HYPERTENSION: FOCUSING MORE ATTENTION ON IDENTIFICATION AND INTERVENTION
JEANNETTE Y. WICK, RPh, MBA, FASCP
Jeannette Y. Wick is the Director of the Office of Pharmacy Professional Development at the University of Connecticut.
Topic Overview
About one-half of the US adult population has hypertension. The most common hypertension guideline used in the US is the American College of Cardiology (ACC)/American Heart Association (AHA) guideline. The guideline's four hypertension categories are Normal, Elevated, Stage I, and Stage II. Modifiable or lifestyle risk factors can be more critical than nonmodifiable risk factors. Patients who address lifestyle factors aggressively and consistently can reduce their risk for all cardiovascular-related events by up to 15%. With blood pressure monitoring devices now ubiquitous in pharmacies, screening is easier than ever. Simply asking patients if they have checked their blood pressure lately can prompt them to self-screen. Pharmacists should also screen patients with diagnosed hypertension for other cardiovascular risk factors.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-183-H01-P
Pharmacy Technician 0669-0000-23-184-H01-T
Credits: 2 hours of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 hours, including Course Test and course evaluation
Release Date: November 14, 2023 Expiration Date: November 14, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From November 14, 2023, through November 14, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Recognize the various types of garden variety hypertension
Describe risk factors and the appropriate lifestyle modifications
Compare first and second-line medications and their potential adverse effects
Identify appropriate interventions in the pharmacy
Disclosures
The following individuals were involved in developing this activity: Jeannette
Y. Wick, RPh, MBA, FASCP, and Pamela Sardo, PharmD, BS. Pamela Sardo was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
When clinicians think about patients who may have chronic garden variety hypertension, they might think about it in terms of a coin toss. In a coin toss, the chances of heads or tails are about 50%. Hypertension is similar: Roughly 50% of people develop hypertension. However, developing hypertension also differs from a coin toss since certain risk factors can increase the likelihood of developing this silent disease. If the statistics are true, half of patients will have hypertension, and this includes pharmacy patients. With pharmacists and staff becoming more involved in community- based care, they are positioned to act in the prevention and management of hypertension through team-based care. This continuing education activity will explore this common condition, identify reasons for its tremendous impact, and discuss treatment.
The Prevalence and Cumulative Impact of Hypertension
Approximately 116 million Americans—or about one-half of the United States (US), adult population—have hypertension (HTN), sometimes also referred to as elevated blood pressure. Globally, the statistics are similar.1-5 Only 24% of those affected have their blood pressure (BP) under control, and one in three adults have no idea they have HTN. In addition, in 2020, the death certificates of more than 670,000 Americans listed HTN as the primary cause of death.1-5 In a developed country, how can this happen with a condition that is so well understood? Many people who are insured, have primary care providers and have been seen recently or regularly remain undiagnosed. Somehow, healthcare providers miss the diagnosis or fail to treat HTN when it is identified.
Uncontrolled HTN is a common, modifiable risk factor for the leading cause of death in the United States: cardiovascular disease (CVD). It causes or contributes to chronic kidney disease, dementia, heart failure, stroke, and vision loss. Most cases of HTN are idiopathic in nature, and idiopathic HTN is also called primary or essential hypertension. Hypertension is also
symptomless, so many patients have no idea they have a chronic, dangerous condition.6
Hypertension's cost to American society tops $131 billion annually. Increasing awareness of HTN and its sequelae can reduce cardiovascular misadventure and healthcare costs. Once patients are aware of their HTN, patient education about appropriate medications and the importance of adherence is critical.1-5
Defining and Classifying Hypertension
Hypertension occurs when the BP force against arterial walls and through blood vessels increases dangerously.7 Sphygmomanometers (blood pressure cuffs) measure two components: systolic pressure and diastolic pressure in mm Hg. Systolic BP (SBP/the upper number) reflects the force when the heart pumps blood out of the ventricles and into the circulation. Diastolic BP (DBP/the lower number) measures the resting state in between heartbeats. Although the target blood pressure number has changed over the last century, the current consensus is that a normal BP is 130/80 mm Hg or lower, and persistent BP readings of 140/90 mm Hg require treatment. The most common HTN guideline used in the US is the American College of Cardiology (ACC)/American Heart Association (AHA) guideline, and it, too, uses the 130/80 threshold in patients who are untreated or being treated with antihypertensive medication.7
To diagnose HTN, clinicians need to average BP measurements from at least two patient visits on at least two separate occasions. Table 1 lists the guideline's four HTN categories.7
Table 1
Blood Pressure Classification in Adults
| Classification | Systolic and Diastolic Blood Pressure (mm Hg) |
| Normal | <120 and <80 |
| Elevated | 120-129 and <80 |
| Stage I | 130-139 or 80-89 |
| Stage II | >140 or >90 |
Pharmacists need to be aware of two other kinds of HTN: masked and white coat HTN. In masked hypertension, patients' office readings suggest normal BP, but readings taken at home or using ambulatory devices are consistently above normal. White coat hypertension occurs when office readings are elevated but they are normal outside the office.8 These conditions underscore the need for office and home monitoring.

