HOSPICE: UNDERSTANDING AND OPTIMIZING COMFORT CARE
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and currently licensed pharmacist in 3 states. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS. from the University of Connecticut and her PharmD. from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Topic Overview
Medicare hospice regulations and the Consolidated Omnibus Reconciliation Act (COBRA) of 1985 created a permanent federal hospice benefit. The word hospice is often misunderstood and is frequently associated with imminent death. Hospice emphasizes quality of life, focuses on the patient and family wishes, and eases distress approximately six months before death. Hospice provides a wide range of treatments and services related to a terminal illness at no out-of-pocket cost to the patient or family. Hospice care prioritizes comfort, emotional and spiritual needs, and minimizing pain and suffering. The number of hospice agencies has increased over the years. Hospice care management includes healthcare providers with clinical expertise in advanced illness and end-of-life care. Pharmacy team members are ideally positioned to provide diverse services in hospice care, including symptom management, pharmacotherapy, and support aspects of transition of care.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-109-H01-P
Pharmacy Technician 0669-0000-23-110-H01-T
Credits: 1 hour of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $4.99
Estimated time to complete activity: 1 hour, including Course Test and course evaluation
Release Date: July 22, 2023 Expiration Date: July 22, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From July 22, 2023, through July 22, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Understand the definition of palliative care and hospice care
Identify the basic services of hospice care
Describe Inter-professional Collaborative Approach to providing hospice care
Identify medications provided in a hospice patient Comfort Care kit
Disclosures
The following individuals were involved in developing this activity: Pamela Sardo, PharmD, BS. Pamela Sardo, PharmD, BS, was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Hospice care today is largely a government healthcare system. Patients who meet specific criteria are eligible for this benefit. Hospice care is not a new concept, but the philosophy behind this type of care is changing. Hospice care is also advancing with new technologies. This course will examine the history of hospice care, the distinction between hospice care and palliative care, the current state of hospice care in the United States, the pharmacy team interface, advancements in care, and the technologies now used or being considered in hospice care.
The History of Hospice
The philosophy of caring for persons with terminal illnesses was established hundreds of years ago. In the 11th century, the Roman Catholics adopted the concept of hospice as a place of hospitality for the sick and dying.1 The first hospice was believed to have been established during the Crusades, and hospices were reportedly widespread in the Middle Ages.1 The word ‘hospice’ derives from the Latin word hospes, which means ‘guest’ and ‘host.’1
A British physician named Dame Cicely Saunders worked with terminally ill patients in the London area beginning in 1948. In 1963, she introduced the idea of specialized care for the dying, which centered on palliative care rather than treatments to cure.1 In 1969, Dr. Elisabeth Kubler-Ross, a psychiatrist and pioneer in near-death studies, emphasized the benefits of home care over treatment in an institutional setting for terminally ill patients.1 She argued that everyone deserves the right to decide on end-of-life care.1
The first hospice in the United States was the Connecticut Hospice, founded in 1974 with a National Cancer Institute grant.1 In 1986, the United States Congress passed the Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985. It stated that terminally ill patients in nursing facilities could elect Medicare hospice care.2 COBRA also allowed states to add a hospice benefit to their Medicaid programs.2
In 2004, more than 1 million Americans were reported to have received hospice services.3 In the same year, The Diana, Princess of Wales Memorial Fund, and the Franklin Mint made a $3.35 million gift to National Hospice and Palliative Care Organization (NHPCO) to promote better end-of-life care.3 In 2018, the Medicare Patient Access to Hospice Act was signed by President Donald Trump.4
Distinctions Between Hospice and Palliative Care
For many years, hospice and palliative care were not well distinguished. The word palliative care is derived from the Latin words for ‘cover’ or ‘cloak.’5 There is a consensus definition that palliative care is the holistic care of individuals of all ages with profound health-related suffering due to severe illness. This concept is especially relevant for those populations near the end of life (EOL).6 These programs aim to improve the quality of life of patients, their families, and their caregivers.

The terms palliative care and hospice should not be used interchangeably. Palliative care is considered a model of care or an approach to care.7 Hospice care is applied to specific programs or services that provide specialist care. Hospice is a focused component of palliative care, with specific eligibility requirements from the Medicare hospice benefit. Hospice is usually provided in the patient’s home to allow comfort and the presence of loved
ones. Table 1 clarifies particular distinctions between palliative care and hospice.
