NAVIGATING NEPHROLITHIASIS: INSIGHTS AND INTERVENTIONS IN KIDNEY STONE MANAGEMENT
L. Austin Fredrickson, MD, FACP
Dr. Fredrickson is an Assistant Professor of Internal Medicine at the Northeast Ohio Medical University College of Medicine, where he serves as a course director and core teaching faculty. He is board-certified in Internal Medicine and is a practicing general internist.
Topic Overview
Renal calculi, commonly referred to as kidney stones, are ubiquitous and persistent causing significant duress and pain, missed work and decreased productivity, and increased utilization of healthcare resources. Despite well- documented approaches to diagnosis and management of kidney stone disease (urolithiasis), including tested methods of prevention, this remains a common malady affecting many patients. Recent literature further underscores the discrepancies in evaluation and treatment based on socioeconomic status and race. With increasing prevalence and diverse etiologies, a thorough and updated understanding of effective management and prevention is warranted for all healthcare professionals and interdisciplinary collaboration.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-212-H01-P
Pharmacy Technician 0669-0000-23-213-H01-T
Credits: 1 contact hour of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $4.99
Estimated time to complete activity: 1 contact hour, including Course Test and course evaluation
Release Date: December 12, 2023 Expiration Date: December 12, 2026
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
How to Earn Credit: From December 12, 2023, through December 12, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Identify risk factors for nephrolithiasis
Describe the process of diagnosing kidney stones
Recall approaches to treating and preventing kidney stones
Disclosures
The following individuals were involved in developing this activity: Austin Fredrickson, MD, FACP, Liz Fredrickson, PharmD, BCPS, and Pamela M. Sardo, PharmD, BS. Pamela M. Sardo was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Renal calculi, commonly referred to as kidney stones, are ubiquitous and persistent causing significant duress and pain, missed work and decreased productivity, and increased utilization of healthcare resources. Despite well- documented approaches to diagnosis and management of kidney stone disease (urolithiasis), including tested methods of prevention, this remains a common malady affecting many patients. Recent literature further underscores the discrepancies in evaluation and treatment based on socioeconomic status and race. With increasing prevalence and diverse etiologies, a thorough and updated understanding of effective management and prevention is warranted for all healthcare professionals. The dynamic landscape of stone formation, diagnosis, treatment, and prevention is ever- evolving, promoting the importance of continuing education and interdisciplinary collaboration. Within this course, healthcare personnel will learn how to identify risk factors for nephrolithiasis, describe the process of diagnosing kidney stones, and understand approaches to treating and preventing kidney stones.
Terminology
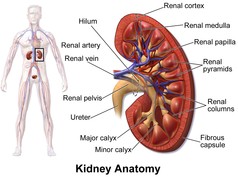
Urolithiasis and nephrolithiasis are terms often used interchangeably but technically refer to distinct aspects of urinary stone disease.1 Nephrolithiasis specifically pertains to the formation and presence of stones within the kidneys, encompassing the intricate process of stone development within the renal parenchyma and renal collecting system, which can be viewed in Figure 1 below.2 Urolithiasis is a broader definition, encompassing not only nephrolithiasis but also the formation or occurrence of urinary stones throughout the entire urinary tract, including the ureters and bladder.1 It is important to differentiate between these terms, as they inform clinical management and treatment approaches. Nephrolithiasis often requires specific interventions for stones lodged within the kidneys, and urolithiasis encompasses a more comprehensive evaluation and management of stones throughout the urinary system, often collecting in the bladder itself.1 Most stones still arise from the kidney or ‘start’ as nephrolithiasis but migrate into
other areas. Colloquially, “kidney stones”, known medically as “renal calculi”, comprise true nephrolithiasis but generally any urolithiasis, even if lodged in the bladder or a “bladder stone”.1 For example, a bladder stone may be removed with cystoscopic retrieval, whereas a stone wedged in the kidney itself may require lithotripsy or stent insertion more proximally to the bladder.
