MANAGING PATIENT OUTCOMES WITH DEPRESCRIBING
Pamela Sardo, PharmD, B.S.
Pamela Sardo, PharmD, B.S. is a freelance medical writer and currently licensed pharmacist in 3 states. She is the founder and principal at Sardo Solutions in Texas. Pam received her B.S. from the University of Connecticut and her Pharm.D. from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Topic Overview
Deprescribing is a top priority in patient safety and is a component of effective prescribing practices. It is one of the processes that can address harmful polypharmacy. Deprescribing is the planned and supervised process of reducing doses or stopping medication that might cause harm or no longer be needed. It is fundamentally patient-centered. Deprescribing can prevent or correct medication complications, improve outcomes, and reduce costs.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-071-H01-P
Pharmacy Technician 0669-0000-23-072-H01-T
Credits: 1 hour of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $4.99
Estimated time to complete activity: 1 hour, including Course Test and course evaluation
Release Date: May 13, 2023 Expiration Date: May 13, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From May 13, 2023, through May 13, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Identify what deprescribing means in healthcare
Describe common therapeutics to consider in patient-centered deprescribing
Recall 2 goals of deprescribing
Identify deprescribing tools or resources to implement deprescribing
Disclosures
The following individuals were involved in developing this activity: Pamela Sardo, PharmD, BS. Pamela Sardo, Pharm.D., B.S., was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Deprescribing can identify patient medications that may be or should be discontinued. There are barriers to deprescribing that clinicians should know so they may overcome them. When these barriers are eliminated, deprescribing can improve a patient’s healthcare outcomes and address the potentially harmful aspects of polypharmacy. Deprescribing is applicable to all populations but is particularly relevant for older adults with cardiovascular disease. Monitoring patients’ active medication lists and deprescribing any unnecessary medications is recommended to reduce pill burden, reduce the risks of adverse drug events, and minimize financial hardship. Deprescribing is best accomplished within the context of a multidisciplinary approach, where various healthcare professionals may collaborate to determine the best treatment plan for the patient.
Polypharmacy and its Impact
Polypharmacy refers to the condition of taking multiple medications, usually defined as five or more medications; however, there is no single agreed- upon definition. Polypharmacy can be helpful or harmful. Medication overload is a type of polypharmacy and is defined as the use of multiple medications for which the harm to the patient outweighs the benefit.1
Over the next decade, it is forecasted that medication overload will cause the premature deaths of at least 150,000 older people in the U.S., reducing the quality of life for millions more.1 Prescribing inappropriate or unnecessary medications is also costly. Reducing inappropriate or unnecessary medications could save at least $60 billion over the next decade in unnecessary hospitalization for older adults alone.1
A prescribing cascade can contribute to polypharmacy. A prescribing cascade describes a sequence of events that begins when an adverse drug event (ADE) occurs, is misinterpreted as a new medical condition, and a subsequent drug is then prescribed to treat the ‘new condition.’2 A prescribing cascade can be appropriate or problematic, and the ADEs can be recognized or unrecognized.2 Understanding how prescribing cascades develop and identifying
strategies for their identification, prevention, and management can improve patient care.3 Deprescribing may be part of that management.
Patients and healthcare providers struggle to recognize prescribing cascades and to identify when they occur.3 Strategies that narrow knowledge gaps and equip patients and clinicians with resources to recognize prescribing cascades are needed.3 At least one pharmacy school incorporates prescribing cascade knowledge into its curriculum through a game-based recognition activity.4
The U.S. has had limited success addressing medication overload and is lagging behind other countries in addressing medication overload.5 Canada and Australia have established “deprescribing networks” of researchers, clinicians, pharmacists, and patient advocates who create strategies, share information, and report on interventions to help clinicians stop or pause potentially dangerous or unnecessary medications.5 Pharmacy team members have an opportunity to reduce medication overload. This begins with a move away from the culture of “more is better” in medicine.1 This change in culture can be accomplished in part through deprescribing.