Table 1
Palliative Care and Hospice Distinctions9
| Question | Palliative Care | Hospice |
| Who is treated? | Anyone with a serious illness | Anyone with a serious illness whom a doctor believes only has a short time to live, often <6 months |
| Will Medicare pay? | It depends on the benefit design and treatment plan | Yes, it pays for hospice charges associated with the terminal illness |
| Does private insurance pay? | It depends on the plan | It depends on the plan |
| How long will the patient be cared for? | This depends on what care is needed and the insurance plan | As long as the hospice criteria are met, and there is a life expectancy of months, not years |
| Where will the patient receive care? | Home Assisted living Nursing home Hospital Palliative care clinic | Home Assisted living Nursing home Hospital Hospice facility |
The Current State of Hospice Care
Hospice is a large government-supported and government-regulated healthcare system.11 It is a government entitlement for eligible patients and involves care management by clinical experts with EOL care training. Hospice
is also a managed care benefit with a capitated payment to agencies that accept full risk management of a terminal illness.11
As the Medicare program struggles to control expenditures, there is an increased focus on opportunities to manage patient populations more efficiently and at a lower cost. A major source of expense for the Medicare program occurs in beneficiaries at the EOL. Estimates of the percentage of Medicare costs that arise from patients in the last year of life may range from 13% to 25%.11 Patients at the EOL are considered an appropriate population for risk-sharing cost management by Medicare. Greater use of hospice care offers the possibility of expense reduction to the Medicare program while improving quality of life outcomes.11
A current unmet need is that fewer than 25% of Americans die at home, despite an overwhelming desire to do so. For those who enter hospice care, over 75% of patients in hospice die at home.8
Of all the Medicare beneficiaries who died in 2014, 46 percent used hospice. This percentage has more than doubled since 2000, when only 21 percent of beneficiaries used hospice.12 The rate of hospice use increases with age, with the highest rate existing among decedents ages 85 and over.12 Hospice use is also higher among women than men and among white beneficiaries than beneficiaries of other races/ethnicities.13 More research is needed to understand the reasons for the disparities better.
Despite the increase in participation, why are not all patients diagnosed with a terminal illness quickly referred to hospice? One reason is the lack of resources. Some rural geographies may have fewer trained professionals or less training in addressing terminal illnesses beyond oncology.14 A second reason is a lack of awareness of resources. Some hospice centers are well integrated, others are stand-alone institutions, and integration may be more fragmented. In addition, medical school residents infrequently have access to palliative care rotations to learn about hospice.14 A third reason is ignorance regarding what palliative care is. A fourth reason is a reluctance to refer.
Physicians may fear upsetting patients and do not want to abandon them. Some professionals do not understand the benefits of referral. A fifth reason is the reluctance of the patient and/or family to be referred. Sometimes, there is a cultural reason, and sometimes a perception that hospice means immediate demise causes delayed participation.14
One way to identify patients who could qualify for hospice and encourage participation is knowing how to introduce people to hospice. When introducing hospice to patients, families, or clinicians, researchers have proposed that a ‘surprise question’ can be asked.10 This question has been used to identify patients at high risk of death who might benefit from hospice services when the response is ‘no.’10 The surprise question inquires: “Would I be surprised if this patient died in the next 12 months?” This question may help identify patients who are eligible for covered hospice services.
Hospice Eligibility and Covered Services
To qualify for hospice, a physician must confirm that the patient is expected to die within six months if the illness is normal. If a Medicare patient lives longer than six months, hospice coverage may continue if the physician and the hospice team re-certify the eligibility criteria.12 A decline in a patient’s clinical status requires an ongoing assessment of the patient’s condition over time. Baseline data is established on admission to hospice, or data entry extracts existing information from records. The change in patient status is also considered to be part of the documentation of the patient’s clinical variables. The payers of the hospice benefit require that the clinical variables, which lead to the conclusion of a six-month or less life expectancy, should be documented in the clinical record.15
These changes in clinical variables include worsening clinical status, symptoms, signs, and laboratory results. Clinical findings may include recurrent or intractable infections, dysphagia (trouble swallowing) leading to recurrent aspiration, or other factors such as inadequate oral nutrition intake.15
When a patient’s health declines, difficult-to-treat symptoms can appear. Symptoms may include dyspnea (trouble breathing), nausea, vomiting, diarrhea, or poor responsiveness to treatment.15 Pain requiring increasing doses of analgesics may be identified. Patients may present with a decline in systolic blood pressure, ascites (abdominal fluid), weakness, or a change in level of consciousness. An increase in emergency room visits, hospitalizations, or increase in physician visits related to the primary hospice diagnosis may occur.14 Assistance with activities of daily living may be required, and other issues, such as pressure ulcers, may be present.15 These factors require a coordinated plan of care (POC).