Figure 1 Kidney Anatomy
Epidemiology and Etiology
There are various types of kidney stones, and the type of stone identified will inform a patient’s prognosis, treatment, and preventive care regimen.3 Stones can be a mix of different crystal types, for example, a combination of calcium oxalate and calcium phosphate.3 Stones can also be made up of medications, such as acyclovir, though this is rare. Types of kidney stones are listed in Table 1. Figure 2 visually depicts a kidney stone.4
The prevalence of urolithiasis varies globally, with rates estimated between 1-13%.5 The incidence of urolithiasis within the United States (US) has increased in recent years, with an estimated lifetime risk of 10-15%.6 Numerous factors contribute to this rise, including dietary habits, increased body mass index, comorbidities, climate change, and socio-economic conditions.3,5 Recent data suggest approximately 19% of men and 9% of women will develop a kidney stone at least once in their lifetime.3 For men,
the peak incidence occurs around 40 years of age and then starts to decrease.3 For women, the peak incidence occurs at 30 years of age.3
Table 1
Types of Kidney Stones3
| Stone Type | Percentage |
| Calcium oxalate | 75% |
| Calcium phosphate | 15% |
| Uric acid | 8% |
| Struvite | 1% |
| Cystine | <1% |
Figure 2 Kidney Stone4

The disease prevalence among Hispanics (6.4%) and blacks (4.3%) has been estimated to be lower than among non-Hispanic whites. Yet, minority patients have been found to have poorer quality of life, delays in diagnosis and treatment, and greater incidence of disease recurrence.7 As an example, studies have shown that African American patients receive poorer analgesic care compared to white patients; one study found African American patients received less analgesia when presenting with nephrolithiasis compared to white patients.8
In addition to causing disease-related complications and issues for patients, nephrolithiasis is also associated with a significant economic burden for patients due to loss of work and costs related to treatments and surgeries.3 These issues and discrepancies described above also occur for patients with lower socio-economic status.3
Pathophysiology and Risk Factors
The pathophysiology of stone formation is important to effective treatment and management. Understanding the pathophysiology of stone formation also helps the clinician identify risk factors for nephrolithiasis.
Pathophysiology
The pathophysiology of nephrolithiasis requires an understanding of the complex solution called urine. It is often supersaturated with one or more kinds of chemicals or crystals.3 Stones are prevented from forming via the presence of crystallization inhibitors, most notably urine citrate.3 Citrate is able to reduce the supersaturation of urine with calcium salts by binding with calcium and inhibiting calcium crystal growth.9 Citrate is also able to increase the activity of macromolecules that inhibit the aggregation of calcium oxalate.9
Kidney stone formation occurs due to the deposition of calcium phosphate at the thin limb of the loop of Henle (the medullary component that connects the proximal and distal tubules) within the kidney.3 This deposition continues and eventually erodes through the papillary epithelium, which
allows for the deposition of calcium oxalate and calcium phosphate crystals.3 It has been hypothesized that kidney stone formation can start even years before a stone is clinically detected, not unlike atherosclerosis predating acute coronary thrombosis.3
Risk Factors
The risk factors for nephrolithiasis can be grouped into four broad categories: dietary, nondietary, urinary, and genetic.3 Diet can play an important role in both the generation and recurrence of kidney stones, with many factors involved in the pathophysiology of nephrolithiasis affected by diet.3 Dietary factors associated with an increased risk of nephrolithiasis include animal protein, oxalate, sodium, sucrose, and fructose intake.3 Intake of calcium, potassium, and phytate are associated with a decreased risk of developing nephrolithiasis.3 Increases in dietary calcium may lead to a reduction in risk due to a reduction in the intestinal absorption of dietary oxalate, which leads to a decrease in urine oxalate and, thus, a decreased risk of calcium oxalate stones.3 A summary of dietary factors is presented in Table 2.