Risk Factors for Hypertension
Risk factors for HTN are modifiable and nonmodifiable. Approximately 17% of people who have HTN have three or more risk factors.9 Nonmodifiable risk factors include age older than 65 years, ethnicity, and family history. In terms of ethnicity, Blacks, Pacific Islanders, and Hispanics are at elevated risk.7,10,11 People who have diabetes are also at elevated risk, and 71% of them develop HTN.12 In addition, obstructive sleep apnea is a risk factor, and it appears to be a factor in more than 80% of adults with resistant hypertension, discussed below.13
Modifiable or lifestyle risk factors can be more critical than nonmodifiable risk factors. Patients who address lifestyle factors aggressively and consistently can reduce their risk for all cardiovascular-related events up to 15%.14 Overweight, obesity, and abdominal adiposity; physical inactivity and sedentary lifestyles; high fat, low potassium, and high sodium diets; excessive alcohol intake; and smoking significantly increase an individual’s risk for HTN.7,10,11
One area in which knowledge is growing is that of the genetic response to salt.15 Salt sensitivity is especially common in Blacks, older adults, and those with higher BPs or comorbidities (e.g., chronic kidney disease, diabetes, or metabolic syndrome).7,16 Researchers from the United Kingdom have been able to identify a genetic association between blood pressure and 107 independent loci that had previously been suggested as contributors to HTN. They found an allele of the NADPH oxidase 4 (NOX4) locus that is linked to increased tissue-specific NOX4 expression in endothelial cells. NOX4 enhances endothelial vasodilatation and reduces blood pressure in vivo. It also generates reactive oxygen species in the kidney and the vasculature that may contribute to salt-sensitive hypertension. About 50% to 60% of patients are salt sensitive and therefore tend to develop hypertension.15 Currently, the techniques for measuring salt sensitivity are so complicated they are generally only used in clinical studies. Hopefully, better and cost-effective methods will be forthcoming.17
Screening for Hypertension
The US Preventive Services Task Force routinely looks at screening requirements for many diseases. For HTN, it recommends screening all adults aged 18 years and older. It further recommends screening adults aged 40 years or older or who are at increased risk for HTN annually. Among younger adults (aged 18 to 39 years) who have no risk factors, screening every three to five years is sufficient. Clinicians should conduct the first screening using an office, clinic, or pharmacy device. If HTN is a possibility or probability, clinicians can confirm the diagnosis by having the patient use either an ambulatory BP monitor or a home BP machine with validated and accurate devices.18
Managing Hypertension
Treatment goals for HTN are fairly straightforward. In addition to a goal BP of 130/80 mm Hg or less for most adults, the overarching goal is to reduce morbidity and mortality from cardiovascular events and to prevent complications such as kidney disease and heart failure. To achieve this goal,
clinicians need to recommend and educate patients about the necessity of nonpharmacologic actions and prescribe medication as appropriate. Technicians can be helpful, too, by reminding patients that the goal for BP is 120/80 or 130/90, depending on the patient’s age and comorbidities.
Nonpharmacologic Therapy
All patients with elevated BPs need to adopt some lifestyle modifications. Lifestyle modifications directly address the risk factors listed above. They include incorporating a heart-healthy diet, increasing potassium and reducing sodium intake, reducing alcohol consumption, focusing on physical activity, and losing weight. Used without medication, lifestyle modifications can reduce mean SBP by about 5 mm Hg in patients with HTN and by 2 to 3 mm Hg in patients without HTN.

The ideal diet plan for HTN focuses on healthier eating, reducing sodium intake, and increasing potassium intake. Reducing dietary sodium by 1,000 mg can lower SBP by 3 mm Hg, and increasing potassium intake by 0.6 g/day can result in a 1 mm Hg reduction in SBP. Two diets tend to be the best documented and most recommended. The Dietary Approaches to Stop Hypertension (DASH) diet and the Mediterranean diet both decrease the risk of HTN. Their emphasis on fruits, vegetables, whole grains, olive oil, nuts, and seeds makes sense and is easy for patients to understand. Such foods are calcium-, magnesium-, and potassium-dense, and they emphasize less red meat, sodium, and saturated and total dietary fat. They also educate patients about acceptable alcohol consumption (two or fewer drinks daily for men and
one or fewer drinks daily for women). Careful adherence to these or similar diets has resulted in lower SBP, with overall reductions up to 11 mm Hg, allowing for better BP control.7,19,20
As physical inactivity is a major risk factor for HTN, increasing exercise is critical. Exercise can reduce SBP by an average of 5 to 8 mm Hg and DBP by 3 mm Hg. The guidelines recommend at least 150 minutes per week of moderate-intensity physical activities, such as brisk walking. Often, when patients think about exercise, they think about aerobic exercises (e.g., cycling, dancing, swimming, running) and may feel overwhelmed by the idea. However, evidence indicates dynamic resistance exercise and static isometric exercises can also improve BP. Patients may find that starting slowly with low- intensity workouts and setting goals to increase them gradually will help build endurance and strength.7,21,22
Weight loss can lead to HTN reversal if patients lose enough weight, but it is quite a challenge for most patients. Modest weight loss can have a positive impact on BP; a 2- to 4-kg (2.2 to 8.8 pound) reduction in weight has been shown to decrease SBP by 3 to 8 mm Hg. The typical formula is to reduce caloric intake and increase physical activity, but this formula's success varies by patient. (Increasingly, researchers are finding that this formula may be overly simplified.) Ideally, experts recommend gradual weight loss, with a weekly goal of 1 to 2 kg (2.2 to 4.4 pounds).7,23

Smoking cessation, discussed below, and moderating or discontinuing alcohol use are also important. Technicians often have more time than pharmacists do to help patients find smoking cessation products; reviewing
the products and knowing how they differ can prepare technicians for questions.
Pharmacologic Therapy
Clinicians should start pharmacologic therapy based on the patient’s risk for atherosclerotic cardiovascular disease (ASCVD) and HTN stage (see Table 2) if lifestyle modifications alone do not help patients reach a normal BP. The ACC’s website includes an ASCVD Pooled Cohort Equations calculator (https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/) that can be downloaded as a mobile phone application. Many electronic medical records embed this tool in their clinical information software systems.7 The ACC considers patients to be at "elevated" risk if the Pooled Cohort Equations predicted risk is at least 10%. The ACC has validated this calculator is for US adults ages 40 to 79 years who are not taking concurrent statin therapy. For patients older than 79, the 10-year ASCVD risk generally exceeds 10%, and prescribers should instead use an SBP threshold of 130 mm Hg to start antihypertensive drug treatment. In all patients, prescribers need to consider predicted CVD risk in conjunction with BP to guide antihypertensive drug therapy.24,25,26