Comorbidities are considered when determining a decision to begin hospice. These comorbidities, and their severity, can impact life expectancy. These may include cancer, chronic obstructive pulmonary disease, congestive heart failure, diabetes mellitus, neurologic disease (such as stroke or Parkinson’s), or renal failure, among others.15 The following case exemplifies the impact of comorbidities on determining life expectancy. Consider an 85- year-old male dialysis patient with diabetes. The patient contracted SARS- CoV-2. Dialysis was briefly suspended during COVID treatment. The patient survived COVID, but he experienced a state of shock after restarting dialysis. The shock symptoms included cold, pale skin, and mottling red blotches all over the body. This led the healthcare team to cease further dialysis. Thereafter, the team was guided by an assessment of the patient, concluding that the patient was eligible for hospice.
For terminally ill individuals who no longer continue to pursue curative treatments, a hospice benefit covers many services to address the needs associated with the conditions described above. The hospice benefit includes nursing care, counseling, palliative medications, and up to five days of respite care to assist family caregivers.12 Hospice care is most often provided in patients’ homes.12 Medicare patients who elect the hospice benefit have little to no cost-sharing liabilities for most hospice services associated with the causative terminal illness.12 The Hospice Benefit Provisions figure below illustrates the broad range of hospice services.
Hospice Benefit Provisions16
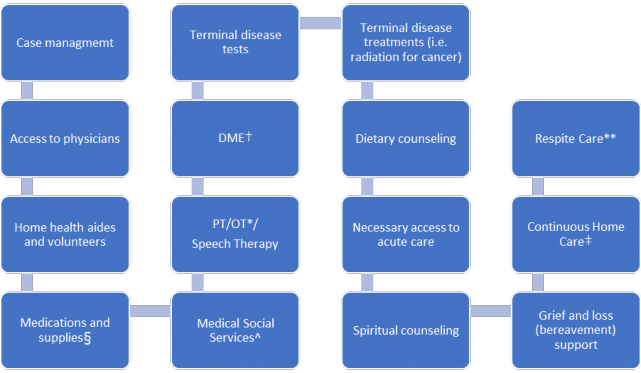
*PT/OT- physical therapy, occupational therapy
^Medical Social Services- to access community services
†DME- durable medical equipment (i.e., hospital bed, mucous suction device, bed wedge)
‡Continuous Home Care (nurse ≥8 hours/day)
**Respite Care- Admit a patient to a facility for up to 5 days for caregiver rest
§Bedpads, adult diapers, wipes
In hospice, individualized patient goals are identified, and the POC is written to include all services necessary to manage the terminal illness. Hospice staff also identify and document patient needs that are unrelated to the terminal illness, and document who is addressing them. Hospice patients generally receive a few visits every week. Visit frequency and duration may depend on the patient’s condition, staffing, or other resources. During the home visits, the hospice staff develops a relationship with the patient, contributing to patient comfort.
Medicare requires the hospice POC to include interventions to manage pain and symptoms and maintain a detailed statement of the scope and frequency of services.17 The POC also includes measurable outcomes expected, necessary drugs, medical supplies, and appliances. Documentation
of the patient’s or representative’s level of understanding, involvement, and agreement with the POC is also included in the POC.17
Inter-professional Collaborative Approach to Hospice Care
Hospice uses an inter-professional collaborative approach so the Interdisciplinary Group (IDG), physician, patient, and primary caregiver will identify patient and family goals. The IDG team members support and manage the physical, medical, psychosocial, emotional, and spiritual needs of hospice patients and families.17 The IDG sets up the POC when an individual chooses hospice and frequently updates the POC. The IDG also offers a bereavement POC and supportive services to the caregiver and family for 1 year after the death of the hospice patient.17 Families may also supplement hospice services with care from other sources.