Judicious prescribing and judicious deprescribing are important.6 Deprescribing is a top priority in patient safety and is a component of effective prescribing practices. Clinicians should determine whether medications are currently necessary and, if not, whether a deprescribing trial is reasonable.
What is Deprescribing?
There are many definitions for deprescribing. One definition describes it as a process to identify and discontinue medications when existing or potential harms outweigh poten-tial patient care benefits. Deprescribing is fundamentally patient-centered. This means that a patient’s response or reaction to each drug, life expectancy, values, and preferences must also be included in evaluating deprescribing.7
Deprescribing involves discontinuing medications, decreasing medication dosages, and changing medications to optimize clinical outcomes.7 Approaches to deprescribing should be focused, and patient-specific, considering variable patient characteristics and specific medications.6 Clinical practice guidelines often discuss how to initiate therapies but rarely discuss when and how to discontinue them.6 Deprescribing can prevent or correct medication complications, improve outcomes, and reduce costs.
It is prudent to review medications in diverse populations, such as the seriously ill and frail elderly, and consider deprescribing inappropriate medications. Studies have suggested that deprescribing leads to improvement in cognition, fewer falls, and improved survival.8
Barriers to Deprescribing
There are various barriers to deprescribing. Knowledge gaps, an absence of an interdisciplinary approach, patient resistance, time constraints, a lack of patient support, and other factors may prevent deprescribing.
Knowledge Gaps
Prescribing cascades develop due to inconsistent awareness of medications; diverse feelings of accountability for medication decision-making; and variable accessibility to relevant information.3 Patients and healthcare providers struggle to recognize prescribing cascades. Knowledge gaps contribute to this challenge and lead to inaction.
In one study, 14 participants were interviewed.3 Very few of those interviewed could state specific medication goals. Some participants were able to recall names and reasons for use. Many could not recall when medications were started or the order in which they were prescribed.3 Some participants lacked awareness of the usual duration of medication use and some were unaware of alternative potential non-pharmacologic options for their conditions.3
Absence of an Interdisciplinary Approach
Physicians reported that when a pharmacist was not present to screen patients for possible prescribing cascades, they found it difficult to do so independently.3 This was partly due to a lack of awareness of prescribing cascades and an assessment process learned in medical school focusing on treating symptoms more than considering drug-induced symptoms.3
Patient Resistance
Patients may be reluctant to discontinue medications, even when presented with evidence that the medications are not beneficial and may cause harm and financial distress.6 Patients taking chronic medications may worry about worsening conditions and resist discontinuing medications despite new guidelines. One example is that the use of opioids with benzodiazepines is now discouraged.6
Patients taking medications prescribed by previous physicians may not wish to question the historical care plan by stopping their medications. Medication prescribing between patients and providers is based on trust and mutual goals of improved patient health. Deprescribing may raise patients’ concerns that the healthcare team is “giving up” on them.9 Therefore, it is critical to ensure that this process is framed in a positive manner.9
Time Constraints
Other barriers include time constraints. Pharmacies are often fast-paced work environments and are under time pressure. For example, a prescriber can feel pressured to address multiple issues in one visit and may not have enough time to deprescribe with shared decision-making discussions.6 In addition, patients may put pressure on healthcare providers when requesting medications, despite unclear benefits.6 Another barrier is that clinical practice guidelines strive to optimize disease management but rarely address patients with complex comorbidities.9
A Lack of Patient Support
Deprescribing may be hindered if social support is absent, which may lead to the patient being confused about changes in prescribing.3 Communicating a change in prescribing plans to patients is crucial. Otherwise, patients requesting discontinued medications may be confused, resulting in delayed deprescribing.
Other Factors
Additional barriers to deprescribing are automated refills.6 Some employers reward employees based on the total or increased sales. That creates a possible disincentive to deprescribe. Another factor is that the patient may request refills of discontinued medications.