Table 2
Dietary factors and risk of kidney stone development3
| Dietary Factor | Modification | Potential Stone Risk |
| Fluid intake | Reduction | Increased urine saturation / concentration |
| Sodium intake | Increase | Increased urine calcium and reduced citrate expression |
| Calcium intake | Reduction | Increased urinary oxalate excretion |
| Meat intake | Increase | Low urine pH, increased urine calcium, reduced citrate excretion |
| Diet content in oxalate foods | Increase | Increased urinary oxalate excretion |
Risk factors that are non-dietary in nature include age, race, body size, medication use, and the environment.3 While nephrolithiasis can occur in patients as young as infants and in the elderly population, it is most common among middle-aged white men.3 Regarding geographic prevalence, kidney stone development is most common within the southeastern region of the US.3 Kidney stone development is also associated with weight gain, and the increase in nephrolithiasis has mirrored the increase in obesity rates within the US.3 Environmental risk factors include those that lead to decreased urine volume, such as lack of water or bathroom access.3 Numerous medications are associated with an increased risk of kidney stone formation. These are listed in Table 3.3
Table 3
Medications Associated with Kidney Stone Formation
| Type of medication | Examples |
| Antibiotics | Ampicillin, amoxicillin, ceftriaxone, sulfonamides |
| Carbonic anhydrase inhibitors | Acetazolamide, topiramate |
| Diuretics | Furosemide, triamterene |
| Laxatives | Overuse of any laxative that results in electrolyte loss |
| Potassium channel blockers | Amiodarone, dalfampridine, sotalol, |
| Reverse transcriptase inhibitors and protease inhibitors | Efavirenz, indinavir, nelfinavir, raltegravir |
| Sulfonylureas | Therapies for type 2 diabetes |
| Others | Aluminum magnesium hydroxide, ascorbic acid, calcium, dexamethasone, guaifenesin, phenytoin, vitamin D |
Generally, all these medications either promote crystallization in the urine, alter urinary chemistry, decrease the solubility of minerals, dehydrate the body, or promote urinary stasis.3 Still, these can be reviewed in brief highlights here:3
Antibiotics can increase the risk of crystal deposition, including through increased urine concentration.
Carbonic anhydrase inhibitors can lead to metabolic acidosis by excreting more bicarbonate. This can increase the excretion of calcium and uric acid in the urine.
Diuretics cause dehydration and increase concentration, as do laxatives.
Potassium channel blockers’ effect on electrolyte homeostasis can predispose to stones.
Certain antiviral medications also lead to metabolic changes that increase risk.
Sulfonylureas increase the risk of obesity and insulin resistance, both of which can increase the risk of calculi.
Other medications that affect urine composition (namely calcium or uric acid) or other metabolic disturbances can affect stone formation.
Urinary risk factors also contribute to the development of kidney stones.3 One major urinary risk factor is the low urine volume.3 This is considered a modifiable risk factor, with studies highlighting the utility of increasing fluid intake to reduce the risk of nephrolithiasis.3 The pH of urine can also affect the solubility of different types of crystals.3 For example, uric acid stones can only form at a pH <5.5 and calcium phosphate stones at a pH
>/6.5.3 Calcium oxalate stone development is not affected by urinary pH. The remaining urinary risk factors are summarized in Table 4.
