Valenta, Pamela Sardo, and Kristina (Tia) Neu have no conflicts of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2025: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Parkinson's Disease: A Collaborative Approach to Addressing Motor Symptoms
Introduction
Parkinson's disease (PD) is a chronic, progressive neurodegenerative disorder characterized by motor and non-motor symptoms. Its rising prevalence and significant impact on patients, caregivers, and healthcare systems make it an important area of focus for healthcare teams. This course is one of a two-part series that aims to enhance understanding of PD to empower meaningful contributions to a patient-centered, multidisciplinary approach to care. This course is focused on the recognition and management of the motor symptoms of PD.
Epidemiology
Prevalence and Incidence
Parkinson's disease is the fastest-growing neurodegenerative disease. In adults over age 45 years, it currently affects approximately 572 per 100,000 individuals.1 Its global burden, in terms of death and disability, has more than doubled over the past 2 decades,2 and it is expected to affect more than 12 million people globally by 2040.3
This increase in incidence and prevalence likely stems from factors such as population aging, improved diagnostic accuracy, and prolonged survival. However, the higher incidence observed in some regions, mainly industrialized nations, suggests that environmental factors may play a role.2
The risk of developing PD steadily increases with age. Of adults diagnosed with PD, 5-10% are diagnosed before age 50, and approximately 25% are diagnosed before age 65.2 Incidence increases from 47-77 cases per
100,000 individuals 45 years of age and older to 108-212 cases per 100,000 individuals 65 years old age and older.1
The male-to-female ratio is 2:1.1 Onset for males is earlier, and they live more years with disability. They also have a greater risk of cognitive decline compared to females. In contrast, females have a greater risk of developing dyskinesia (uncontrolled, involuntary movement), depression, and urinary complaints than males. Females also receive less care and are less represented in clinical trials.2
Data suggest disparities in incidence and prevalence among different racial and ethnic groups. Further research is needed to understand how this reflects genetic or environmental differences or healthcare access disparities. At present, incidence is highest in East Asia and in high-income countries in Europe.2
Causes and Modifying Factors
The exact cause of PD remains unknown, but in most cases, it is likely due to a combination of genetic and environmental factors. Current research points towards several key areas.
Genetic Factors
While responsible for a minority of PD cases, several specific single gene (monogenic) mutations have been identified as causing familial PD. Genetic variants in the gene GBA are the most common genetic risk factor for PD, with up to 30% penetrance.4 It is most common in populations with Ashkenazi Jewish or North African ancestry.2 Additionally, researchers have found four other autosomal dominant mutations with incomplete penetrance that cause later-onset PD (LRRK2, CHCHD2, VPS35, SNCA) and three autosomal recessive mutations that cause early-onset PD (PRKN, PINK1, DJ1).4
Genome-wide association studies have identified over 90 genetic risk loci implicating pathways such as mitochondrial dysfunction, lysosomal dysfunction, and neuroinflammation. Many of these are near the known causative genes.1 Overall, genes are thought to contribute to PD development in approximately 20% of PD cases.1
Environmental Factors
Exposure to certain environmental toxins, including pesticides, herbicides, solvents, and heavy metals, has been linked to an increased PD risk.2 Residential or occupational exposures to pesticides (paraquat, rotenone, 2,4-dichlorophenoxyacetic acid, and several organochlorines and organophosphates) and chlorinated solvents (trichloroethylene, perchloroethylene) are of particular concern.1
Studies have also suggested that high dairy consumption could also increase PD risk, potentially through exposure to the organochlorine pesticide heptachlor.1
Emerging evidence suggests that head injuries increase the risk of developing PD, possibly through mechanisms like neuroinflammation and disruption of the blood-brain barrier.2 One study showed that adults who experienced traumatic brain injury after age 55 had a 44% increased risk of developing PD within 5 to 7 years.5
Lastly, it is possible that certain lifestyle factors, such as diet, smoking, coffee intake, caffeine consumption, and the amount of physical activity, may influence PD risk.2
Clinical Presentation
Parkinson's disease affects everyone differently. Individuals experience unique combinations of symptoms and rates of progression. What may be most troubling for one person might be less of a concern for another. This
affects how people describe their symptoms and can make diagnosis challenging.2
Prodromal Phase
Parkinson's disease typically begins with a prodromal phase. This is the period before the onset of motor symptoms, when individuals may experience various non-motor symptoms.
Hyposmia (decreased sense of smell) and rapid eye movement (REM) sleep behavior disorder (loss of normal muscle atonia during REM sleep, leading to the active enactment of dreams) are most common.2
Signs of autonomic dysfunction, such as orthostatic hypotension, constipation, urinary dysfunction, erectile dysfunction, and impaired thermoregulation, may first appear during this phase and then progress.2
Retrospective studies suggest the prodromal phase can last anywhere from a few years to decades before motor symptoms emerge,2 but it does not occur in all individuals with PD.6
There is significant interest in learning how to recognize the prodromal phase. By the time motor symptoms appears, up to 75% of substantia nigra dopaminergic neurons have lost their function.1
The clinical setting is an ideal time to catch the prodromal phase of PD, leading to early disease detection. Primary care professionals can spend extended time with their patients and are the hub of the patient's care. They may have a bigger picture of the patient's overall health and what testing has already been completed. For example, the primary care physician may fit the puzzle together when it comes to nonspecific symptoms such as constipation, blood pressure issues, or sleep concerns. Early recognition of PD may positively impact the quality of life, and once disease-modifying therapies are available, may eventually enable clinicians to prevent progression to clinically diagnosable PD altogether.7,8
Motor Symptoms
Motor symptoms are the hallmark of PD. The cardinal motor symptoms of PD are bradykinesia, rest tremor, rigidity, and postural instability. Other motor symptoms (see Table 1 for definitions) are hypomimia, micrographia, festination, shuffling gait, dysarthria, dysphagia, and dystonia.
Bradykinesia
Bradykinesia means slow movement, but in PD, it refers to slower and smaller movements.3 Early in PD, bradykinesia affects the limbs asymmetrically. Someone with bradykinesia might have trouble getting started with a movement (like taking a first step) or may find their movements get progressively slower and smaller as they continue the action (like their handwriting getting smaller across the page).
A doctor will often assess bradykinesia by asking the patient to tap their fingers, open and close their hand, or quickly turn their palm up and palm down. Reduced movement speed and size are key signs of PD and help differentiate it from other movement disorders.3
Resting Tremor
Resting tremor is a rhythmic shaking that typically occurs when the affected limb is completely relaxed and supported. It is often described as a "pill-rolling" motion between the thumb and fingers. It tends to decrease or disappear with voluntary movement or when the limb is actively held in a posture. The tremor may increase with mental stress.
Similar to bradykinesia, the resting tremor is usually asymmetric. It can involve the upper and/or lower limbs. A feature that can help distinguish it from other tremors, such as essential tremor, is its higher frequency of 4-6 Hertz.3 Although a resting tremor is often the first symptom individuals report, its absence does not rule out PD.
Rigidity
Rigidity is an increased muscle tone and resistance to passive movement. It is sometimes called "lead-pipe rigidity." This resistance is present regardless of how quickly or slowly the examiner moves the limb. A "cogwheel" phenomenon, which is a ratcheting sensation felt during passive movement, can be present due to the underlying tremor. However, this cogwheeling alone is not sufficient to diagnose rigidity. The examiner must detect a consistent resistance throughout the range of motion.3
Rigidity is distinct from spasticity or paratonia, which are related to other neurological issues. With rigidity, the resistance remains constant throughout the passive movement of the limb. This contrasts with spasticity, where the resistance increases with faster movement, and paratonia, where the resistance increases and decreases unexpectedly throughout the movement.