Table 2
Guideline Recommendations for Antihypertensive Treatment Initiation
| Classification | Treatment |
| Normal | Healthy lifestyle habits (prevention) |
| Elevated | Nonpharmacologic interventions (lifestyle modification) |
| Stage I | CVD risk < 10%: Use nonpharmacologic interventions CVD risk > 10%: Use nonpharmacologic interventions and add antihypertensive(s) |
| Stage II | Use nonpharmacologic interventions and add antihypertensive(s); consider two antihypertensives as initial therapy |
| ABBREVIATION: CVD = cardiovascular disease | |
Fortunately, clinicians can choose from a wide array of antihypertensives when medication is needed. The ACC/AHA guideline recommends thiazide diuretics, calcium channel blockers, and angiotensin- converting enzymes or angiotensin receptor blockers as first-line therapies. Table 3 lists these medications and describes common ADRs.7,26 Clinical trials have shown that all these medications can reduce clinical events. Once daily medications simplify treatment and improve adherence. Clinicians should check a patient’s blood pressure every two to four weeks after starting medication.7
Table 3
Initial Therapy: Thiazide Diuretics, Calcium Channel Blockers, and Angiotensin-Converting Enzymes, Angiotensin Receptor Blockers
| Medication Class and Approved Medications* | Potential Class Adverse Events and Counseling Points* |
Angiotensin-converting enzyme inhibitors Benazepril Captopril Enalapril Fosinopril Lisinopril Moexipril Perindopril Quinapril Ramipril Trandolapril | All ACE inhibitors are oral, except enalapril, which can be given orally or intravenously (enalaprilat). Initiate at the lower end of the adult dosing range for geriatric patients Decrease doses in patients with heart failure, salt-depleted patients, and/or renal impairment Up to 10% of patients develop a dry, nonproductive paroxysmal cough; it occurs more frequently in women. It may require treatment discontinuation Most common adverse events include angioedema, headache, dizziness, and cough; (hypotension and hypertension Monitor blood pressure, renal function and serum potassium periodically |
Angiotensin Receptor Blockers Azilsartan Candesartan Irbesartan Losartan | Rare cases of angioedema and cough reported Contraindicated in patients with bilateral renal artery stenosis or |
Olmesartan Valsartan | patients with heart failure who have hypotension Most common adverse reactions (include dizziness, headache, diarrhea, upper respiratory infection, nasal congestion, back pain Reduce dose in hepatic impairment |
Calcium Channel Blockers Amlodipine Felodipine Isradipine Nicardipine SR Nifedipine LA Nisoldipine | Most common adverse reactions include peripheral edema, dose- dependent headache and edema: headache, fatigue, nausea, abdominal pain, and somnolence In geriatric patients, start dosing at the low end of the dose range Titrate slowly in patients with severe hepatic impairment All CCBs are major CYP450 3A4 substrates; diltiazem and verapamil are P-gp substrates and moderate 3A4 inhibitors; avoid grapefruit |
Thiazide Diuretics Chlorthalidone HydroCHLOROthiazide† Indapamide Metolazone | Numerous adverse effects are possible, but this is a very old drug and the incidences are unclear; most common include electrolyte imbalances, dizziness, photosensitivity, hyperuricemia (usually asymptomatic rarely leading to gout), hypochloremic alkalosis in patients at risk (e.g., hypokalemic patients), hyperglycemia and glycosuria in patients with diabetes. Monitor serum electrolytes periodically |
*Taken from References 26-30
†TALL man lettering from Reference 31
Many medications used today have been available for many years and are inexpensive. For this reason, treating HTN early is not only smart but also cost-effective.32 Clinicians usually start patients whose BP is at least 140/80 or who have an ASCVD risk exceeding 7.5% on one drug, and often, they choose hydroCHLOROthiazide (HCTZ) or the related chlorthalidone, which rarely causes adverse effects. By increasing the amount of urine produced and
excreted by the kidneys, diuretics decrease blood volume and lower BP. The effectiveness evidence is better for chlorthalidone and indapamide than for hydroCHLOROthiazide, but clinicians tend to use hydroCHLOROthiazide more often than the others (probably by sheer habit).33,34
Prescribers should consider up-titrating two drugs of different classes for patients with stage 2 HTN. They also need to consider the patient's age, concurrent medications, drug adherence, drug interactions, the overall treatment regimen, out-of-pocket costs, and comorbidities. Here, as in all treatments, clinicians need to employ clinical judgment to help patients with shared decision-making.7
Recent trends in prescribing have explored the idea of earlier use of combination pills.35 Monotherapy and its up-titration are often ineffective, time-consuming, and frustrating for prescribers and patients. A number of studies have found that using a drug combination early can reduce BP more effectively and faster. The results indicate a higher proportion of patients achieve targets with favorable cardiovascular outcomes. Yet up to one-third of patients will need three or more antihypertensive drugs.35 For example, a randomized, placebo-controlled, double-blind, crossover trial (N = 55 participants with untreated HTN) used a "quadpill."36 It was a capsule containing irbesartan 37.5 mg, amlodipine 1.25 mg, hydroCHLOROthiazide
6.25 mg, and atenolol 12.5 mg); these are a quarter of the components’ usual doses. Patients treated with the quadpill attained an average reduction in SBP of 19 mm Hg and in-office BP of 22/13 mm Hg. All participants reached a target of less than 140/90 mm Hg during the quadpill arm compared to 33% of placebo-treated participants.36
Prescribers should start patients with stage II HTN initially with two medications from different classes.7,26 ACE inhibitors and ARBs are effective treatments for HTN, and prescribers often use them for patients with underlying heart disease, diabetes, or kidney disease. ACE inhibitors block the conversion of angiotensin I to angiotensin II, decreasing BP and reducing sodium and fluid retention. ARBs block angiotensin II, decreasing BP and
improving blood flow. ACE inhibitors and ARBs are usually well-tolerated but may cause cough, dizziness, and hyperkalemia.7,33,34
Calcium channel blockers are also effective. Calcium channel blockers block the entry of calcium into cardiac and vascular cells, decreasing BP and improving blood flow. Both classes may cause dizziness, fatigue, and gastrointestinal disturbances.7,33,34
Once the BP exceeds 20/10 mm Hg above the target BP level, prescribers will need to employ at least two drugs.7,33,34 Various combinations include ACE inhibitors, ARBs, or calcium channel blockers with thiazide diuretics. Prescribers should individualize the drugs in combination therapy based on the patient’s specific needs, tolerability, and potential adverse effects, especially with drugs associated with electrolyte disturbances. They should also avoid using two drugs with the same (or similar) mechanisms of action.7,33,34 Additional medications (see Table 3) are available and can be considered for resistant HTN.