| Risk Factor | Description |
| Urine calcium | Higher urinary calcium excretion increases the risk of calcium oxalate and calcium phosphate stones |
| Urine oxalate | Higher urine oxalate excretion increases risk of calcium oxalate stone formation |
| Urine citrate | Lower urine citrate excretion increases the risk of kidney stone formation |
| Urine uric acid | High levels of urine uric acid increase the risk of uric acid stone formation |
Table 4 Urinary Risk Factors3
The final category of risk factors is genetic in nature.3 An individual with a family history of kidney stone development is twice as likely to develop nephrolithiasis as someone without a family history.3 To date, two rare monogenic disorders lead to kidney stone development: primary hyperoxaluria and cystinuria.3 Primary hyperoxaluria is an autosomal recessive disorder that leads to excessive endogenous oxalate being created by the liver.3 This eventually causes calcium oxalate stone formation and deposition.3 Cystinuria is also an autosomal recessive disorder.3 This disorder causes the abnormal reabsorption of filtered basic amino acids. Because cystine is poorly soluble, the excessive urinary cysteine excretion leads to cysteine stone formation.3
Patient Presentation and Diagnosis
The diagnosis and management of kidney stones is summarized in the Kidney Stones: Treatment and Prevention American Family Physician 2019 guidelines.11 Patients with kidney stones may present with various symptoms, including cramping and intermittent abdominal and flank pain.11 Associated symptoms include nausea, vomiting, malaise, fever, and chills.11 If patients have experienced a previous episode of kidney stones, these symptoms can aid the diagnosis.11 Patients generally present with either renal colic or painless gross hematuria when an acute stone event occurs.3 The pain associated with renal colic can vary in intensity and can increase rapidly. 3
To diagnose nephrolithiasis, clinicians should perform a physical examination that excludes the differential diagnosis of conditions listed in Table 5.11 The workup of a patient with suspected kidney stones should include a point-of-care urinalysis to detect hematuria, which can assist in confirming the diagnosis.11
Urine culture and urinalysis can be used to rule out infection.11 Imaging can help confirm the diagnosis and is also used to assess stone size and position. Compared to computed tomography (CT), ultrasonography has been shown to yield an acceptable level of performance and is more cost-effective.11 Thus, this is recommended as a first-line imaging modality for nephrolithiasis.
Because stones frequently do travel down the urinary tract, the entire tract can be visualized with a plain radiograph of the abdomen.11 This x-ray test is commonly called a KUB for kidneys, ureters, and bladder.11 Radiopaque stones (namely those with calcium) can be visualized through this modality.11 However, radiolucent stones (such as uric acid stones) may not be visualizable. A fuller assessment of the soft tissues can be detailed with the CT urogram; however, it also comes with increased radiation and cost.11
Table 5
Differential Diagnosis of Kidney Stones11
| Clinical Clues | Suggested Diagnosis |
| Dysuria | Interstitial cystitis, prostatitis, urinary tract infection, vaginitis |
| Fever, chills | Nonspecific response to infection or inflammation |
| Hematuria | Benign prostatic hyperplasia, renal glomerular disease, urinary tract infection, urinary tumor |
| Nausea, vomiting | Gastrointestinal disease, intestinal or urinary obstruction, nonspecific response to pain |
| Abdominal pain and tenderness | Acute mesenteric ischemia, cholecystitis, gastrointestinal disease |
| Flank pain and tenderness | Dysmenorrhea, herpes zoster, pyelonephritis |
| Urinary frequency | Benign prostatic hyperplasia, bladder spasms, high fluid intake, hyperglycemia, urinary tract infection |
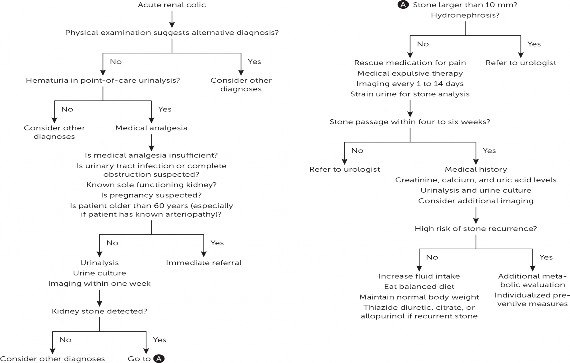
A diagnostic pathway is detailed in Figure 3.11 If a stone is found to be larger than 10mm in size or is causing obstructive features of hydronephrosis or kidney injury, it is generally recommended to refer the patient to a urologist. Smaller stones still may be unable to pass, however, as even stones at 4mm may not be able to pass without intervention.11
Figure 3
Algorithm for the Diagnosis and Management of Acute Kidney Stones11
Approaches to Treatment