Postural Instability
Postural instability is an impaired ability to maintain upright posture and balance during movements. A stooped posture, small, shuffling steps, difficulty turning, and reduced arm swing are some signs of postural instability. It is progressive and is a later-developing symptom of PD.3
Postural instability increases the risk of falls and serious injury. Embarrassment and fear of falling can lead to decreased physical activity and social isolation. It can significantly impact daily life and independence. Cognitive decline associated with advanced PD further affects the ability to perform tasks requiring simultaneous physical and mental effort, making it harder for individuals to compensate for balance issues or adapt to changing environments. The following table summarizes common motor symptoms in PD.
Table 1
Parkinson’s Disease Motor Symptoms
| Motor Symptom | Description |
| Bradykinesia | Slow and small movements. |
| Resting tremor | Rhythmic shaking in a resting limb. |
| Rigidity | Increased muscle tone and resistance to passive movement of a limb. |
| Postural instability | Impaired ability to maintain upright posture and balance during movement. |
| Hypomimia | Loss of facial expression. |
Micrographia | Small handwriting that occurs due to bradykinesia and rigidity, which impair the fine motor control needed for writing. |
Festinating gait | A walking pattern with rapid, small steps done in an attempt to keep the center of gravity (COG) in between the feet while the trunk leans forward involuntarily and shifts the COG forward. |
| Shuffling gait | A walking pattern in which the foot is still moving when it hits the ground. |
Dysarthria | A motor speech disorder that can manifest in various ways, including monotonous speech (lacking variations in pitch and loudness), breathy or hoarse voice quality, reduced volume, imprecise pronunciation of consonants, or rapid, mumbled speech. (Atalar) |
Dysphagia | A swallowing impairment that can lead to malnutrition, difficulty with medication intake, and aspiration pneumonia, which is a major cause of death in PD.10 |
| Dystonia | A sustained or repetitive muscle twisting, spasm or cramping. |
Diagnosis
The International Parkinson and Movement Disorders Society (MDS) defines PD as “a core clinical motor syndrome (parkinsonism) accompanied by substantia nigra pars compacta neurodegeneration and synuclein deposition.”4
According to this definition, PD is a diagnosis that can only be definitively made postmortem. In life, PD diagnosis is based on typical parkinsonian motor features in the absence of signs that would suggest an alternative diagnosis. Clinical expert opinion is the current gold standard for PD diagnosis because, at present, no validated biomarkers are available.4
Diagnostic Criteria
The MDS-PD clinical diagnostic criteria were designed for use in research but can help guide diagnosis in practice.9 These criteria involve a two-step process:
First, confirm the presence of parkinsonism.
Then, assess whether the parkinsonism is due to PD, using supportive and exclusionary criteria.
Parkinsonism is diagnosed when the following features are present and are not attributable to other conditions:9
Asymmetric limb bradykinesia, AND one or both of the following:
Rigidity of major joints (limb, neck)
Rest tremor of 4-6 Hz that is suppressed with movement initiation
Note that postural instability is not part of the MDS-PD criteria for parkinsonism. This is because it usually occurs in the later stages of PD. If it develops early, it suggests an alternative diagnosis.9
After confirming the presence of parkinsonism, the next step is to determine its cause by reviewing various neurological signs and symptoms. Specific signs and symptoms either support the diagnosis of PD (supportive criteria) or support another diagnosis (absolute exclusion criteria and red flags).
Supportive Criteria
Supportive criteria are positive factors that support a diagnosis of PD, increasing confidence that the individual does, in fact, have the disease. Examples include the following:9
Significant and sustained improvement in response to levodopa (one month trial of levodopa, 600 mg up to 1000 mg daily, is recommended)2,3
Developing dyskinesias (involuntary movements) as a side effect of levodopa
The classic "pill-rolling" resting tremor in one hand
Reduced sense of smell, an objective indicator validated as being specific to PD
Red Flags
Red flags are signs that make a PD diagnosis less likely, but they do not definitively rule it out. Examples of red flags include the following:9
Rapidly worsening walking problems requiring a wheelchair within 5 years of the first symptoms
No symptom progression for 5 years or more (PD is progressive)
Severe difficulty speaking or swallowing developing early on
Problems with breathing, specifically inspiratory stridor (wheezing while breathing in) or frequent sighing
Significant problems with orthostatic hypotension or bladder/bowel control within 5 years of the first symptoms
Severe stiffness or twisting in the neck (antercollis) or contractures (permanent tightening of muscles) within 10 years of the first symptoms
No non-motor symptoms even after 5 years of disease (e.g., REM sleep behavior disorder, loss of smell, autonomic dysfunction, depression, anxiety)
Symptoms or signs clearly linked to issues with spinal cord function (pyramidal tract signs)
Parkinsonian symptoms affecting both sides of the body equally from the very beginning (PD typically starts on one side)
Absolute Exclusion Criteria
Absolute exclusion criteria, also called negative features, are specific signs and symptoms that strongly suggest the individual does not have PD. Their presence points towards a different diagnosis altogether. Examples include the following:9
Problems with coordination (ataxia) indicating a possible cerebellar issue
Specific eye movement abnormalities (like sustained downward gaze) suggestive of progressive supranuclear palsy
Certain types of early-onset dementia (frontotemporal dementia) that have their distinct pathologies
Parkinsonian symptoms primarily affecting the legs and no other symptoms, which is unusual in PD and raises suspicion for vascular parkinsonism
Symptoms while the person is being treated with a medicine known to cause parkinsonism or if the parkinsonism started shortly after stopping such medication
Loss of sensory function in different parts of the body (cortical sensory loss), or trouble doing tasks learned previously (apraxia), or difficulty with comprehending or expressing speech (aphasia)
Although ancillary testing is not usually done, imaging tests and olfactory testing may help certain cases, especially when alternative diagnoses are being considered.3 Likewise, genetic testing is not routinely part of the PD workup, but it may help to clarify the prognosis and risk for family members.4
Diagnostic Challenges
Parkinson's disease should be suspected in any patient who presents with parkinsonism, balance problems, changes in gait, or the non-motor symptoms common to PD.3 Common early non-motor symptoms to watch out for include constipation, REM sleep behavior disorder, loss of smell, asymmetric vague shoulder pain, and depression.2
Despite the existence of the MDS-PD clinical diagnostic criteria, PD diagnosis remains challenging. On average, it takes 10 years to diagnose PD following the first noticeable symptoms. Most primary care physicians are familiar with the cardinal motor symptoms of PD but are less aware of the non-motor symptoms, which tend to present earlier. Younger individuals who present with predominantly lower extremity symptoms or who do not have a resting tremor are also more likely to have their diagnosis delayed.2
Even when PD is suspected, up to 15% of people are diagnosed incorrectly.2 Many conditions can cause or mimic parkinsonism (Table 2).3
Table 2
Other Causes of Parkinsonism3
| Condition | Description | Compared to PD |
| Due to antidopaminergic | Less prominent gait | |
| medications such as | disturbance | |
| Medication- induced parkinsonism | typical neuroleptics (e.g., haloperidol), atypical neuroleptics at higher doses (e.g., risperidone | Symptoms may be more symmetrical Upper limb symptoms are the most common |
| >0.5 mg/d), and | Usually improves after the | |
| antiemetics (e.g., | medication is discontinued |
| prochlorperazine, metoclopramide) | ||
Vascular parkinsonism |
A secondary form of parkinsonism caused by ischemia in the basal ganglia | May have an abrupt onset and stepwise decline Symmetrical bradykinesia May affect the lower limbs more Minimal response to levodopa |
Progressive supranuclear palsy |
Neurodegenerative disorder caused by abnormal accumulation of tau protein in the brain | Postural instability with early falls Truncal rigidity Vertical supranuclear gaze palsy (extraocular movement) Startled facial expression Rapid progression Up to 50% may have some response to levodopa |
Multiple system atrophy, parkinsonian type |
Severe neurodegenerative disorder characterized by a combination of autonomic dysfunction and parkinsonism | Early and severe autonomic dysfunction (orthostatic hypotension, urinary incontinence, erectile dysfunction) Rapid progression Poorly responsive to levodopa |
Dementia with Lewy bodies | Neurodegenerative disorder characterized by dementia plus parkinsonism, visual hallucinations, fluctuations in awareness, and/or REM sleep behavior disorder | Dementia presents early Parkinsonism symptoms may respond to levodopa, but hallucinations and confusion may be exacerbated |
Normal pressure hydrocephalus | A clinical syndrome characterized by the triad of gait disturbance, urinary incontinence, and cognitive impairment. | “Magnetic gait,” which is a walking pattern with shortened step length and height Cognitive dysfunction |
| Enlarged cerebral ventricles are seen on MRI. | Urinary urgency or incontinence No response to levodopa |
Case Presentation: Recognizing Red Flags
“Good morning, Mrs. Smith," Raj, the pharmacist, greeted warmly. "I see you're picking up your new levodopa prescription. How are you feeling today?"