Table 4
Additional drugs for Hypertension
| Medication Class and Approved Medications* | Potential Class Adverse Events and Counseling Points* |
Alpha1 antagonists Doxazocin Prazosin Terazosin | Common adverse effects include orthostatic hypotension (especially on the first dose), headache, pounding heartbeat, fatigue, weakness, tachycardia, and tremulousness Caution in elderly patients or if previous cataract surgery, marked renal impairment, cerebrovascular disease, coronary artery disease, or current respiratory infection |
Beta-blockers (cardioselective) Atenolol Betaxolol Bisoprolol | Common adverse effects include bradycardia, hypotension, fatigue, dizziness, nausea, constipation, sexual dysfunction and erectile dysfunction |
| Metoprolol | Lesser known but troubling effects include insomnia, sleep changes and nightmares while using beta-blockers Metaprolol should be taken with food |
Beta-blockers (non- cardioselective) Nadolol Propranolol | Common adverse effects include bradycardia, hypotension, fatigue, dizziness, nausea, constipation, sexual dysfunction and erectile dysfunction Do not use in patients with asthma |
Beta-blockers (third- generation β- adrenoreceptor antagonists) Carvedilol Nebivolol | Have additional endothelium- dependent vasodilating properties Common adverse effects include headache, fatigue, dizziness, hypotension, diarrhea, hyperglycemia, asthenia, bradycardia, weight increase, dyslipidemia |
Central alpha2 agonists Clonidine Guanfacine Methyldopa | Most common adverse effects are sedation and fatigue Contraindications include concurrent use of phosphodiesterase inhibitors, orthostatic hypotension, and any condition leading to autonomic instability |
Direct vasodilators Hydralazine Minoxidil | Common adverse effect include For hydralazine: compensatory tachycardia, headache, angina, SLE-like symptoms (in slow acetylators), fluid retention. For minoxidil: hypertrichosis, water retention, tachycardia, hair growth, pericarditis that may progress to tamponade. Minoxidil is contraindicated in patients with coronary artery disease or angina, as it can cause compensatory tachycardia. It is also contraindicated in patients with mitral valve rheumatic heart disease |
Loop diuretics Furosemide Torsemide | Most common adverse effects include excessive urination, hyponatremia, hypokalemia, hypochloremia, hypomagnesemia, metabolic alkalosis, prerenal azotemia, dehydration, hypertriglyceridemia, hypercholesterolemia, hyperuricemia, gout, restlessness, headache, dizziness, vertigo, postural hypotension, syncope, skin photosensitivity, interstitial nephritis, tinnitus, ototoxicity, deafness, and in patients with renal failure who receive high doses, myalgias, and muscle soreness Contraindications to loop diuretics include anuria, hypersensitivity to furosemide, bumetanide, or torsemide (or sulfonamides), hepatic coma, severe electrolyte depletion May cause or contribute to ototoxicity especially is injected rapidly or with severe renal impairment, the use of higher than recommended doses, hypoproteinemia or concomitant therapy with ototoxic drugs |
Mineralocorticoid receptor antagonists Eplerenone Spironolactone | Adverse reactions include dose- dependent, reversible hyperkalemia and acute renal function decline. In men, gynecomastia, loss of libido, and general feminization; in women, menstrual irregularities Sex-related adverse events are noted mainly in spironolactone; switching to eplerenone could attenuate those effects. |
Potassium-sparing diuretics Amiloride Triamterene | Common adverse effects include headache, nausea, vomiting, anorexia, diarrhea/constipation, hyperkalemia, dizziness, fatigue, dry mouth, dehydration, rash, muscle cramps, |
weakness, xerostomia, azotemia, and hyperuricemia, hyperuricemia Both have boxed warnings for hyperkalemia (K > 5.5 mEq/L) |
*Taken from References 37-48
Despite the available treatments, almost 75% of patients continue to have uncontrolled HTN. Pharmacists need to examine the many reasons why this is so.49-51
Clinicians may prescribe suboptimal dosing, fail to intensify the treatment when patients respond poorly (called clinical inertia), or select a drug that simply does not work for the patient.
Patients may have limited access to or use of healthcare or simply have nonadherence issues with lifestyle modifications and/or prescribed antihypertensives. Adherence is critical to improving HTN control, but evidence indicates that approximately 12% of patients with HTN never fill initial prescriptions. Additionally, one year after the initiation of hypertensives, the average adherence rate is lower than 50%.
The combination of prescriber and patient issues can be deadly. Poorly controlled HTN increases the likelihood of cardiovascular events and stroke.
Hypertensive Emergencies and Resistant Hypertension
Some patients experience hypertensive emergencies, defined as a rapidly accelerating blood pressure that reaches or exceeds 180/120 mm Hg.7 Such situations can lead to organ damage or cardiovascular damage, so it is critical that patients access treatment immediately. Some examples of target organ damage include acute coronary syndrome, acute kidney injury, aortic dissection, encephalopathy, and pulmonary edema. A hypertensive crisis can be life-threatening. If no organ damage has occurred, clinicians should treat the patient with any oral medication that has an onset of action within 15 to 30 minutes. They should expect to see a BP reduction over the next 24 to 48 hours. If there is evidence of organ damage, they should treat the patient with
IV medications and attempt to reduce blood pressure by no more than 10% to 25% in the first hour. Next, they should attempt to reduce blood pressure to 160/100 mm Hg over the next two to six hours. Typical intravenous medications include clevidipine, enalaprilat, esmolol, fenoldopam, hydralazine, labetalol, nicardipine, nitroglycerin, phentolamine, and sodium nitroprusside. The guidelines contain tables describing appropriate doses and contraindications.7
Resistant hypertension (RH) is a BP above target despite the use of at least three antihypertensives from different substance classes, including a diuretic in appropriate doses and combinations. Before diagnosing RH, clinicians need to rule out poor adherence to prescribed medicines, white-coat phenomenon, faulty BP measurements, and irrational regimens and/or inadequate dosing.7 Between 10% and 15% of patients who are treated for hypertension develop RH.52
Once nonadherence, white-coat phenomenon, faulty measurements, and prescribing issues are ruled out, clinicians should re-examine lifestyle factors such as obesity or alcohol consumption. They should also check to make sure patients are not using vasopressors or sodium-retaining substances such as oral contraceptives, nonsteroidal anti-inflammatory drugs and analgesics, cancer therapies, or steroids.53
The approach to RH is similar to that of essential HTN. Clinicians need to reemphasize the importance of sodium restriction, weight loss, and physical activity.
When RH occurs, experts indicate using an effective diuretic is critical. RH is often associated with sodium retention, volume excess, and/or high sympathetic tone. Indapamide and chlorthalidone have longer durations of action than hydroCHLOROthiazide and may be more effective.54-56 Spironolactone has been a standard of care in RH and remains the mineralocorticoid receptor antagonist of choice. Its adverse effect profile has made many prescribers wary of using it, but its antihypertensive effect is
better than eplerenone’s. Eplerenone is an alternative if patients cannot tolerate spironolactone but must be taken twice daily.57
Beta-blockers are used less often than previously. Randomized controlled trials and meta-analyses have found that beta blockers reduce the risk of stroke, heart failure, and major cardiovascular events. However, they are less effective than first-line drugs for stroke. Patients also tend to discontinue them because of adverse effects, and they increase the risk for new-onset diabetes.58-60 Prescribers should avoid the direct vasodilators, such as hydralazine and minoxidil.34 They can cause fluid retention and increased sympathetic tone. When they are employed. They must be given with loop diuretics and beta blockers in divided doses during the day (meaning once- daily dosing is not possible).34
Hypertension Intervention: Pharmacy Matters
Pharmacists see patients who have HTN frequently—if the statistics are true (and we know they are), half of their patients have HTN. The CDC, recognizing the pharmacist's growing contribution to community-based care, has issued a call to action for pharmacists to prevent and manage HTN through team-based care. Its comprehensive resource guide, “Using the Pharmacists’ Patient Care Process to Manage High Blood Pressure: A Resource Guide for Pharmacists,” describes the pharmacists' responsibilities in medication management that can help patients optimize their antihypertensive regimens. Working with other healthcare providers, pharmacists can identify the adverse effects that patients may experience and modify or change drug therapy to improve the patient's response.