The acute management of kidney stones involves appropriately managing the patient’s pain.11 If not contraindicated, it is recommended to utilize nonsteroidal anti-inflammatory drugs over opioids, assuming there is no kidney injury that could be exacerbated, as NSAIDs have greater efficacy and a lower risk of adverse effects.11 Suggested agents include ketorolac at a dose of 30 mg or 60 mg intramuscularly.11 If opioids are utilized, it is recommended to avoid meperidine due to the risk of nausea and vomiting associated with this agent.11 If a patient’s pain is uncontrollable, referral to a urologist or emergency department is recommended.11 Patients should also seek emergency care when sepsis is suspected, if they are anuric, if they have a urinary tract infection with renal obstruction, for women who are pregnant or could possibly be pregnant, and in patients with comorbidities or those greater than 60 years of age.11
If referral to a urologist is unnecessary, patients can be managed conservatively.11 Proper hydration is encouraged. Pain medications should be prescribed as needed, and follow-up imaging should be scheduled within two weeks to determine the stone's position and monitor for hydronephrosis.11 If the stone does not pass on its own, the patient should be referred to a urologist for removal.11 It is estimated that approximately 86% of stones pass spontaneously.12 Medical expulsive therapy can be done to quicken the passage of stones. This involves the use of alpha-blockers (such as tamsulosin or doxazosin).11 It is recommended to offer the use of these medications to patients with stones between 5 and 10 mm in diameter.11 Tamsulosin is the most studied agent in this context. These medications relax the ureteral smooth muscles, which can dilate the ureter and improve stone passage.13 This mechanism can also reduce spasticity and renal colic pain. Clinicians should recognize that increasing fluid intake and use of corticosteroids does not alleviate renal colic or quicken stone passage.11
Clinicians should instruct patients to strain their urine to catch the stone. The stone should be sent in a clean, dry container for stone analysis.11 It is recommended to consider analyzing recurrent stones in case they have different compositions.11 Once the stone composition is known, appropriately targeted preventative measures can be taken to guard against recurrence.11 Creatine, ionized calcium, and uric acid levels should be measured. Parathyroid hormone levels can also be measured if serum calcium levels are high to assess for hyperparathyroidism.11
Special Considerations
Special consideration should be made for asymptomatic kidney stones, children, and pregnant women.
Asymptomatic Kidney Stones
Kidney stones may sometimes be asymptomatic and only found incidentally on imaging.11 Stones can take weeks to months to grow to a clinically detectable size.3 It has been estimated between 10-25% of stones
are symptomatic or require some type of intervention.11 For patients without contraindications, conservative management with active surveillance is appropriate. The patient can be referred for stone removal if issues arise, such as obstruction or recurrent infection.3,11
Children
Due to increasing rates of obesity and diabetes in children, nephrolithiasis is becoming more prevalent in the pediatric population.11 Children who develop kidney stones are more likely to have a metabolic, neurologic, or congenital urinary system structural abnormality.11
Pregnant Women
An estimated 75% of stones in pregnant women are made of calcium phosphate.11 Due to the risk to the fetus, both diagnostic and treatment options are limited in this population.11 In some cases, the development of kidney stones may increase the risk of maternal and fetal complications.11
Prevention
Non-pharmacologic and pharmacologic strategies are available to prevent recurrent kidney stones. The method by which to prevent recurrent stones is dependent on the risk of recurrence. Lifestyle modifications are recommended for those with a low risk of recurrence.11 These include increasing fluid intake to between 2.5 and 3 liters of fluids per day, which aids in achieving a urine-specific gravity of less than 1.010.11 Beverages consumed should be neutral in pH, and carbonated drinks should be avoided.11 In addition to increased fluids, patients should eat a balanced diet high in fiber and vegetables and with a normal consumption of calcium (1-1.2 grams per day).11 Patients should be counseled to limit sodium consumption to 4-5 grams daily and animal protein to 0.8-1 grams per kilogram daily.11 Obese and overweight patients should aim to achieve a normal body weight by increasing physical activity.11