"A little nervous, to be honest," Mrs. Smith admitted. "The neurologist said this might be Parkinson's, but I'm not entirely convinced. I mean, the tremor in my right hand is definitely getting worse, but I've also been having so much trouble with my balance lately. I've fallen twice in the past month, and my walking has gotten so much worse so quickly. I'm using a cane now, and I'm worried I'll need a walker soon." She sighed. "It just seems like everything is happening so fast."
Raj listened attentively, a concerned look creeping onto his face. He recalled from Mrs. Smith's profile that she was relatively young for a Parkinson's diagnosis, only 58 and that her initial symptoms had started just a year ago. The rapid progression of her gait problems, combined with the recurrent falls, was definitely a red flag. "Mrs. Smith," he began gently, "I appreciate you sharing that. Your concerns about your balance are important. While some people with Parkinson's do experience balance issues, the speed at which yours have developed, along with the falls, is something we need to discuss with your neurologist. It might be worthwhile to explore some additional testing to ensure we have the right diagnosis." He paused. "I'm going to call Dr. Jones' office now and see if we can get you in sooner for a follow-up. How does that sound?"
Pathophysiology
The exact pathogenesis of PD is multifactorial, complex, and remains elusive. Motor symptoms of parkinsonism are associated with Lewy bodies and
loss of dopaminergic neurons in the substantia nigra. As mentioned earlier, the nervous system, neurotransmitters, protein aggregates, genetics, and the environment contribute to the pathology of PD.11
The development and progression of PD are influenced by abnormal aggregation of α-synuclein and the spreading of pathology between the gut, brainstem, and higher brain regions.12 The Figure below, entitled Proposed Molecular Pathogenesis, provides a visual description of the proposed pathogenesis of PD.
Proposed Molecular Pathogenesis12
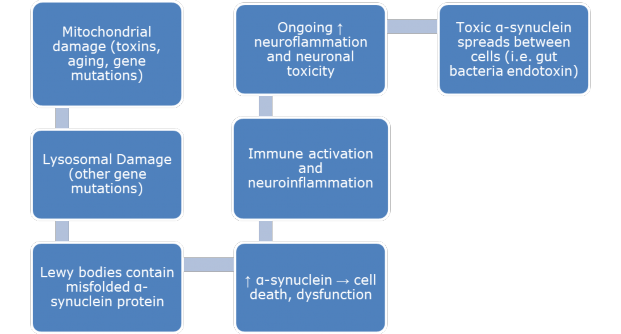
Lewy bodies contain the protein α-synuclein, which traps mitochondria and lysosomes and disrupts cell function, leading to damaged neurons.12 Mutations in α-synuclein lead to aggregation or clumping, suggesting that α- synuclein dysfunction is an early step in PD. There is an abundance of α- synuclein in brain neurons and elsewhere.12 For example, the presence of α- synuclein in neurons surrounding the gut might contribute to constipation in individuals with PD.
There are many interrelated factors to consider when addressing PD. Immune responses are generally protective. In PD, inflammation involving immune cells, cytokines, and chemokines can damage neurons.13 Inflammatory mediators, such as TNFα or COX2, can contribute to the degeneration and death of dopamine neurons. When dopamine cell death occurs, bradykinesia is a result.11
Tremor is a challenge in patients with PD. The cerebello-thalamo-cortical circuit may be essential in tremor. In addition to the loss of dopamine, serotonin and noradrenaline are additional possible contributors to the development of tremors.14 There may also be a role of the cholinergic system in PD tremor.14
One theory proposes that PD may start in the periphery, such as in the gut or the olfactory system, and spread to the subcortical and cortical brain.12 Other studies have suggested that some patients might have brainstem- predominant disease.12
Parkinson’s Disease Management A Multidisciplinary Approach
Parkinson's disease is a complex neurodegenerative disorder, and there is a growing appreciation for the value of a multidisciplinary team in caring for these patients. After surveying neurologists from 20 PD expert centers about the role of the multidisciplinary clinical care teams for PD patients, Radder, et al. (2020),15 provided the following consensus statement:
Parkinson's disease is a complex, multidimensional condition with cognitive, psychological, and social ramifications, as well as motor and non- motor signs. The clinical manifestations are only partially amenable to pharmacological or surgical treatment. This makes it impossible for one healthcare professional in any discipline to cover all complexities and diversities of symptoms and to deliver all management options.
To support this collaborative approach, various care team models have been proposed. These models consistently place the patient and their care partners at the center, supported by a primary care/community team, a core team specializing in PD, and an extended multidisciplinary team tailored to individual patient needs.2,15
The primary/community team provides general, ongoing support and serves as a liaison between the patient and specialists. It includes:
Primary care physician (family medicine, internist): Oversees general health, manages comorbidities, and provides initial points of contact for health concerns, making referrals to specialists as needed. Acts as a care coordinator to improve overall communication among providers and maintain continuity of care.
Community nurse: Supports medication management, reinforces patient education, and provides basic health monitoring.
Pharmacist: Optimizes medication regimens, monitors for drug interactions and adverse effects, addresses adherence challenges, and provides patient education on medications and disease management.
The core PD team consists of specialists with expertise in PD who work together to develop and implement a comprehensive care plan. The core team includes:
Neurologist (preferably a movement disorder neurologist): Leads the team, diagnoses PD, manages medications, monitors disease progression, and coordinates care with other specialists. Referral to a movement disorders specialist is highly recommended, especially for atypical presentations or diagnostic uncertainty.3
Parkinson's disease nurse specialist: Provides expert guidance on PD management, medication administration, and symptom management and serves as a key point of contact for patients and their families.
Registered dietician: Assesses nutritional needs, develops dietary plans to address PD-related challenges (e.g., constipation, weight loss), and provides education on maintaining a healthy diet. Nutritional interventions, combined with exercise and avoiding exposure to toxins, may favorably modify the risk of PD.
Occupational therapist: Focuses on adapting daily activities, recommending assistive devices, and modifying the home environment to maximize independence and safety for individuals experiencing functional limitations due to PD.