Patient counseling starts with heightening awareness, which could be as simple as making it a goal to ask all patients who are 40 or older if they have had their blood pressure taken recently. Certainly, this is an area where technicians can help. Thorough education about lifestyle modifications and medication is critical. It should include an emphasis on adherence to lifestyle modifications and medication and a frank discussion about potential adverse events and the fact that they can be managed.
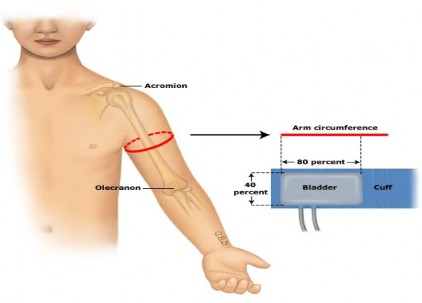
Every patient who has uncontrolled HTN needs a mechanism to monitor BP at home.7 They need to know how to use the machine, and they should also keep a log of their blood pressure and bring it to every visit. Many automated devices store recent blood pressure readings. Pharmacists need to remind patients to sit quietly for at least five minutes with their feet on the floor, and legs uncrossed before taking their blood pressure. They should sit up straight and have their arms supported on a hard surface. Most directions from reputable sources indicate the blood pressure cuff should cover 80% of the arm circumference; ill-fitting pressure cuffs can underestimate or overestimate blood pressure readings.7 These directions are vague. They make more sense when one understands that the part of the machine that wraps around the arm is divided into two parts: the inflatable bladder and the flat part covered in Velcro (the actual cuff). The bladder should cover about 80% of the arm circumference measured at about the armpit level. In addition, the height of the cuff should cover about 40% of the arm between the shoulder and the elbow, as illustrated in the figure entitled Selecting the Correct Cuff Size for Monitoring Blood Pressure below.61
Selecting the Correct Cuff Size for Monitoring Blood Pressure
In some cases, prescribers use ambulatory blood pressure monitoring (ABPM) devices that track BP while patients go about their normal daily activities. They are most helpful when patients seem to experience nocturnal “dipping,” early-morning BP surges, or overt symptoms.62 Asking patients to document that they took their medication with their blood pressure reading daily can improve adherence. It also helps patients and healthcare providers make informed decisions about medication management and acknowledge the benefits of lifestyle modifications.16,63,64
Since lifestyle modification needs to continue throughout life, pharmacists should touch base with patients periodically to ensure they remain diligent in five areas: weight management, salt restriction, tobacco cessation, adequate management of obstructive sleep apnea, and exercise.
Weight management. For every 5% increase in body weight, the risk of HTN increases by 20-30%.60 Patients who are overweight or obese may see a reduction in BP if they lose weight. Experts have yet to find the optimum body mass index (BMI) and optimal weight range to target in patients with HTN, but it is clear that weight loss alone can decrease BP by 5 to 20 mm Hg in systolic blood pressure.
Findings from multiple studies over the years indicate that obesity affects insulin and leptin resistance, perivascular adipose tissue dysfunction, renal impairment, renin-angiotensin-aldosterone-system activation, and sympathetic nervous system activity. These can all contribute to HTN.65 Patients who lose weight often regain the weight (and often gain more than they lost), and become frustrated, so the long-term benefit is lost. For patients who qualify by virtue of weight and/or comorbidities, bariatric surgery is more likely to lead to permanent weight reduction and significant dramatic declines in blood pressure and attenuation of long-term cardiovascular risk.66 Pharmacists need to monitor patients carefully when they start to lose weight successfully. Patients will need medication changes as they lose weight and their BP falls. Celebrating the discontinuation of medication (and pointing out that they can spend the copay or the cost of the drugs elsewhere) is one way to encourage patients.
Salt restriction. In the United States, the primary sources of dietary sodium are processed foods or commercially prepared food from sit-down and fast-food restaurants.67 The AHA recommends no more than 2,300 mg of salt daily and is considering dropping that limit to 1500 mg.68 That said, the average American consumes more than 3,400 mg of sodium daily. The AHA says that for that reason, reducing salt intake by 1,000 mg daily can significantly improve blood pressure and heart health.68 Pharmacists can reinforce the nutritionist’s counseling and remind patients to read labels carefully for sodium content. In addition, they can clear up a point of confusion for patients. Patients often cannot visualize salt in milligrams. Telling them that 2300 mg of sodium is about one level teaspoonful measured with a measuring spoon can help them understand how much (or little) they can consume.69 Technicians can help patients read labels to determine its salt or sodium content.
Tobacco cessation. Tobacco use contributes significantly to various causes of morbidity and mortality. Smoking cessation programs (SCPs) can be effective, cost-effective, and an excellent way to help people with HTN.
Research indicates that quit rates for patients who enroll is traditional or abbreviated pharmacist-led smoking cessation programs range from 22% to 36% compared to rates of about 7% in smokers who do not use a structured program.70
Finally, pharmacists can discuss adequate management of obstructive sleep apnea and exercise with patients and reinforce messages from other interdisciplinary team members.
Medication Considerations
Many antihypertensives are available as combination products. In the initial titration, however, using single-component tablets or capsules is best; if the patient doesn’t respond or experiences adverse effects, the offending drug can be discontinued. Table 4 lists a few key points to remember.
There are basic points to remember when treating patients with primary HTN:71,72
Patients who take diuretics need to
consume potassium-rich foods; often, recommending they eat a banana daily meets the requirement.
take their last dose no later than 4 PM to avoid nocturnal diuresis
Do not use ACE inhibitors and ARBs together
If the patient does not respond to an antihypertensive within one month, up-titration or the addition of an additional medication from another class is warranted.
ACE inhibitors, ARBs, and aliskiren (a direct renin inhibitor) are contraindicated in pregnancy. The American College of Obstetricians and Gynecologists recommends labetalol, nifedipine extended release, and methyldopa as first-line antihypertensives in pregnancy.
Do not use potassium-based salt substitutes while taking these medications
Frequent use of non-steroidal anti-inflammatory drugs can reduce many antihypertensives’ effectiveness.