Many hospice participants do not have a primary caregiver. They may live alone without family or friends nearby. Plans can usually be created so the individual does not have to relocate. Hospice volunteers can provide meals, light housekeeping, and company to those living alone.
The POC is overseen by a Registered Nurse (RN) coordinator. Each patient is assigned an RN.17 The RN Coordinator ensures that the POC is updated, individualized, and relevant to the needs of the patient and family by continuously assessing each patient’s and family’s needs. The POC also documents and revises patient care goals and objectives.17 The RN communicates changes in services and facilitates the exchange of information.
Depending on the goals, medical requirements, and staffing, the IDG may include specialists, or roles may be combined:17,18
The hospice medical director is responsible for the management of the terminal illness and any related conditions
The primary physician or nurse practitioner may continue to be involved in hospice care
The registered nurse (RN) patient care coordinator visits regularly and makes ongoing assessments of physical, emotional, and spiritual symptoms
The hospice visiting nurse may assist with medication management, dressing changes, other physical care, and emotional support
Hospice aide provides personal care, homemaking services, and other supportive services
The pharmacist is dedicated to hospice, regularly reviews medications, and provides input to manage symptoms to improve quality of life
The social worker meets with the patient and family to assess financial issues, emotional stress, the safety of the patient’s environment, and coping skills
The bereavement coordinator provides follow-up, support, and grief education for loved ones throughout the 13 months following the patient’s death
Volunteers are screened and trained by hospice staff to provide a variety of services, including companionship and a supportive presence
The chaplain or spiritual care coordinator respects individual beliefs and practices and is available for spiritual, religious support or both
Other professionals are available based on your needs, including physical, occupational, speech therapists, or dietitians

Dialogue and documentation are essential to establish and maintain an accurate picture of the patient’s functional status. An extensive medication review occurs at hospice IDG meetings. This allows the hospice pharmacist to identify and recommend changes in nonessential or overly burdensome medication therapy. The pharmacist may recommend the addition of
medications for symptom management and comfort.19 The hospice pharmacist may also contribute to developing medication-use policies and procedures to support compliance with federal and state regulations and best practices.19 The hospice pharmacist will often participate in symptom assessment, laboratory monitoring, medication management, and prescribing in states that grant prescriptive authority to pharmacists through collaborative practice agreements (CPAs).19
Occasionally, a patient’s condition will improve beyond a brief period resulting in an expected life expectancy that extends beyond six months. Hospice may discharge a patient in this case, but the family can reapply if the condition changes again because the Medicare hospice benefit does not expire.20
Comfort Care Kits
When individuals join hospice, medications that are no longer essential are discontinued. A statin for elevated cholesterol will be discontinued. A cream or biologic for psoriasis will be discontinued. During hospice, different medications will be provided for the patient. As symptoms appear, such as anxiety, nausea, pain, or increased secretions, an emergency hospice kit eliminates the need to wait for critical medications to be delivered.21 These kits are prepared early in the hospice care process and delivered proactively to the patient’s location, generally before they are needed. While the medicines included in the kit may vary depending on one’s specific health, certain types of medication are frequently included. These kits are often referred to as comfort care kits.21
The hospice nurse, or the hospice pharmacist, explains the purpose and proper administration of each medication in the kit. It is efficient and easier for a family and patient to receive the kit upon joining hospice rather than wait for symptoms to appear, which may be in the context of a stressful medical emergency.21 Some of the medications have off-label uses in hospice care. The Food and Drug Administration has not reviewed or determined comprehensive safety and efficacy in these limited off-label uses. The full
prescribing information should always be reviewed for safety and efficacy details.

The following medications may be found in a hospice comfort kit, along with the symptoms they may treat:21
Morphine Liquid is a narcotic that is used to treat pain and in hospice, has an off-label use for shortness of breath
Lorazepam is a medication used to treat anxiety, and in hospice, has an off-label use in nausea and insomnia
Drops of Atropine are used to treat wet respirations, which, at the end of life, may be referred to as death rattles
Haloperidol is an antipsychotic that is effective for treating agitation and terminal restlessness in hospice
Prochlorperazine is available in pill or rectal suppository form and is used to treat nausea and vomiting
Promethazine is an antiemetic to treat nausea and vomiting
Bisacodyl rectal suppositories are for symptoms of constipation
Senna is a laxative made from plants and is used to treat constipation
Saline laxative rectal enema is for constipation when other treatments are ineffective
Additional medications may be added based on the hospice diagnosis. For instance, if a patient with a brain tumor is at risk of seizures, the comfort kit may include diazepam rectal suppositories. Families should always keep hospice medications and all other medications out of reach of children. Hospice medications should be kept in a secure location to minimize the risk of diversion.