Targets for Deprescribing
Deprescribing applies to all populations but is particularly relevant for older adults with cardiovascular disease.9 Concomitant geriatric conditions such as polypharmacy, frailty, and cognitive dysfunction are also relevant to consider.9 A trigger to consider deprescribing includes the presentation, or risk, of adverse drug reactions. Considerations also include unnecessary polypharmacy, and the need to align medications with goals of care when life expectancy is reduced.9
Targets for deprescribing include older adults with multiple subspecialist physicians and no primary care physician. Vulnerable adults in long-term care facilities are also at risk because they are more frail than community-dwelling populations. Up to 91% of patients in long-term care take at least five medications daily.6
Younger adults with chronic pain, such as fibromyalgia or developmental disabilities, should be assessed for deprescribing opportunities.10 Younger adults with mental health conditions are also often prescribed psychotropic medications with adverse effects, and more medications may be added to miti-gate side effect profiles.10
Within a healthcare system, poor medical record keeping can lead to polypharmacy and the opportunity for judicious deprescribing.6 One published study revealed another finding in patients with diabetes.11 Complex medication regimens were associated with less optimal type 2 diabetes outcomes. It concluded that the more complex medication regimens were associated with worse hemoglobin A1c.11
Deprescribing should be considered a therapeutic intervention, just like starting a new treatment.6 When deprescribing, it is imperative to consider patient/caregiver perspectives on the goals of therapy.6 This includes discussing views on medications, chronic conditions, preferences, and priorities.6 Pharmacy teams and nurses12 are optimally positioned to engage in targeted discussions and shared decision-making regarding slowing disease progression, preventing health decline, and addressing symptoms.
Deprescribing Goals and the Patient-Centered Approach
Monitoring patients’ active medication lists and deprescribing unnecessary medications is recommended to reduce pill burden, reduce the risks of adverse drug events, and minimize financial hardship.6 Point-of-care tools and resources can aid healthcare providers in deprescribing, if appropriate, and help patients understand the need to decrease medication burden and reduce risks.6
Clinical goals for deprescribing include:6-7,12
Identify and prioritize medications to discontinue and discuss potential deprescribing with the healthcare team, prescribers, and patients
Determine whether there are medications without current and valid indications
Determine if duplicate therapy is present
Determine if appropriate dosing is present
Evaluate whether drug-drug or drug-disease interactions exist
Prioritize deprescribing to the treatments with the lowest benefit-to- harm ratio
Prioritize deprescribing to the lowest likelihood of withdrawal reactions or disease rebound syndromes
Always develop a follow-up plan with the patient when deprescribing
Once a deprescribing plan is initiated, consider it at each visit and during health maintenance visits
Consider nonpharmacologic treatments when appropriate
Consider a new medication as a trial, rather than permanent
Goals for deprescribing are more likely to be accomplished if consideration is given to patient-centered approaches.13-15 Patient-centered “multimodal deprescribing,” provides better clinical outcomes than uniform deprescribing.13 Multimodal deprescribing involves shared decision-making that includes the healthcare team, the patient, and possibly family members or caregivers, whereas uniform deprescribing is more of a top-down approach that does not engage the interdisciplinary team or patient as much. Therefore, clinicians should engage in a shared decision-making process, which is an effective deprescribing method.13
The development of the clinician-patient relationship facilitates patient- centered care.14 This improves rapport and builds trust. A patient-centered approach happens when communication is improved between the clinician and the patient.14 “The clinician must promote an open environment that is conducive” to patient-centered care.14 The clinician should discuss the patient’s treatment options and their respective risks and benefits with the patient, and this information should be conveyed in an understandable way.14 This allows patients to understand their healthcare plan and give “informed” consent.14,15