All diuretics can decrease lithium clearance.
Do not discontinue beta-blockers, alpha-2 adrenergic agonists, or clonidine abruptly. Taper over one to two weeks.
Beta-blockers can enhance insulin’s and sulfonylureas’ glucose-lowering effects and mask hypoglycemia.
If patients use the clonidine patch, they need to remove it before magnetic resonance imaging.
If patients forget a dose, they should take it as soon as they remember unless it is close to the next dose.
ACE inhibitors, ARBs, and long-acting calcium channel blockers are preferred in patients with metabolic syndrome because they do not affect glucose metabolism or weight.
Nonadherence is epidemic in patients with HTN, so pharmacists should help patients identify adherence barriers (e.g., forgetfulness, adverse effects, and cost) and help them address contributing factors.16,63,64
Summary
The most common HTN guideline used in the US is the ACC/AHA guideline. This guideline uses the 130/80 threshold in patients who are untreated or being treated with antihypertensive medication. To diagnose HTN, clinicians need to average BP measurements from at least two patient visits on at least two separate occasions. The guideline's four HTN categories are Normal, Elevated, Stage I, and Stage II. Two other kinds of HTN are masked and white coat HTN.
Risk factors for HTN are modifiable and nonmodifiable. In terms of ethnicity, Blacks, Pacific Islanders, and Hispanics are at elevated risk. People who have diabetes are also at elevated risk. In addition, obstructive sleep apnea is a risk factor.
Modifiable or lifestyle risk factors can be more critical than nonmodifiable risk factors. Patients who address lifestyle factors aggressively and consistently can reduce their risk for all cardiovascular-related events up to 15%. Overweight, obesity, and abdominal adiposity; physical inactivity and sedentary lifestyles; high fat, low potassium, and high sodium diets; excessive alcohol intake; and smoking significantly increase an individual’s risk for HTN.
One area in which knowledge is growing is that of the genetic response to salt. Salt sensitivity is especially common in Blacks, older adults, and those with higher BPs or comorbidities (e.g., chronic kidney disease, diabetes, or metabolic syndrome).
With BP monitoring devices now ubiquitous in pharmacies, screening is easier than ever. Simply asking patients if they have checked their BP lately can prompt them to self-screen. Pharmacists should also screen patients with diagnosed HTN for other cardiovascular risk factors, such as diabetes, smoking, and elevated lipid levels.
Course Test
Which of the following accurately describes white coat hypertension?
Two consecutive readings exceeding 130/80 in any healthcare setting
Normal office readings with elevated readings outside the office
One reading exceeding 180/120 in the office, but normal readings at home
Elevated office readings with normal readings outside the office
Which of the following accurately describes masked hypertension?
Two consecutive readings exceeding 130/80 in any healthcare setting
Normal office readings with elevated readings outside the office
One reading exceeding 180/120 in the office, but normal readings at home
Elevated office readings with normal readings outside the office
Which of the following patients has three risk factors for hypertension?
A White 37-year-old female who has diabetes and asthma
A 72-year-old Hispanic male whose parents both had hypertension
A 36-year-old female who is obese and walks 5 miles every day
A 25-year-old male who has the gene for salt sensitivity
When patients who have hypertension have sedentary lifestyles, how many minutes of exercise should pharmacists recommend?
115 minutes per day of moderate-intensity physical activity
150 minutes per week of moderate-intensity physical activity
150 minutes per week of high-intensity physical activity
150 minutes per week of any activity that gets the patient moving
A patient who is obese is diagnosed with hypertension. He asks how his obesity is related to his hypertension. Which of the following is the BEST answer?
For every 5-pound increase in body weight, the risk for hypertension increases roughly 25%.
Obesity has a profound effect on hypertension, reversible only by bariatric surgery.
For every 5% increase in body weight, the risk of hypertension increases by 20 to 30%.
Losing weight may lower your blood pressure, but it cannot eliminate the need for medication.
The American Heart Association is considering changing its recommendation for daily sodium consumption. What change are they considering?
Reducing the recommendation from 2300 mg of salt to 1500 mg of salt daily
Eliminating the daily recommendation entirely and simply advising patients to cut down
Changing the recommendations from describing consumption in milligrams to teaspoons
Recommending that all patients use potassium-containing salt substitutes exclusively
Which of the following is a list of first-line medications to be used in hypertension?
HydroCHLOROthiazide, lisinopril, and valsartan
Chlorthalidone, doxazosin, and metoprolol
Indapamide, metolazone, and propranolol
Clonidine, hydroCHLOROthiazide, and lisinopril
A prescriber started a patient on a combination of hydroCHLOROthiazide and another antihypertensive. After about two weeks, the patient returned to the pharmacy complaining of a cough. Which of the following medications, if co-prescribed, would most likely cause a cough?
HydroCHLOROthiazide
Azilsartan
Captopril
Amlodipine
A patient comes to the pharmacy with new prescriptions for her hypertension. She has been taking chlorthalidone daily for a month, but she reports that her blood pressure continues to be elevated. Her new prescriptions are for losartan and lisinopril. Why would you call the prescriber?
Losartan and lisinopril are both diuretics.
The guidelines recommend stronger antihypertensives after diuretics.
Before adding a drug, someone should assess the patient's adherence.
Patient should not take ACE inhibitors and ARBs together.
Which of the following medications is preferred in patients who have metabolic syndrome?
ACE inhibitors, ARBs, and calcium channel blockers
Hydrochlorothiazide, ace inhibitors, and propranolol
Labetalol, nifedipine extended release, and methyldopa
Amiloride and triamterene
References
Centers for Disease Control and Prevention. Facts about hypertension.
CDC. January 5, 2023. www.cdc.gov/bloodpressure/facts.htm. Accessed
September 25, 2023.
GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659-1724.
Centers for Disease Control and Prevention. 5 Surprising facts about high blood pressure. CDC. December 13, 2022. www.cdc.gov/bloodpressure/5_surprising_facts.htm. Accessed September 25, 2023.
Kirkland EB, Heincelman M, Bishu KG, et al. Trends in healthcare expenditures among US adults with hypertension: national estimates, 2003-2014. J Am Heart Assoc. 2018;7(11):e008731.
Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223-237. doi:10.1038/s41581-019-0244- 2
Wall HK, Hannan JA, Wright JS. Patients with undiagnosed hypertension: hiding in plain sight. JAMA. 2014;312(19):1973-1974.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):e13-e115.
Banegas JR, Ruilope LM, de la Sierra A, et al. High prevalence of masked uncontrolled hypertension in people with treated hypertension. Eur Heart J. 2014;35:3304–12.