Educational Pearls and Resources
Patient time under hospice care varies. Hospice is most beneficial when the range of services is provided for a month or more. After experiencing the quality and comfort of hospice teams and services, families who have utilized hospice often say they wish they had requested hospice earlier in the illness process.
In many cases, the family members of hospice patients continue to provide day-to-day care. Families in hospice can rely on assistance and advice 24 hours a day 7 days a week from the hospice company staff. Because of the design of the hospice benefit, when a crisis or concern arises while receiving care, the hospice staff should be the first call for help. A hospice nurse will visit in person if a crisis cannot be handled over the phone.
When a pharmacy team knows a family well, or the pharmacist learns of a health status change to a terminal illness from a provider, sensitive and thoughtful conversations about hospice may be possible. Delicately, pharmacy team members can encourage patients, family members, friends, or healthcare providers to contact a hospice agency to inquire whether hospice may be appropriate for an individual with a terminal illness and poor prognosis.
Patient-facing conversations can allow a pharmacy technician to inquire about over-the-counter drugs and supplements during a transition to hospice care. Pharmacy technicians are familiar with dosage forms, strengths, and usual dosing schedules of a wide range of medications for hospice patients. Pharmacy technicians are ideally positioned to optimize workflow in a busy
setting and ensure accurate processing of the comfort kits. Pharmacy technicians can answer questions from hospice patients and families about medication storage and can apply auxiliary labels for items that should be refrigerated in the kits. Pharmacy technicians with hospice roles understand the unique aspects of hospice.
Families can be assured that hospice providers do not accelerate the dying process. The providers also cannot cure terminal illnesses. Hospice strives to maximize the patient’s quality of life. Table 2 provides some hospice resources for clinicians or patients.
Table 2
Select Hospice Resources
| Resource | Contact |
CaringInfo National Hospice and Palliative Care Organization | 800-658-8898 |
| Hospice Foundation of America | 800-854-3402
https://hospicefoundation.org/End-of- Life-Support-and-Resources
https://hospicefoundation.org/End-of- Life-Support-and-Resources/Coping- with-Terminal-Illness/How-to-Choose |
| Medicare | https://www.medicare.gov/what- medicare-covers/what-part-a- covers/how-hospice-works |
| Healthcare Compare Hospice Compare | https://healthcarecomps.com/hospice Locating a hospice provider |
Trends in Hospice Care
The future of hospice care is advancing rapidly. In ClinicalTrials.gov, there are over 800 current studies on the topic. One study is incorporating virtual reality to assess pain control in hospice care.22 Another study is utilizing aromatherapy in hospice protocols.23 An additional clinical trial will assess bias and disparities in end-of-life care.24 Pharmacy team members in a broad range of practice settings are optimally positioned to provide support, education, or in-services to teach healthcare professionals or the community about hospice. Pharmacy team involvement in hospice includes providing broad essential services to hospice care teams, direct or indirect patient care, and medication therapy management. Pharmacy teams can also provide transition of care support and symptom management.
Summary
The philosophy of caring for persons with a terminal illness is hundreds of years old. In the United States, hospice began within private healthcare institutions, but today it is largely a federal government healthcare system.
The terms palliative care and hospice should not be used interchangeably. Palliative care is an approach or model of care, whereas hospice care is applied to a specific program or service that provides care by a specialist. Hospice is a focused component of palliative care, with specific eligibility requirements from the Medicare hospice benefit.
A current unmet need in hospice care is that fewer than 25% of Americans die at home, despite an overwhelming desire to do so. This can be improved through an inter-professional collaborative approach to hospice care that can identify a patient’s eligibility for care. It also provides the patient with the needed information to access care.
Pharmacotherapy and comfort care kits support optimal patient outcomes. Collaborative practice opportunities have also strengthened the working relationship between pharmacists and multidisciplinary hospice care
practitioners. Pharmacy practice within a hospice team setting is unique and can be very rewarding.