Factors a clinician would want to consider in patient-centered care include the patient’s cost, convenience, side effects, lack of efficacy, poor compliance, life expectancy, and preferences.15 It is important that the patient is willing to deprescribe. In some cases, the patient may not want to deprescribe over concerns of worsening symptoms.15 The clinician’s goal should be to identify opportunities for deprescribing that are supported by clinical evidence and are in line with the patient’s preferences.15
Frequent Therapeutic Classes of Medications in Deprescribing
Certain drugs are more likely to be inappropriately prescribed. In one study, potentially inappropriate medications were screened in 26 patients with a diagnosis of cancer.16 The mean number of medications was 12 in each patient. After assessment and discussions with prescribers, deprescribing was accomplished in 73% of potentially inappropriate medications.16 Approximately two-thirds of the patients reported a reduction in symptoms after the deprescribing intervention. Healthcare expenditures of $4282.27 per patient were potentially avoided as a result of deprescribing.16
Deprescribing in this study included:16
Vitamins and minerals due to pill burden and drug interactions
Antihypertensives due to fatigue, orthostatic hypotension, falls
Statins due to lack of benefit, myalgias, fatigue
Benzodiazepines due to CNS depression, falls
Aspirin/NSAIDS due to gastrointestinal bleeds
Proton pump inhibitors due to chronic kidney disease, hypocalcemia
Omega 3 fatty acids due to ↑ bleeding risk, pill burden
Physician and pharmacist-led medication reviews can make a difference in patient care. One publication discussed an ambulatory program to optimize the health and quality of life of frail, community-dwelling older people (aged 65 and over) referred by other physicians.3 The referral addressed two or more concerns with mobility or falls, activities of daily living, cognition, function, medication, and future planning/caregiver stress.3 Patients attended twice weekly, over 8-
10 weeks, for assessment and personalized interdisciplinary team care.3 This ambulatory site was chosen as the setting because comprehensive pharmacist physician-led medication reviews frequently resulted in prescribing cascades being identified, managed, and/or resolved.3
This was a very intensive intervention, and twice-a-week visits over many weeks - in the real world of patient care - are not generally feasible. The baseline findings and results are significant and may provide opportunities in a busy practice setting.
In this study, at the baseline, the following prescribing cascades were observed:3
Cholinesterase inhibitors (ChI), such as donepezil or rivastigmine, were prescribed, urinary incontinence was identified (a possible side effect of ChI), and anticholinergic medication, such as oxybutynin, was prescribed
NSAIDs, such as naproxyn, were prescribed, hypertension was identified (a possible side effect of NSAIDs), and antihypertensives were prescribed
Thiazide diuretics, such as chlorthalidone, were prescribed, gout (a possible side effect of thiazide diuretics) was identified, and anti-gout medication was prescribed
Gabapentin was prescribed, peripheral edema (a possible side effect of gabapentin) was identified, and diuretics were prescribed
In the study, the baseline findings served as a basis for patient interviews, and additional prescribing cascade cases warranting assessment were identified:3
Amlodipine was prescribed. Ankle swelling was seen, so furosemide was prescribed, leading to urinary frequency, so tamsulosin was prescribed
Diltiazem was prescribed. Ankle swelling was seen, so chlorthalidone was prescribed, leading to hyperglycemia, so glyburide was prescribed
Hyperglycemia was identified while prednisone treatment was underway, so glyburide was prescribed
After naproxen was prescribed, pantoprazole was prescribed for protection against possible stomach ulcer, then vitamin B-12 was prescribed because pantoprazole ↓ B12 absorption
After paroxetine was taken for years, levodopa was added for Parkinson’s symptoms. Lisinopril was added due to observed ↑ blood pressure (BP). Paroxetine can cause both tremors and ↑ BP
Palliative care is another important condition for deprescribing. A discussion of deprescribing should be routine in older adults with cardiovascular disease (CVD) and an anticipated life expectancy of less than 2 years.9 Comorbid conditions, frailty, or cognitive impairment in addition to CVD should trigger a deprescribing conversation, even if the life expectancy is over 2 years.9 Deprescribing conversations in these late-in-life cases should focus on symptom management, reducing adverse events and treatment burden. Table 1 lists some potential medications for deprescribing. This is not a complete list, but it provides examples for review and consideration.