Physical therapist: Creates individualized exercise programs targeting mobility, balance, gait, and motor control. It may also address specific motor challenges like freezing of gait using compensatory strategies as needed.2,16
Speech-language pathologist: Evaluates and treats communication (dysarthria) and swallowing difficulties (dysphagia) often seen in PD. Speech- language pathologists develop individualized plans to improve speech clarity, voice volume, and swallowing safety.16 Problems such as drooling may be managed with sublingual atropine drops or salivary-gland botulinum toxin injections.1
Mental health professional (psychologist, psychiatrist): Addresses the emotional and cognitive challenges related to PD, including depression, anxiety, apathy, and psychosis. May provide therapy (including cognitive behavioral therapy [CBT]), counseling, and medication management.2,17 CBT has been effective in the treatment of both anxiety and depression related to PD.17
Social worker: Connects patients and caregivers with support services, provides counseling, assists with financial and legal matters, and advocates for patient needs.2
The extended multidisciplinary team consists of additional specialists who may be consulted based on the individual's specific needs. This team may include the following professions:
Gastroenterologist
Geriatrician
Neurosurgeon
Nursing home physician (aka SNFist)
Pain medicine specialist
Urologist
Clinical geneticist
Dentist
Neuro-ophthalmologist
Pulmonologist
Physical medicine and rehabilitation specialist
Sleep medicine physician
Despite these recommendations for a robust, multidisciplinary team, few patients with PD can access such a team. A shortage of specialists, financial/resource constraints, and an underappreciation of the expertise and potential contributions of these specialists are the likely causes. Approximately 40% of patients with PD do not see a neurologist at all.3,18
Pharmacologic Management
Levodopa and Adjunct Therapies for Motor Symptoms
A multi-pronged approach for patients, with pharmacological and non- pharmacological interventions, is important because each patient is unique in clinical presentation, and symptom onset varies. Medications will not cure PD or slow its progression. One goal is to replace the lost dopamine. Levodopa (L-dopa), a dopamine receptor agonist, or a monoamine oxidase type B inhibitor are options to provide initial motor symptom benefit. Carbidopa/L- dopa is the gold standard medication. Carbidopa and L-dopa have very short
half-lives, so medication timing is very important. Efficacy with long-acting medications is similar to immediate-release dosage forms.
Early in the course of the disease, a missed dose may not be noticed due to subtle symptoms, and the patient may not have sufficient dopaminergic neurons to maintain function.19 The remaining dopaminergic neurons decrease over time, requiring more complex pharmacologic intervention to manage symptoms. When there are fewer dopaminergic neurons, more levodopa (L- dopa) is needed. As the disease progresses, the therapeutic window of medication effectiveness narrows.19
Treatment options for PD continue to expand. The International Parkinson and Movement Disorder Society summarized that effective options for monotherapy of early PD include non-ergot dopamine agonists, oral L-dopa preparations, selegiline, and rasagiline.20 L-dopa has been reported to be superior compared with dopamine agonists.21 For adjunct therapy, nonergot dopamine agonists, rasagiline, and zonisamide provide relief.20 Most non- ergot dopamine agonists, pergolide, levodopa ER, levodopa intestinal infusion, entacapone, opicapone, rasagiline, zonisamide, and safinamide, are clinically useful among other options for motor symptoms.20 L-dopa is more likely than dopamine agonists to cause dyskinesia.21 Amantadine and clozapine are also prescribed for symptom relief.
Patients with PD experience motor symptoms with ‘On’ time and ‘Off’ time. The ’On’ time is when the symptoms are controlled with medication. The ‘Off’ time is when there is a decreased duration of time with no symptoms and an increased incidence of dyskinesia.
Daily regimens and doses are highly variable and must be individualized to maximize efficacy and minimize adverse effects. Considering genetic factors, some genes demonstrate a good response to treatment with L-dopa, and other genes in individuals with PD have a poor, variable, or uncertain response to L-dopa.22 Always consult the full prescribing information for each medication for comprehensive safety and efficacy information. Some commonly prescribed treatments are listed in the tables below.
Table 3
Common Levodopa-Containing Medications for Parkinson’s Disease 23-28
| Select Agents | Typical Dose | Common Adverse Effects |
| Nausea, loss of | ||
| Carbidopa/levodopa IR, ODT | Individualize up to 200/2,000 mg daily in divided doses | appetite, lightheadedness, confusion, dyskinesias, hallucinations, |
| impulsivity | ||
| Nausea, loss of | ||
| appetite, | ||
| Carbidopa/levodopa ER | Individualize up to 525/2,100 mg daily | lightheadedness, confusion, dyskinesias, hallucinations, |
| impulsivity | ||
| Nausea, loss of | ||
| appetite, | ||
| Carbidopa/levodopa enteral suspension | Individualize to 2,000 mg levodopa over 16 hours | lightheadedness, confusion, dyskinesias, hallucinations, impulsivity, |
| gastrointestinal or | ||
| insertion complications | ||
| Nausea, loss of | ||
| Individualize up to | appetite, | |
| Foscarbidopa/foslevodo pa subcutaneous injection | 3,525 mg foslevodopa (approximately 2,500 mg levodopa) (preferably in the | lightheadedness, confusion, dyskinesias, hallucinations, impulsivity, |
| abdomen via pump) | infusion/catheter site reactions | |
| Individualize up to | Nausea, loss of | |
| 1200 mg levodopa | appetite, | |
| Carbidopa/ levodopa/ | daily. Experience with | lightheadedness, |
| entacapone | daily doses above | confusion, dyskinesias, |
| 1600mg of entacapone | hallucinations, | |
| is limited | impulsivity, urine |
| discoloration, diarrhea, and abdominal pain | ||
| Max dose per OFF | Max dose per OFF | |
| Levodopa inhalation | period is 84 mg. Max | period is 84 mg. Max |
| powder | daily dosage is 420 mg | daily dosage is 420 mg |
| by inhalation only | by inhalation only |
IR, immediate release; ODT, oral disintegrating tablets; ER, extended-release
Table 4
Common Dopamine Agonists for Parkinson’s Disease29-35
| Select Agents | Typical Dose | Common Adverse Effects |
Pramipexole |
Individualize up to 4.5 mg daily by week 7 | Nausea, dizziness, somnolence, insomnia, constipation, asthenia, hallucinations |
Pramipexole Dihydrochloride ER |
Individualize up to 4.5 mg | Somnolence, nausea, constipation, dizziness, fatigue, hallucinations, dry mouth, muscle spasms, and peripheral edema |
Ropinirole |
Individualize dose, titrate to a maximum daily dose of 24 mg | Nausea, somnolence, dizziness, syncope, leg edema, vomiting, dyskinesia, hallucination, sweating |
Ropinirole XL |
Individualize dose up to a maximally recommended dose of 24 mg/day | Somnolence, abdominal pain/discomfort, dizziness, headache, and constipation, dyskinesias, hallucination, abdominal pain/discomfort, orthostatic hypotension |
| For intermittent use. |