Wilson PW, Kannel WB, Silbershatz H, D'Agostino RB. Clustering of metabolic factors and coronary heart disease. Arch Intern Med. 1999;159(10):1104-1109. doi:10.1001/archinte.159.10.1104
Centers for Disease Control and Prevention. Know your risk for high blood pressure. CDC. March 17, 2023. www.cdc.gov/bloodpressure/risk_factors.htm. Accessed September 25, 2023.
Andriolo V, Dietrich S, Knüppel S, et al. Traditional risk factors for essential hypertension: analysis of their specific combinations in the EPIC-Potsdam cohort. Sci Rep. 2019;9(1):1501.
Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States. Atlanta, GA: U.S. Department of Health and Human Services; 2014.
Pedrosa RP, Drager LF, Gonzaga CC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;58:811–7.
Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, Murray CJ, Ezzati
M. The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009;6(4):e1000058.
Warren HR, Evangelou E, Cabrera CP, et al. Genome-wide association analysis identifies novel blood pressure loci and offers biological insights into cardiovascular risk [published correction appears in Nat Genet. 2017 Sep 27;49(10 ):1558]. Nat Genet. 2017;49(3):403-415.
doi:10.1038/ng.3768
Richardson SI, Freedman BI, Ellison DH, Rodriguez CJ. Salt sensitivity: a review with a focus on non-Hispanic blacks and Hispanics. J Am Soc Hypertens. 2013;7(2):170-179. doi:10.1016/j.jash.2013.01.003
Elijovich F, Weinberger MH, Anderson CA, et al. Salt Sensitivity of Blood Pressure: A Scientific Statement From the American Heart Association [published correction appears in Hypertension. 2016 Oct;68(4):e62]. Hypertension. 2016;68(3):e7-e46. doi:10.1161/HYP.0000000000000047
U.S. Preventive Services Task Force. Screening for hypertension in adults: U.S. Preventive Services Task Force reaffirmation recommendation statement. JAMA. 2021;325(16):1650-1656.
Cicero AFG, Veronesi M, Fogacci F. Dietary intervention to improve blood pressure control: beyond salt restriction. High Blood Press Cardiovasc Prev. 2021;28(6):547-553.
Bazzano LA, Green T, Harrison TN, Reynolds K. Dietary approaches to prevent hypertension. Curr Hypertens Rep. 2013;15(6):694-702.
Hegde SM, Solomon SD. Influence of physical activity on hypertension and cardiac structure and function. Curr Hypertens Rep. 2015;17(10):77.
Barone Gibbs B, Hivert MF, Jerome GJ, et al. Physical activity as a critical component of first-line treatment for elevated blood pressure or cholesterol: who, what, and how?: a scientific statement from the American Heart Association. Hypertension. 2021;78(2):e26-e37.
Harsha DW, Bray GA. Weight loss and blood pressure control (Pro).
Hypertension. 2008;51(6):1420-1425.
Karmali KN, Lloyd-Jones DM. Global risk assessment to guide blood pressure management in cardiovascular disease prevention. Hypertension. 2017;69:e2–9.
Muntner P, Whelton PK. Using predicted cardiovascular disease risk in conjunction with blood pressure to guide antihypertensive medication treatment. J Am Coll Cardiol. 2017;69:2446–56.
Carey RM, Moran AE, Whelton PK. Treatment of hypertension: a review.
JAMA. 2022;328(18):1849-1861.
COZAAR (losartan potassium) tablets [package insert]. Organon. 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/020386s0 64lbl.pdf. Accessed September 25, 2023.
NORVASC® (amlodipine besylate) tablets [package insert]. Pfizer. 2011.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/019787s0 47lbl.pdf. Accessed September 25, 2023.
Zestril® (lisinopril) tablets [package insert]. 2014. https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/019777s0 64lbl.pdf. Accessed September 25, 2023.
Hydrochlorothiazide Tablets [package insert]. Mylan Pharmaceuticals. 2011.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/040735s0 04,040770s003lbl.pdf. Accessed September 25, 2023.
Institute for Safe Medication Practices. FDA and ISMP Lists of Look-Alike Drug Names with Recommended Tall Man Letters. ISMP. 2016. https://www.ismp.org/sites/default/files/attachments/2017- 11/tallmanletters.pdf. Accessed November 10, 2023.
Rubinstein A, Colantonio L, Bardach A, et al. Estimation of the burden of cardiovascular disease attributable to modifiable risk factors and cost- effectiveness analysis of preventative interventions to reduce this burden in Argentina. BMC Public Health. 2010;10:627.
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2019;74(10):1428-1429] [published correction appears in J Am Coll Cardiol. 2020 Feb 25;75(7):840]. J Am Coll Cardiol. 2019;74(10):1376-1414. doi:10.1016/j.jacc.2019.03.009
Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension [published correction appears in J Hypertens. 2019 Jan;37(1):226]. J Hypertens. 2018;36(10):1953-2041. doi:10.1097/HJH.0000000000001940
Volpe M, Gallo G, Tocci G. New approach to blood pressure control: Triple combination pill. Trends Cardiovasc Med. 2020;30(2):72-77. doi:10.1016/j.tcm.2019.03.002
Chow CK, Thakkar J, Bennett A, et al. Quarter-dose quadruple combination therapy for initial treatment of hypertension: placebo- controlled, crossover, randomised trial and systematic review. Lancet. 2017;389(10073):1035-1042. doi:10.1016/S0140-6736(17)30260-X
Sica DA, Pool JL. Current Concepts of Pharmacotherapy in Hypertension
- Alpha-Adrenergic Blocking Drugs: Evolving Role in Clinical Medicine. J Clin Hypertens (Greenwich). 2000;2(2):138-142.
Oliver E, Mayor F Jr, D'Ocon P. Beta-blockers: Historical Perspective and Mechanisms of Action. Rev Esp Cardiol (Engl Ed). 2019;72(10):853- 862. doi:10.1016/j.rec.2019.04.006
Grimm RH Jr. alpha 1-antagonists in the treatment of hypertension. Hypertension. 1989;13(5 Suppl):I131-I136. doi:10.1161/01.hyp.13.5_suppl.i131
Kallistratos MS, Pittaras A, Theodoulidis I, Grassos C, Poulimenos LE, Manolis AJ. Adverse Effects of Mineralocorticoid Receptor Antagonist Administration. Curr Pharm Des. 2018;24(46):5537-5541. doi:10.2174/1381612825666190222144359
Parthasarathy HK, Ménard J, White WB, et al. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. J Hypertens. 2011;29(5):980-990. doi:10.1097/HJH.0b013e3283455ca5
Reinhart M, Puil L, Salzwedel DM, Wright JM. First-line diuretics versus other classes of antihypertensive drugs for hypertension. Cochrane Database Syst Rev. 2023;7(7):CD008161. doi:10.1002/14651858.CD008161.pub3
Martins VM, Ziegelmann PK, Ferrari F, et al. Thiazide diuretics alone or combined with potassium-sparing diuretics to treat hypertension: a systematic review and network meta-analysis of randomized controlled trials. J Hypertens. 2023;41(7):1108-1116. doi:10.1097/HJH.0000000000003436
DMADEX (torsemide) tablets [prescribing information]. Meda Pharmaceuticals Inc. 2016. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020136s0 27lbl.pdf. Accessed September 25, 2023.