Table 1: Potentially Inappropriate Medications in Older Adults9
| Risk of Exacerbation of Condition | Medications |
| May exacerbate heart failure | Flecainide Disopyramide Thiazolidinediones Calcium channel blockers TNF-α inhibitors |
| May raise blood pressure | Antidepressants Antipsychotics Decongestants Systemic corticosteroids NSAIDs |
| May raise the risk of syncope, falls, fractures | Anticonvulsants Hypnotics Olanzapine Opioids Terazosin |
| May raise delirium, dementia | Anticholinergics Antipsychotics Benzodiazepines Corticosteroids H2 receptor antagonists |
| May raise GI bleed, renal insufficiency | Aspirin >325 mg/day Non-COX NSAIDs |
TNF – tumor necrosis factor; NSAID – nonsteroidal anti-inflammatory; mg – milligram
COX- cyclooxygenase
If a patient’s treatment involves a complex regimen, or if the medication is potentially inappropriate or lacks an indication, then shared decision-making regarding deprescribing may be appropriate.17 If a medication fails to provide additional benefit, lacks efficacy, or causes an adverse reaction, consider shared decision-making with the provider and patient to implement deprescribing tapering or discontinuing the medication.17
One study enrolled 61 participants with a mean age of 79.6 years who took an average of 11.5 medications.18 The team recommended 263 medication changes.18 The team’s recommendations resulted in the discontinuation of 162 medications and dose changes for 48 medications.18
Tools that help identify potentially inappropriate medication use include Beer’s Criteria, STOPP (Screening Tool of Older Persons' Prescriptions).6 Additional tools include START (screening tool to alert to the right treatment) criteria, and the Medication Appropriateness Index (MAI).6 These and other tools have benefits and provide a specific approach to medication management. No one tool or strategy was shown to be superior in improving patient-related outcomes. Figure 1 below provides a simplified approach to the steps for deprescribing.
Every time a patient encounters the pharmacy team is an opportunity to reduce unnecessary medications. Drug-disease interactions may contribute to adverse events. Geriatric syndromes, or youth-onset chronic diseases, may contribute to polypharmacy and opportunities to reduce medication overload.
Figure 1: Deprescribing Algorithm Option7,16
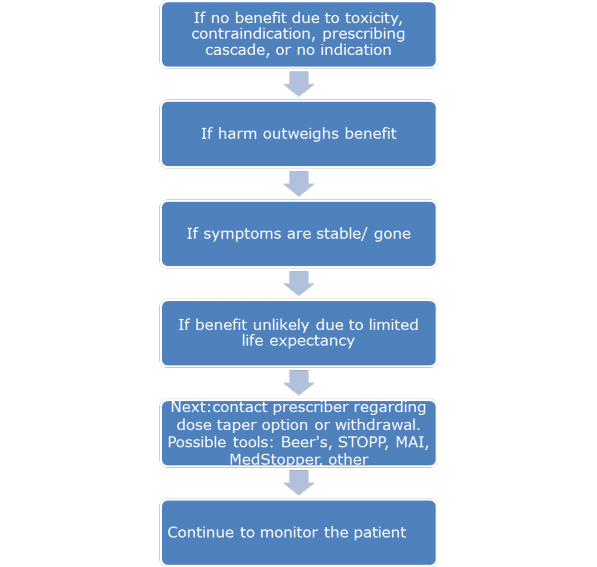
STOPP – Screening tool of older persons’ prescriptions
MAI – Medication appropriateness index
Workplace computer alert systems are becoming more sophisticated to catch some duplicate therapy and other issues. When consumers receive medications from multiple sources, it is helpful to have the patients bring all their medications in a bag for review, referred to as a brown bag review. Some evidence-based tools to guide staff on appropriate medication use are in Table 2.