Certain medications and supplements can also be used to prevent recurrent kidney stones. These include thiazide diuretics, allopurinol, and citrate. These agents are typically employed in cases where lifestyle modifications are insufficient to prevent stone recurrence.11 Thiazide diuretics have been shown to be effective at high dosages (50 mg of hydrochlorothiazide per day, 25-50 mg of chlorthalidone per day, and 2.5 mg of indapamide per day).11 Thiazides work by increasing the excretion of sodium and chloride in the urine, which causes the reabsorption of calcium, lowering its urinary concentration.11 They also increase urine volume and increase the concentration of citrate. While lower doses are associated with fewer side effects, their effectiveness is not known.11
Allopurinol is a second pharmacologic option, specifically for patients who have hyperuricemia and/or uric acid stones.11 It is dosed at 100 mg once daily, and the dose can be increased to 100 mg three times daily if needed.11 Allopurinol can reduce uric acid production and help dissolve uric acid crystals that have formed.11 Currently, insufficient evidence suggests that combining allopurinol with either a thiazide diuretic or citrate is more effective than allopurinol monotherapy.11
Supplementation with citrate can be useful for calcium stones, uric acid, and cystine stones.11 Potassium citrate is recommended at a dose of 5 to 12 grams daily.11 The total dose should be divided into three equal doses taken 30 meals before a meal or snack.11 Potassium citrate alkalinizes the urine, preventing stones that form in acidic environments and also inhibits crystal formation by increasing the solubility of stone-forming substances, including calcium and uric acid.11 Potassium citrate use is associated with gastrointestinal symptoms.11 As with allopurinol, there is no evidence that combination therapy with potassium citrate is more beneficial than monotherapy, though the use of potassium citrate with a thiazide diuretic can correct low potassium levels caused by the diuretic.11 As a less expensive option, patients can use unsweetened lemonade to supplement citrate. This can also assist patients with increased fluid intake.11 Citrate can also be taken in by consuming foods that are rich in alkali, such as fruits and vegetables.3 Patients who supplement citrate should have both potassium levels and liver
enzymes monitored. Potassium levels should specifically be monitored within two weeks of starting a supplement and then every 12 months minimally.3
Summary
Kidney stones, medically known as renal calculi, are a prevalent and persistent condition that brings about considerable pain and distress, leading to missed work, reduced productivity, and heightened healthcare resource utilization. Despite established diagnostic and treatment approaches for kidney stones (urolithiasis), including proven preventive measures, this challenge persists. Recent research highlights disparities in evaluation and care based on socioeconomic factors and race. Familiarity with medications and methods to prevent and treat these painful and organ-threatening conditions are imperative. Given the rising prevalence and varied causes of kidney stones, effective management, and prevention require healthcare professionals to have a comprehensive and up-to-date understanding of this ubiquitous condition.
Course Test
Which type of stone is the most common among kidney stones?
Uric acid
Struvite
Calcium
Cystine
What factors have most contributed to the increased incidence of urolithiasis in the United States?
Improved dietary habits and lower body mass index
Decreased comorbidities and stable climate conditions
Dietary habits, increased body mass index, comorbidities, climate change, and socio-economic conditions
Genetic factors and lifestyle changes
Despite a lower disease prevalence among Hispanics and Blacks compared to non-Hispanic Whites, minority patients with nephrolithiasis are more often to experience
better quality of life and faster diagnosis and treatment.
delays in diagnosis and treatment, poorer quality of life, and a higher incidence of disease recurrence.
fewer disease-related complications.
more effective analgesic care compared to White patients.
What is the role of urine citrate in preventing kidney stone formation?
Urine citrate promotes calcium crystal growth.