Yawning, drowsiness, somnolence, dyskinesias, postural hypotension, rhinorrhea, nausea, vomiting, hallucination, confusion, edema/swelling | |
| Individualize and titrate | ||
| to effect and tolerance. | ||
| Maximum | ||
| Apomorphine hydrochloride injection | recommended dose is 0.6 mL. Pretreat with an | |
| antiemetic 3 days | ||
| before initiation but for | ||
| no longer than 2 | ||
| months | ||
| For Intermittent use. | Nausea, | |
| Maximum of 5 doses | oral/pharyngeal soft | |
| Apomorphine | per day. | tissue swelling, |
| hydrochloride | Maximum single dose is | oral/pharyngeal soft |
| sublingual film | 30 mg, Pretreat with an | tissue pain, |
| antiemetic 3 days | paraesthesia, dizziness, | |
| before initiation | somnolence | |
| Nausea, vomiting, | ||
| Individualize dose, | somnolence, | |
| applied to the skin, up | application site | |
| Rogitotine transdermal system | to 6 mg/24 hours for early-stage disease and up to 8 mg/24 hours | reactions, dizziness, anorexia, sleep disturbances, |
| for advanced-stage | hyperhidrosis, visual | |
| disease | disturbance, peripheral | |
| edema, dyskinesia |
ER, extended-release; XL, extended-release
Table 5
Common Amantadine Formulations for Parkinson’s Disease36-38
| Select Agents | Typical Dose | Common Adverse Effects |
| 200 mg daily and may | Nausea, insomnia, | |
| be split into 100 mg | Blurry vision and/or | |
| twice a day. A | impaired mental acuity, | |
| Amantadine | suboptimal response | dizziness, depression, |
| may increase to 400 | hallucination, | |
| mg daily with close | lightheadedness, mood | |
| supervision | changes |
Amantadine ER capsules | Individualize and increase to the recommended daily dosage of 274 mg | Hallucination, dizziness, dry mouth, peripheral edema, constipation, falls, and orthostatic hypotension |
Amantadine ER tablets | Individualize to a maximum daily dose of 322 mg once daily in the morning | Nausea, dizziness/ lightheadedness, and insomnia |
ER, extended-release
Table 6
Additional Select Pharmaceutical Agents for Parkinson’s Disease39-48
| Select Agents | Typical Dose | Common Adverse Effects |
| Adenosine Receptor Antagonists | ||
Istradefylline | Individualize up to a maximum of 40 mg once daily | Dyskinesia, dizziness, constipation, nausea, hallucination, and insomnia |
| MAO B Inhibitors | ||
Selegiline ODT |
Individualize up to 2.5 mg once a day | Constipation, skin disorders, vomiting, dizziness, dyskinesia, insomnia, dyspnea, myalgia, rash |
Rasagiline |
Individualize up to 1 mg once daily | Flu, arthralgia, depression, dyspepsia, falls, headache, hallucination, dizziness, diarrhea |
Safinamide |
Individualize up to 100 mg once daily | Dyskinesia, falls, nausea, insomnia, hypertension, serotonin syndrome, hallucination, impulse control |
| COMT Inhibitors | ||
Entacapone | Administer concomitantly with each levodopa/carbidopa dose to a maximum 1600 mg daily | Dyskinesia/hyperkinesi a, nausea, urine discoloration, diarrhea, abdominal pain |
Tolcapone | Administer concomitantly with levodopa/carbidopa dose to recommended 100 mg tid. Use 200 mg only if the benefit is justified due to adverse effects | Hepatocellular injury, dyskinesia, nausea, sleep disorder, anorexia, muscle cramps, orthostatic complaints, dizziness, hallucination |
Opicapone |
Recommended dosage is 50 mg orally once daily at bedtime | Arrhythmia, increased heart rate, syncope, dyskinesia, sleepiness, hallucination, impulse control |
| Anticholinergics | ||
Benztropine |
Individualize orally to 1 to 2 mg, 0.5 mg to 6 mg parenterally daily | Gastrointestinal complaints, anhydrosis, and cumulative action may lead to tachycardia, dysuria, weakness, confusion, hallucination |
Trihexyphenidyl tablets or solution |
Individualize to the maximum dose of 12 to 15 mg daily | Intraocular pressure change, anhidrosis, dry mouth, dizziness, nausea, nervousness, hallucination |
COMT, catechol-O-methyltransferase; MAO, monoamine oxidase; ODT, orally disintegrating tablet
Preventing Medication Side Effects
The most effective way to prevent side effects while maintaining the quality of life in patients with PD is to consider medication choices and avoid certain drug interactions carefully.
Avoiding Dopamine-Blocking Medications such as metoclopramide, prochlorperazine, and promethazine.
Caution with Certain Pain Medications. While sometimes necessary, meperidine, tramadol, and methadone can interact with MAO-B inhibitors.
Interactions with MAO-B Inhibitors are also contraindicated when combined with sympathomimetic drugs such as phenylpropanolamine or ephedrine.
Dietary Restrictions with MAO-B Inhibitors. Avoid foods high in tyramine, such as aged cheeses, red wine, and herring.
Non-Pharmacologic Management
Current pharmacological treatments for PD, while offering some relief, often leave patients with significant unmet needs, especially regarding specific motor symptoms like freezing of gait and postural instability. These limitations have increased interest and research into non-pharmacological approaches to managing PD.49 These interventions play an important role in improving quality of life, maintaining function, and promoting overall well-being for individuals with PD.
Exercise and Physical Therapy
Exercise is fundamental to non-pharmacological PD management, providing consistent benefits across motor and non-motor symptoms. If available, individuals should work with a physical therapist (PT) or clinical exercise physiologist specialized in PD for a full functional evaluation and recommendations.49-51
Aerobic exercise: Activities like brisk walking, cycling, or swimming improve cardiovascular health, motor function, sleep, and mood. Patients are advised to aim for moderate-to-high-intensity exercise for at least 30–40 minutes three times per week.
Resistance training: Strength training with weights or resistance bands builds strength and power, improves motor symptoms, and enhances quality of life. Progressive programs have been shown to be most effective. Patients are recommended to train 2-3 non-consecutive days per week for at least 30 minutes and to perform 10-15 reps per major muscle group.
Balance and agility training: These exercises improve postural stability, reduce falls, and build confidence. Programs often incorporate multidirectional stepping, weight shifting, and dynamic balance activities. Activity examples include yoga, tai chi, dance, and boxing. Supervision may be required for safety.
Stretching: Sustained stretching with deep breathing or dynamic stretching is recommended at least 2-3 days per week but is most effective if done on a daily basis.
Multitasking and gait training: Therapists can design exercises to improve specific daily tasks, such as turning or walking while doing another activity (dual-task training). Gait training, focusing on improving walking patterns (speed, stride length, rhythm) via activities such as treadmill work, overground practice, and assistive devices/cues, is another valuable intervention. Robotic-assisted gait training and treadmill training specifically have shown positive effects on both gait and reducing motor disease severity.
Community-based exercise: Group programs foster social interaction, improve motor symptoms, enhance balance, and increase quality of life. These programs can be adapted for different ability levels and settings.