Table 2: Tools to Assist Medication Appropriateness or Deprescribing
| Description | Resource |
| Medication Appropriateness calculator provides questions and a point system | https://globalrph.com/medcalcs/medication- appropriateness/ |
Deprescribing.org IAM Medical Guidelines (Apple and Google Play) | https://deprescribing.org/deprescribing- mobile-app-iam-medical-guidelines/ |
| Deprescribing.org Deprescribing guidelines and algorithms | https://deprescribing.org/resources/deprescri bing-guidelines-algorithms/
https://www.deprescribingnetwork.ca/algorit hms |
| Medication-free options (with patient brochures) | https://deprescribing.org/resources/deprescri bing-information-pamphlets/ |
| Deprescribing.org Deprescribing pamphlets | https://deprescribing.org/resources/deprescri bing-information-pamphlets/ |
| Anticholinergic Burden Calculator | http://anticholinergicscales.es/calculate or https://www.acbcalc.com/ |
| Beers List of medications with highest risk to older patients | https://geriatricscareonline.org/ProductAbstr act/2023-ags-beers-criteria- pocketcard/PC0015/ |
| MedStopper to enter drug list and receive recommendations | http://medstopper.com/ |
| Choosing Wisely (with English/Spanish patient resources) | https://www.choosingwisely.org/ |
When implementing deprescribing, the pharmacy team members are optimally positioned to discuss this topic with patients. Discussion includes asking probing questions and teach-back. The teach-back method involves asking patients to re-state in their words, and in a gentle, respectful manner, what the provider discussed with them. Teach-back can also uncover what they need to know or do. This recall ensures that the patients understand the healthcare team’s discussion and goals of care. Probes and teach-back could include the patient restating the indications for prescribed medications or when did a patient begin to experience symptom(s) that bothered them? The patient can be asked what symptom(s) were like and what they did about it.
Pharmacy staff are often busy and understaffed. A pharmacist, or pharmacy technician, asking just one question may uncover opportunities to optimize medication regimens. Uncovering medication overload requires a delicate manner and sensitivity to the situation and the consumer. The approach differs based on your practice setting, space for privacy during patient dialog, patient status, patient personality, and many other factors. Open-ended questions uncover more information than yes/no questions. Examples of open- ended questions suggested by researchers are as follows:3
Do you have any questions for the pharmacist about any medication?
How do you feel about the medications you are taking?
How do you feel about the number and types of medication you take?
How do you like to learn about your medication?
Who usually does the teaching about your medications?
I want to make sure you have all the information that you need. What did the doctor tell you this is for?
What instructions did you receive about the length of time you will be taking this?
How do you get all of your questions answered about your medication?
How did your recent new medicine help (or not help) with symptoms that were bothering you?
Have you experienced any symptoms that bother you?
With these questions, and the exchange that can naturally follow, a clinician can make positive progress in implementing deprescribing. the pharmacy team members are optimally positioned to discuss this topic with patients. This promotes a patient-centered healthcare approach, which leads to better patient outcomes.
Summary
Drug therapy aims to prevent, delay, or treat disease, improve quality of life, optimize outcomes, and increase longevity where possible. Deprescribing is a critical component of good prescribing practice. It is fundamentally patient- centered. The prescriber and pharmacy teams must discuss with patients to set shared goals for each medication and the patient's comorbidities. The healthcare team should review each medication's risks, side effects, and the potential impact on the patient if a medication is stopped.
Pharmacy teams are ideally positioned to lead or contribute to deprescribing interventions. The healthcare team can reassure patients that deprescribing medications is evidence-based, beneficial, and may lead to improved patient outcomes and cost savings.
References
Garber, J, Brownlee S. Medication Overload: America's Other Drug Problem. The Lown Institute. Updated 2019 doi:https://doi.org/10.46241/LI.WOUK3548. Accessed April 19, 2023.