Urine citrate inhibits the aggregation of calcium oxalate crystals.
Urine citrate increases the supersaturation of urine with calcium salts.
Urine citrate erodes papillary epithelium.
Which of the following dietary factors is associated with an increased risk of developing nephrolithiasis?
Increased intake of calcium
Increased intake of potassium
Increased intake of animal protein
Increased intake of water
Which demographic group is most commonly affected by nephrolithiasis?
Infants
Elderly population
Middle-aged White men
Middle-aged Black women
Which of the following collection of symptoms is typically associated with kidney stones?
Cramping, intermittent flank/abdominal pain with nausea or vomiting
Headache, dizziness, and visual changes
Diarrhea with GI hemorrhage
Chest discomfort, shortness of breath, and palpitations
What is the best recommended first-line imaging modality for diagnosing nephrolithiasis?
Computed tomography (CT)
Electrocardiography (EKG)
Magnetic resonance imaging (MRI)
Plain radiograph of the abdomen (aka a KUB), or Ultrasonography (US)
When should a patient with a calculus larger than 10mm (or causing obstructive features) be referred to a urologist?
Only if the stone is causing symptoms
Immediately upon diagnosis
Only if the stone grows larger than 15mm
If the stone is radiolucent
What lifestyle modification is recommended for patients with a low risk of recurrent kidney stones?
Limiting fluid intake
Increasing sodium consumption
Consuming more animal protein
Achieving a normal body weight
References
Bishop K, Momah T, Ricks J. Nephrolithiasis. Prim Care.
2020;47(4):661-671. doi:10.1016/j.pop.2020.08.005
Wiki Commons. Kidney Anatomy. https://en.wikipedia.org/wiki/Kidney#/media/File:Blausen_0592_Kidne yAnatomy_01.png. Accessed November 13, 2023.
Curhan GC. Nephrolithiasis. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson J. eds. Harrison's Principles of Internal Medicine, 21e. McGraw Hill; 2022.
Wiki Commons. Kidney Stone. https://commons.wikimedia.org/wiki/File:Blausen_0592_KidneyAnatom y_01.png. Accessed November 13, 2023.
Lang J, Narendrula A, El-Zawahry A, Sindhwani P, Ekwenna O. Global Trends in Incidence and Burden of Urolithiasis from 1990 to 2019: An Analysis of Global Burden of Disease Study Data. Eur Urol Open Sci. 2022;35:37-46. Published 2022 Jan 3. doi:10.1016/j.euros.2021.10.008
Wilcox CR, Whitehurst LA, Cook P, Somani BK. Kidney stone disease: an update on its management in primary care. Br J Gen Pract. 2020;70(693):205-206. Published 2020 Mar 26.
doi:10.3399/bjgp20X709277
Scotland KB, Armas-Phan M, Dominique G, Bayne D. Social Determinants of Kidney Stone Disease: The Impact of Race, Income and Access on Urolithiasis Treatment and Outcomes. Urology. 2022;163:190-195. doi:10.1016/j.urology.2021.08.037
Scales CD, Smith AC, Hanley JM, Saigal CS. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160–165. 10.1016/j.eururo.2012.03.052.
Caudarella R, Vescini F. Urinary citrate and renal stone disease: the preventive role of alkali citrate treatment. Arch Ital Urol Androl. 2009;81(3):182-187.
Ferraro PM, Bargagli M, Trinchieri A, Gambaro G. Risk of Kidney Stones: Influence of Dietary Factors, Dietary Patterns, and Vegetarian-Vegan Diets. Nutrients. 2020;12(3):779. Published 2020 Mar 15. doi:10.3390/nu12030779
Fontenelle L and Sarti T. Am Fam Physician. 2019;99(8):490-496.
Favus M and Feingold K. Kidney Stone Emergencies. Endotext. 2018.
Lexicomp Online, Tamsulosin: UpToDate, Inc.; 2023. https://online.lexi.com. Accessed November 2023.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.