Patient Handout
Parkinson's Exercise Recommendations handout from the Parkinson’s Foundation:
https://www.parkinson.org/library/fact-sheets/exercise-recommendations
Occupational Therapy
Occupational therapy (OT) is considered a core non-pharmacologic component of PD care, focused on maximizing the quality of life and independence for individuals with this progressive condition. Occupational therapy helps people with PD adapt to the challenges of daily living by developing personalized strategies to maintain function and participation in meaningful activities for as long as possible. Studies have demonstrated that OT interventions lead to significant improvements in quality of life.52
Occupational therapy interventions address many practical aspects of daily living impacted by PD. OTs work with individuals to overcome motor challenges affecting routines such as dressing, bathing, eating, and grooming, recommending assistive devices and home modifications as needed. Importantly, OTs help individuals maintain or resume engaging in hobbies, social activities, and even work. This support for participating in meaningful activities can significantly reduce feelings of depression and anxiety and improve overall mood and well-being.49,52 For example, participation in community-based programs, like dance classes or support groups, is useful for psychosocial adaptation and may enhance compliance in those receiving multidisciplinary team care.49
Patient Handout
Occupational Therapy handout from the Parkinson’s Foundation:
https://www.parkinson.org/sites/default/files/documents/occupational- therapy.pdf
Speech Therapy
Speech-language pathologists (SLPs) play an important role in helping people with PD manage speech, communication, and swallowing difficulties. For speech problems (dysarthria) like soft voice (hypophonia), imprecise articulation, or monotone speech, SLPs use a variety of techniques, including specialized exercises and strategies like Lee Silverman Voice Treatment (LSVT LOUD).53
LSVT LOUD is an intensive program focusing on increasing vocal loudness, and research shows it can have significant and long-lasting positive effects. Other approaches include working on breath support, articulation, and intonation or using external cues (like rhythmic beats) to improve speech clarity and rhythm.53
For swallowing difficulties (dysphagia), SLPs assess swallow function and make recommendations to improve the safety and efficiency of swallowing. They might recommend modified food textures (e.g., thickened liquids) or specific swallowing maneuvers to help prevent choking or aspiration. Additionally, exercises to improve coordination and strength of the swallowing muscles are frequently employed. Collaboration with other members of the care team, like dieticians and occupational therapists, is essential to provide comprehensive support.54
Patient Handout
Speech & Swallowing in Parkinson’s handout from the Parkinson’s Foundation:
https://www.parkinson.org/sites/default/files/documents/Speech- Swallowing-fact-sheet.pdf
Nutritional Therapy
A healthy, balanced dietary pattern may improve symptoms and potentially slow disease progression in PD. The Mediterranean diet and similar eating styles (like the MIND diet) are consistently associated with positive outcomes.55
Taking levodopa with a meal high in protein can interfere with levodopa absorption in the gut. Protein redistribution diets are a dietary strategy that helps to manage this interaction. These diets don’t restrict overall protein intake but aim to optimize the timing of protein consumption. For example, individuals may be encouraged to consume a reduced portion of their daily protein during the day when it corresponds with their levodopa therapy and then consume a higher portion of their daily dietary protein in the evening.55
It is important to note that many individual factors, like trouble swallowing (dysphagia) or loss of smell (hyposmia), can affect diet. Therefore, personalized advice from a registered dietitian is important to optimize food choices for symptom management. Additionally, diet quality often declines after a PD diagnosis, emphasizing the importance of nutritional support. Individuals living with PD benefit most when their individual food preferences, cultural preferences, limitations such as access, mobility and cost of foods, cooking ability, and available support at home are taken into consideration before advice and recommendations for specific interventions are applied to improve nutritional outcomes.54
Patient Handout
Nutrition and PD handout from the Parkinson’s Foundation:
https://www.parkinson.org/sites/default/files/documents/nutrition- 2022.pdf
Other Non-Pharmacological Interventions
Several other interventions have shown promise:
Mindfulness, yoga, dance, creative arts therapies, and other mind- body practices offer benefits for stress reduction, mood, and physical function.17
Support groups provide a sense of community and support for individuals with PD and their caregivers.
Education programs teach patients and caregivers about PD, its symptoms, management strategies, and available resources and support self-management and overall well-being.2
When integrated as part of a comprehensive, multidisciplinary approach to care, this diverse range of non-pharmacological interventions significantly improves the management of PD and the quality of life for those living with this complex condition.
Advanced and Emerging Therapies
While pharmacological and non-pharmacological interventions form the basis of current PD management, advanced device-based therapies offer important options, particularly as the disease progresses and symptoms become more complex or severe. If patients are considering one of these advanced options, their multidisciplinary team will expand to include a neurosurgeon, a neuropsychologist, and possibly a neuroradiologist.
Some of the currently available device-based therapeutic options are listed below.
Deep Brain Stimulation
Deep brain stimulation (DBS) involves surgically implanting electrodes in specific brain regions (usually the subthalamic nucleus or globus pallidus) to modulate neuronal activity with electrical impulses. A neurostimulator implanted under the skin in the chest delivers these impulses.2
Deep brain stimulation is typically reserved for individuals with advanced PD experiencing motor complications, such as tremor, rigidity, and dyskinesias (involuntary movements), that do not respond adequately to medication.1,2
Deep brain stimulation can offer a significant improvement in motor symptoms and quality of life, and the motor benefits may persist for up to 15 years. However, DBS is not a cure and does not typically address all symptoms caused by PD or necessarily benefit all individuals. For example, DBS has not been shown to improve postural instability or non-motor symptoms.1
Focused Ultrasound
Focused ultrasound is a non-invasive technique that uses high-intensity focused ultrasound waves to create precise lesions in targeted brain areas. Currently approved for treating essential tremor, this approach is being investigated in trials in those individuals with PD for whom medication alone is insufficient and shows some promise, though limited evidence, in treating tremor-dominant PD.1
Continuous drug delivery systems
Continuous drug delivery systems aim to provide a more continuous and stable delivery of medication, reducing motor fluctuations experienced by
those whose symptoms return as the dosage of their regularly prescribed medications wears off ("off" periods). There are two available methods:
Levodopa-carbidopa intestinal gel pump therapy: Delivers levodopa- carbidopa directly into the small intestine via a surgically placed tube, which minimizes side effects and may allow for a higher rate of treatment tolerance.2
Apomorphine infusion (approved in Europe): Subcutaneous apomorphine infusion provides continuous delivery of this dopamine agonist, improving the amount of “on” time and reducing motor fluctuations and dyskinesias.2
These advances represent important progress in managing complex PD. Ongoing research continues to explore new and repurposed medications, gene therapies, and neurosurgical interventions, driven by improved understanding of PD's underlying pathophysiology, including the role of genetics, protein aggregation (a-synuclein), neuroinflammation, and mitochondrial dysfunction.1,2,12
Future Directions
Researchers are actively exploring several promising avenues to improve PD treatment and potentially slow or even stop disease progression. Many of these focus on the underlying causes of PD, including:
Targeting alpha-synuclein: This protein plays a central role in PD, and researchers are working to develop therapies that reduce its abnormal clumping (aggregation) and spread throughout the brain.12 This includes immunotherapy approaches (like vaccines) currently in clinical trials.2
Protecting brain cells: Strategies include boosting the cell's natural repair and protective mechanisms (targeting lysosomes, mitochondria) and reducing inflammation and oxidative stress.12 Some existing medications are being "repurposed" for PD based on their effects on these pathways. Examples of repurposed drugs include ambroxol, a
cough suppressant, exenatide, a GLP1 agonist, and terazosin, a prostate drug.2
Restoring lost dopamine: Research is ongoing in cell transplants and infusions of growth factors to replace or support the damaged dopamine-producing brain cells.2,12
In addition, more accurate ways to diagnose early PD through biomarkers (biological indicators of disease), especially in blood or other accessible tissue, and better methods for measuring disease progression (like digital tools and remote monitoring) are also in development.2,4
The field of gene therapy (transferring genes into the brain to replace defective components) remains another area of promise.12 These advancements hold hope for improving outcomes in individuals with PD.
Case Study: Patient Counseling and Education
Pharmacists can play an important role in empowering patients and caregivers through education and counseling. Key areas include:
Medication management: Provide detailed information about medications, including dosing, administration, potential side effects, and drug interactions.
Disease education: Explain the progressive nature of PD, symptom management strategies, and the importance of adherence to treatment plans.
Lifestyle counseling: Encourage healthy lifestyle choices, including regular exercise, balanced nutrition, and stress-reducing techniques.
Referral and support: Connect patients and caregivers to support groups, community resources, and other members of the multidisciplinary care team.
Non-motor symptom discussions: Ensure the patient understands the importance of reporting NMS, such as autonomic dysfunction, sleep disorders, cognitive issues, and neuropsychiatric symptoms (depression, psychosis) and that these may necessitate adjunctive
pharmacologic therapy and non-pharmacological strategies, which can be initiated early in disease course2
Patient and caregiver perceptions of rehab services should be addressed: A study showed that caregivers of PD patients often undervalue OT and emphasize the benefits of PT, which influences referrals and outcomes. This can be addressed through education16
The following interaction between a pharmacist and a patient exemplifies how a caregiver or patient may be educated or counseled regarding the patient’s PD management plan.