McCarthy LM, Visentin JD, Rochon PA. Assessing the Scope and Appropriateness of Prescribing Cascades. J Am Geriatr Soc. 2019;67(5):1023-1026. doi: 10.1111/jgs.15800
Farrell, B.J., Jeffs, L., Irving, H. et al. Patient and provider perspectives on the development and resolution of prescribing cascades: a qualitative study. BMC Geriatr. 2020;20:368.
Testman JA. The prescribing cascades game: applying geriatric pharmacotherapy principles in the classroom. Curr Pharm Teach Learn. 2014;6(5):646-651.
Tannenbaum C, Farrell B, Shaw J, et al. An Ecological Approach to Reducing Potentially Inappropriate Medication Use: Canadian Deprescribing Network. Can J Aging. 2017;36(1):97-107. doi: 10.1017/S0714980816000702
Halli-Tierney AD, Scarbrough C, Carroll D. Polypharmacy: Evaluating Risks and Deprescribing. Am Fam Physician. 2019;100(1):32-38.
Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med. 2015;175(5): 827-834.
Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82(3):583-623. doi: 10.1111/bcp.12975
Krishnaswami A, Steinman MA, Goyal P, et al; Geriatric Cardiology Section Leadership Council, American College of Cardiology. Deprescribing in Older Adults With Cardiovascular Disease. J Am Coll Cardiol. 2019;73(20):2584-2595. doi: 10.1016/j.jacc.2019.03.467
Lunsky Y, Modi M. Predictors of Psychotropic Polypharmacy Among Outpatients With Psychiatric Disorders and Intellectual Disability. Psychiatr Serv. 2018;69(2):242-246. doi: 10.1176/appi.ps.201700032
Russell AM, Opsasnick L, Yoon E, Bailey SC, O'Brien M, Wolf MS. Association between medication regimen complexity and glycemic control among patients with type 2 diabetes. J Am Pharm Assoc.(2003). 2022:S1544-3191(22)00458-7. doi: 10.1016/j.japh.2022.12.028
Brandt NJ. Optimizing Medication Use Through Deprescribing: Tactics for This Approach. J Gerontol Nurs. 2016 Jan;42(1):10-4. doi: 10.3928/00989134-20151218-08
Ie K, Machino R, Albert SM, et al. Deprescribing as an Opportunity to Facilitate Patient-Centered Care: A Qualitative Study of General Practitioners and Pharmacists in Japan. Int J Environ Res Public Health. 2023;20(4):3543. Published 2023 Feb 17. doi:10.3390/ijerph20043543
Smith H, Miller K, Barnett N, et al. Person-Centred Care Including Deprescribing for Older People. Pharmacy (Basel). 2019;7(3):101. Published 2019 Jul 25. doi:10.3390/pharmacy7030101
Vasilevskis EE, Shah AS, Hollingsworth EK, et al. A patient-centered deprescribing intervention for hospitalized older patients with polypharmacy: rationale and design of the Shed-MEDS randomized controlled trial. BMC Health Serv Res. 2019;19(1):165. Published 2019 Mar 14. doi:10.1186/s12913-019-3995-3
Whitman A, DeGregory K, Morris A, Mohile S, Ramsdale E. Pharmacist-led medication assessment and deprescribing intervention for older adults with cancer and polypharmacy: a pilot study. Support Care Cancer. 2018;26(12):4105-4113. doi: 10.1007/s00520-018-4281-3
McGrath K, Hajjar ER, Kumar C, Hwang C, Salzman B. Deprescribing: A simple method for reducing polypharmacy. J Fam Pract. 2017;66(7):436- 445.
Whitty R, Porter S, Battu K, et al. A pilot study of a Medication Rationalization (MERA) intervention. CMAJ Open. 2018;6(1):E87-E94. doi: 10.9778/cmajo.20170134
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.