LASIX (furosemide) tablets [prescribing information]. Ssanofi-aventis. 2011.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016273s0 66lbl.pdf. Accessed September 25, 2023.
Dyrenium (triamterene) capsules prescribing information]. Concordia Pharmaceuticals Inc. 2023. https://medlibrary.org/lib/rx/meds/dyrenium/. Accessed September 25, 2023.
Amiloride HCl tablets [prescribing information]. Padagis US LLC. 2021. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=2b70 cf0c-45be-428f-b396-5001ed4e30fc. Accessed September 25, 2023.
NEBIVOLOL tablets FDA Report. Torrent Pharmaceuticals Limited. 2023. https://fda.report/DailyMed/3e3dc363-731f-4115-b685-a17620dd2034. Accessed September 25, 2023.
Million Hearts. Estimated hypertension prevalence, treatment, and control among U.S. adults. March 22, 2021. https://millionhearts.hhs.gov/data-reports/hypertension- prevalence.html. Accessed September 25, 2023.
Choudhry NK, Kronish IM, Vongpatanasin W, et al. Medication adherence and blood pressure control: a scientific statement from the American Heart Association. Hypertension. 2022;79(1):e1-e14.
Burnier M, Egan BM. Adherence in hypertension. Circ Res.
2019;124(7):1124-1140.
Noubiap JJ, Nansseu JR, Nyaga UF, et al. 2019. Global prevalence of resistant hypertension: a meta-analysis of data from 3.2 million patients. Heart. 105:98–105.
Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874-2071. doi:10.1097/HJH.0000000000003480
Dineva S, Uzunova K, Pavlova V, et al. Comparative efficacy and safety of chlorthalidone and hydrochlorothiazide-meta-analysis. J Hum Hypertens. 2019;33:766–774
Roush GC, Ernst ME, Kostis JB, et al. Head-to-head comparisons of hydrochlorothiazide with indapamide and chlorthalidone: antihypertensive and metabolic effects. Hypertension. 2015;65:1041- 1046
Roush GC, Holford TR, Guddati AK. Chlorthalidone compared with hydrochlorothiazide in reducing cardiovascular events: systematic review and network meta-analyses. Hypertension 2012;59:1110-1117.
Bazoukis G, Thomopoulos C, Tse G, Tsioufis C. Is there a blood pressure lowering effect of MRAs in heart failure? An overview and meta- analysis. Heart Fail Rev. 201823:547-553.
Thomopoulos C, Bazoukis G, Tsioufis C, Mancia G. Beta-blockers in hypertension: overview and meta-analysis of randomized outcome trials. J Hypertens. 2020;38:1669–168.
Tsujimoto T, Sugiyama T, Shapiro MF, et al. Risk of cardiovascular events in patients with diabetes mellitus on beta-blockers. Hypertension. 2017;70:103–110.
Droyvold WB, Midthjell K, Nilsen TI, Holmen J. Change in body mass index and its impact on blood pressure: A prospective population study. Int J Obes. 2005; 29(6): 650-655.
How to select correct cuff size for measuring blood pressure. Centre for Child Health, BLK-MAX Superspeciality Hospital. https://blk-pediatric- practice.com/2021/03/14/correct-cuff-size-for-bp/. Accessed October 15, 2023.
Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring. N Engl J Med. 2006;354(22):2368-2374. doi:10.1056/NEJMra060433
Wagner TD, Jones MC, Salgado TM, Dixon DL. Pharmacist’s role in hypertension management: a review of key randomized controlled trials. J Hum Hypertens. 2020;34(7):487-494.
CDC. Pharmacists’ patient care process approach guide. August 27, 2021.
www.cdc.gov/dhdsp/evaluation_resources/guides/pharmacists_patient_ care.htm. Accessed September 25, 2023.
Fantin F, Giani A, Zoico E, Rossi AP, Mazzali G, Zamboni M. Weight Loss and Hypertension in Obese Subjects. Nutrients. 2019;11(7):1667. Published 2019 Jul 21. doi:10.3390/nu11071667
Cohen JB. Hypertension in Obesity and the Impact of Weight Loss. Curr Cardiol Rep. 2017;19(10):98. Published 2017 Aug 24. doi:10.1007/s11886-017-0912-4
Maalouf J, Cogswell ME, Yuan K, et al. Top sources of dietary sodium from birth to age 24 mo, United States, 2003-2010. Am J Clin Nutr. 2015;101(5):1021-1028. doi:10.3945/ajcn.114.099770
American Heart Association. How much sodium should I eat per day? AHA. 2021. https://www.heart.org/en/healthy-living/healthy- eating/eat-smart/sodium/how-much-sodium-should-i-eat-per-day. Accessed September 25, 2023.
Gowrishankar M, Blair B, Rieder MJ. Dietary intake of sodium by children: Why it matters. Paediatr Child Health. 2020;25(1):47-61. doi:10.1093/pch/pxz153
Phillips LCE, Nguyen H, Genge TL, Maddigan WJ. Effectiveness and cost- effectiveness of an intensive and abbreviated individualized smoking cessation program delivered by pharmacists: A pragmatic, mixed- method, randomized trial. Can Pharm J (Ott). 2022;155(6):334-344. Published 2022 Oct 12. doi:10.1177/17151635221128263
Kotsis V, Jordan J, Micic D, et al. Obesity and cardiovascular risk: A call for action from the European Society of Hypertension Working Group of Obesity, Diabetes and the High-risk Patient and European Association for the Study of Obesity: Part A: Mechanisms of obesity induced hypertension, diabetes and dyslipidemia and practice guidelines for treatment. J Hypertens. 2018;36(7):1427-40.
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 203: Chronic Hypertension in Pregnancy. Obstet Gynecol. 2019;133(1):e26-e50. doi:10.1097/AOG.0000000000003020
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.