Mr. S., 65 years old, has just moved to your neighborhood. He brings in the following prescriptions to the pharmacy:
Carbidopa/levodopa 25 mg/250 mg. Take one tablet at 6 am, 9 am, noon, 3 pm, 6 pm, 9 pm.
Carbidopa/levodopa ER 50 mg/200 mg. Take one tablet at midnight.
Ropinirole 2 mg. Take one tablet at 9 am, 3 pm, 9 pm.
Amantadine 100 mg. Take one tablet at 9 am and 3 pm.
He tells the pharmacist that he likes his new doctor. He told the pharmacist, “The doctor was kind and thorough with my physical exam. The doctor asked me so many questions. He drew blood and placed a referral to a neurologist for me. I had taken my meds before my appointment, so I felt good when I was there. Now that I am here, my stiffness is back, and I am tired, and it is harder to walk. I feel like I am shuffling, and my right arm won’t be still. I forgot to tell the doctor that has been happening sometimes.”
He also informed the pharmacist that he liked the new nurse because she was very nice and told him someone would visit his home. He added, “My wife is exhausted because she must bring me to all my appointments. The nurse said she will teach my wife about something called respite. She also asked me whether I had fallen. She really cared about me even though the office was busy.”
He admits to the pharmacist, “I take one other medication but forgot to tell the doctor about that one. I can’t recall what it is and lost the prescription bottle in the move.”
The pharmacist understands that this patient is presenting with an advanced stage of PD. The patient might be experiencing medications wearing off or the symptoms may be due to the absence of an unknown medication. Reviewing the prescription profile for this new patient, the pharmacist recalls that COMT inhibitors make more levodopa available for transport across the blood brain barrier and considers the possibility that the missing medication may be a COMT inhibitor.
The pharmacist asks the patient “Would you recognize the other drug name if you hear it?”
The patient replies, “Yes.”
The pharmacist asks, “Does the name opicapone or entacapone sound familiar to you?”
The patient replies, “Yes, the ‘enter’ drug. That’s it.” The pharmacist tells the patient he will call the physician.
The pharmacist called the doctor’s office and explained to the medical assistant that the patient forgot about one additional medication, and it may be entacapone because the name ‘enter’ was familiar to the patient. The pharmacist was transferred to the nurse and informed the nurse of the patient's statements and symptom descriptions and that ‘enter’ was familiar to the patient. The pharmacist mentioned that entacapone can increase the half-life of levodopa, and it is usually taken with each dose of carbidopa/levodopa. The nurse informed the physician of the pharmacist's call. The physician called the patient at home for further discussion and then called the pharmacy at the end of the day with the following new medication: Entacapone 200 mg. Take one tablet at 6 am, 9 am. Noon, 3 pm, 6 pm, 9 pm.
The patient returned to the pharmacy the following week and told the pharmacist that he felt much better now that he was again taking the medication he lost in the move.
Summary
Parkinson's disease is a chronic, progressive neurodegenerative disorder characterized by motor and non-motor symptoms. It is the fastest-growing neurodegenerative disease. The exact cause of PD remains unknown, but in most cases, it is likely due to a combination of genetic and environmental factors.
Parkinson's disease is a complex neurodegenerative disorder. Motor symptoms are the hallmark of PD. The MDS-PD clinical diagnostic criteria were designed for use in research but can help guide diagnosis in practice.
There is a growing appreciation for the value of a multidisciplinary team in caring for PD patients through a holistic, collaborative approach. Healthcare professionals who educate their patients and engage in medication optimization and care coordination can significantly improve the quality of life for those living with PD.
Course Test
Which of the following is the most characteristic pathological finding in Parkinson’s disease?
Beta-amyloid plaques
TDP-43 inclusions
Lewy bodies and α-synuclein aggregation
Tau tangles
Which of the following motor symptoms is required for diagnosing Parkinson’s disease?
Resting tremor
Bradykinesia
Postural instability
Rigidity
Which of the following is a major limitation of current pharmacologic therapy for Parkinson’s disease?
Long-term levodopa use is associated with dyskinesias
Dopamine agonists are more effective than levodopa in treating bradykinesia
Monoamine oxidase-B (MAO-B) inhibitors can slow disease progression
Anticholinergic medications are the first-line treatment for all Parkinson’s patients
Which of the following is NOT considered a common prodromal symptom of Parkinson’s disease?
Hyposmia
REM sleep behavior disorder
Visual field loss
Constipation
A patient with Parkinson’s disease reports difficulty with daily tasks such as buttoning a shirt, handwriting, and using utensils. Which referral is most appropriate?
Neurologist
Occupational therapist
Speech-language pathologist
Physical therapist
What is one of the biggest challenges in implementing multidisciplinary care for Parkinson’s disease?
The approach is only beneficial for newly diagnosed patients.
Multidisciplinary care teams do not address non-motor symptoms.
Many healthcare systems lack financial support and reimbursement for multidisciplinary care.
Parkinson’s disease is best managed by a single healthcare provider.
Which option below provides information to remember about the carbidopa/levodopa/entacapone combination?
Individualize up to 1200 mg levodopa daily. Experience with daily doses above 1600mg of entacapone is limited
The maximum dose per OFF period is 84 mg, and the max daily dosage is 420 mg by inhalation
Individualize up to 4.5 mg daily by week 7, then titrate to a maximum daily dose of 24 mg
Individualize up to a maximum of 40 mg once daily of levodopa, 80 mg of carbidopa, and 120 mg of entacapone
Which pharmaceutical agent below is not a dopamine agonist?
Ropinirole
Selegiline
Pramipexole
Apomorphine
A medical center has started a Parkinson’s disease clinic. One day per month, patients see a multidisciplinary team within a 4-hour period. The core PD team members will likely include:
Podiatrist, mental health professional, optometrist, hematologist
Dentist, optometrist, urologist, manicurist
Neurologist, dietician, occupational therapist, physical therapist
Infectious disease physician, hematologist, dentist, geriatrician
A speech-language pathologist treating a PD patient
evaluates and treats communication and the patient’s swallowing difficulties.
often develops plans to improve the ergonomic location of an office computer.
evaluates the patient’s need for a specialist referral to podiatry.
often prescribes antibiotics when the patient has a sore throat and is hoarse.
References
Tanner CM, Ostrem JL. Parkinson's Disease. N Engl J Med.
2024;391(5):442-452. doi:10.1056/NEJMra2401857
Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021;397(10291):2284-2303. doi:10.1016/S0140-6736(21)00218-X
Frank C, Chiu R, Lee J. Parkinson disease primer, part 1: diagnosis. Can Fam Physician. 2023;69(1):20-24. doi:10.46747/cfp.690120
Ben-Shlomo Y, Darweesh S, Llibre-Guerra J, Marras C, San Luciano M, Tanner C. The epidemiology of Parkinson's disease. Lancet. 2024;403(10423):283-292. doi:10.1016/S0140-6736(23)01419-8
Gardner RC, Burke JF, Nettiksimmons J, Goldman S, Tanner CM, Yaffe
K. Traumatic brain injury in later life increases risk for Parkinson disease. Ann Neurol. 2015;77(6):987-995. doi:10.1002/ana.24396
Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson's disease. Lancet Neurol. 2021;20(5):385-397. doi:10.1016/S1474-4422(21)00030-2
Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson's disease. Mov Disord. 2015;30(12):1600-1611. doi:10.1002/mds.26431
Bhidayasiri R, Panyakaew P, Trenkwalder C, et al. Delivering patient- centered care in Parkinson's disease: Challenges and consensus from an international panel. Parkinsonism Relat Disord. 2020;72:82-87. doi:10.1016/j.parkreldis.2020.02.013
Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord. 2015;30(12):1591-1601. doi:10.1002/mds.26424
Suttrup I, Warnecke T. Dysphagia in Parkinson's Disease. Dysphagia. 2016;31(1):24-32. doi:10.1007/s00455-015-9671-9
Kalia LV, Lang AE. Parkinson's disease. Lancet. 2015;386(9996):896- 912. doi: 10.1016/S0140-6736(14)61393-3
Morris HR, Spillantini MG, Sue CM, Williams-Gray CH. The pathogenesis of Parkinson's disease. Lancet. 2024;403(10423):293-304. doi:10.1016/S0140-6736(23)01478-2
Marogianni C, Sokratous M, Dardiotis E, Hadjigeorgiou GM, Bogdanos D, Xiromerisiou G. Neurodegeneration and Inflammation-An Interesting Interplay in Parkinson's Disease. Int J Mol Sci. 2020;21(22):8421. doi: 10.3390/ijms21228421
Pirker W, Katzenschlager R, Hallett M, Poewe W. Pharmacological Treatment of Tremor in Parkinson's Disease Revisited. J Parkinsons Dis. 2023;13(2):127-144. doi: 10.3233/JPD-225060
Radder DLM, Nonnekes J, van Nimwegen M, et al. Recommendations for the Organization of Multidisciplinary Clinical Care Teams in Parkinson's
Disease. J Parkinsons Dis. 2020;10(3):1087-1098. doi:10.3233/JPD- 202078
Roberts AC, Rafferty MR, Wu SS, et al. Patterns and predictors of referrals to allied health services for individuals with Parkinson's disease: A Parkinson's foundation (PF) QII study. Parkinsonism Relat Disord. 2021;83:115-122. doi:10.1016/j.parkreldis.2020.11.024
Weintraub D, Aarsland D, Chaudhuri KR, et al. The neuropsychiatry of Parkinson's disease: advances and challenges. Lancet Neurol. 2022;21(1):89-102. doi:10.1016/S1474-4422(21)00330-6
Pearson C, Hartzman A, Munevar D, et al. Care access and utilization among medicare beneficiaries living with Parkinson's disease. NPJ Parkinsons Dis. 2023;9(1):108. Published 2023 Jul 10. doi:10.1038/s41531-023-00523-y
Stocchi F, Bonamartini A, Vacca L, Ruggieri S. Motor fluctuations in levodopa treatment: clinical pharmacology. Eur Neurol. 1996;36 Suppl 1:38-42. doi:10.1159/000118882
Pringsheim T, Day GS, Smith DB, et.al.; Guideline Subcommittee of the AAN. Dopaminergic Therapy for Motor Symptoms in Early Parkinson Disease Practice Guideline Summary: A Report of the AAN Guideline Subcommittee. Neurology. 2021;97(20):942-957. doi: 10.1212/WNL.0000000000012868
Fox SH, Katzenschlager R, Lim SY, et.al; Movement Disorder Society Evidence-Based Medicine Committee. International Parkinson and movement disorder society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson's disease. Mov Disord. 2018;33(8):1248-1266. doi: 10.1002/mds.27372
Jia F, Fellner A, Kumar KR. Monogenic Parkinson's Disease: Genotype, Phenotype, Pathophysiology, and Genetic Testing. Genes (Basel). 2022;13(3):471. doi: 10.3390/genes13030471
Sinemet. Prescribing Information. Merck and Co., Inc. March 2020.
Crexont. Prescribing Information. Amneal Specialty. August 2024.
Duopa. Prescribing Information. Abbvie. September 2024.
Vyalev. Prescribing information. Abbvie. October 2024.
Stalevo. Prescribing Information. Orion Corporation. September 28, 2010.
Inbrija. Prescribing Information. Acorda Therapeutics, Inc. December 2022.
Mirapex. Prescribing Information. Boehringer Ingelheim International GmbH. May 2018.
Mirapex ER. Prescribing Information. Boehringer Ingelheim International GmbH. July 2024.
Ropinerole. Prescribing Information. Intas Pharmaceuticals Limited. August 2017.
Requip XL. Prescribing Information. GlaxoSmithKline. July 2021.
Kynmobi. Prescribing Information. May 2020.
Apokyn. Prescribing Information. US WorldMeds, LLC. March 2017.
Neupro. Prescribing Information. UCB Inc. July 2021.
Gocovri. Prescribing Information. Adamas Pharma. August 2017.
Osmolex ER. Prescribing Information. Vertical Pharmaceuticals, LLC. February 2018.
Amantadine. Prescribing Information. Marlex Pharmaceuticals Inc October 23, 2024.
Nourianz. Prescribing Information. Kyowa Kirin, Inc. May 2020.
Zelapar. Prescribing Information. Catalent Pharma Solutions Limited. June 2021.
Azilect. Prescribing Information. Teva Pharmaceutical Industries Ltd. August 2003.
Xadago. Prescribing Information. US WorldMeds, LLC. March 2017.
Comtan. Prescribing Information. Orion Corporation. September 28, 2010.
Tasmar. Prescribing Information. Valeant Pharmaceuticals North America, LLC. May 2013.
Ogentys. Prescribing Information. BIAL-Portela & Ca , S.A. April 2020.
Benztropine. Prescribing Information. Major Pharmaceuticals. January 2025.
Trihexphenidyl. Prescribing Information. Natoc Pharma Limited. October 2019.
Trihexphenidyl oral solution. Prescribing Information. Pharmaceutical Associates, Inc. 2025.
Radder DLM, Lígia Silva de Lima A, Domingos J, et al. Physiotherapy in Parkinson's Disease: A Meta-Analysis of Present Treatment
Modalities. Neurorehabil Neural Repair. 2020;34(10):871-880. doi:10.1177/1545968320952799
Osborne JA, Botkin R, Colon-Semenza C, et al. Physical Therapist Management of Parkinson Disease: A Clinical Practice Guideline From the American Physical Therapy Association [published correction appears in Phys Ther. 2022 Aug 1;102(8):pzac098. doi: 10.1093/ptj/pzac098]. Phys Ther. 2022;102(4):pzab302. doi:10.1093/ptj/pzab302
Parkinson’s Foundation. Parkinson’s Exercise Recommendations. Parkinso.org. Undated. Accessed January 29, 2025. https://www.parkinson.org/library/fact-sheets/exercise- recommendations
Tofani M, Ranieri A, Fabbrini G, et al. Efficacy of Occupational Therapy Interventions on Quality of Life in Patients with Parkinson's Disease: A Systematic Review and Meta-Analysis. Mov Disord Clin Pract. 2020;7(8):891-901. Published 2020 Oct 2. doi:10.1002/mdc3.13089
Xu H, Bao Z, Liang D, et al. Speech and Language Therapy for Voice Problems in Parkinson's Disease: A Meta-Analysis. J Neuropsychiatry Clin Neurosci. 2020;32(4):344-351. doi:10.1176/appi.neuropsych.19020044
Gandhi P, Steele CM. Effectiveness of Interventions for Dysphagia in Parkinson Disease: A Systematic Review. Am J Speech Lang Pathol. 2022;31(1):463-485. doi:10.1044/2021_AJSLP-21-00145
Rees J, Ryan J, Laws M, Devine A. A comprehensive examination of the evidence for whole of diet patterns in Parkinson's disease: a scoping review. Nutr Neurosci. 2024;27(6):547-565. doi:10.1080/1028415X.2023.2233727
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2025: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.