New technologies, such as the use of virtual reality, and new protocols in treatment, such as aromatherapy, may also advance the use and effectiveness of hospice care.
Course Test
Which statements are most correct regarding palliative care and hospice care?
Hospice care is a model of care or an approach to care, and palliative care is applied to specific programs
Hospice treats anyone with a serious illness, and palliative care treats those with a life expectancy <6 months
Hospice is a focused component of palliative care, with specific eligibility requirements
Palliative care is a focused component of hospice, and they can be referred to interchangeably
Hospice has developed into
a large government-supported healthcare system without regulations.
a managed care benefit with a fee-for-service agency payment model.
an entitlement program for eligible patients with care management.
a partial risk payment model limited to care for cancer patients.
The more likely reason(s) a terminally ill individual does not enter hospice care may include
a lack of awareness of resources or a reluctance to use hospice care.
providers do not make referrals because they do not want to lose insurance revenues.
because hospice coverage is limited to inpatient care.
a patient’s dietary needs often make hospice impractical.
Which of the following statements about hospice-covered eligibility is FALSE?
A patient can enter hospice and then become ineligible if the family decides to pursue curative treatments
A family can be eligible for hospice services even if a patient is deemed medically ineligible
A patient can remain in hospice if alive after seven months and following hospice IDG reassessment at six-months
An eligible patient stops dialysis and requests an in-home hospital bed and bed pads
Which of the following hospice benefits or services are covered by Medicare?
Access to individualized care by a hospice nurse
Access to medications and 50 days of respite
DME and oversight by community primary care
One year of occupational and physical therapy
Which role is correctly matched with the hospice professional?
The hospice visiting nurse may assist with medication management, dressing changes, other physical care, and emotional support
The chaplain is dedicated to hospice, regularly reviews medications, and provides input to manage symptoms to improve quality of life
The social worker is responsible for managing the terminal illness and any related conditions
The pharmacist provides follow-up, support, and grief education for loved ones throughout the 13 months following the patient’s death
Which is the expected use for morphine in a comfort care kit?
As an antiemetic to treat nausea and vomiting
To treat wet respirations, known as death rattles
As a laxative used to treat constipation
To treat pain or off-label for shortness of breath
Which option below is NOT a possible role of a hospice pharmacist?
To identify and recommend changes in nonessential medications
To manage and assess the physical, financial, and psychosocial needs of the hospice patient
To recommend adding medications for symptom management and comfort
To develop medication-use policies and procedures to support federal and state compliance
What is the purpose of a hospice comfort care kit?
For every hospice patient to have identical medications regardless of specific health
To contain financial brochures and stress-relieving squeeze ball for the social worker to explain
To contain ongoing maintenance treatments for conditions such as elevated cholesterol or psoriasis
To eliminate the need to wait for critical medications to be delivered as symptoms arise
What is the purpose of lorazepam in the comfort care kit?
To crush into a paste to apply to the chest if a patient has dysphagia
To treat anxiety, or as an off-label drug for nausea and insomnia
To use as an antipsychotic for treating hallucinations in hospice
To place in a rectal enema if the patient cannot swallow
References
A brief history of hospice. Understand Hospice. Hospice of Holland. 2023. https://understandhospice.org/brief-history-hospice/. Accessed
June 16, 2023.
Gage B, Miller S, Coppole K, et al. Important questions for hospice in the next century. Office of the Assistant Secretary for Planning and Evaluation. Health and Human Services. February 29, 2000. https://aspe.hhs.gov/reports/important-questions-hospice-next- century-1. Accessed June 16, 2023
History of Hospice. NHPCO. 2023. https://www.nhpco.org/hospice-care- overview/history-of-hospice/. Accessed June 16, 2023.
H.R. 1284- Medicare Patient Access to Hospice Act of 2017. Congress.gov. February 2018. https://www.congress.gov/bill/115th- congress/house-bill/1284/actions. Accessed June 16, 2023.
Palliative Care. Cleveland Clinic. April 22, 2022. https://my.clevelandclinic.org/health/articles/22850-palliative-care. Accessed June 17, 2023.
Radbruch L, De Lima L, Knaul F, et al. Redefining Palliative Care-A New Consensus-Based Definition. J Pain Symptom Manage. 2020;60(4):754- 764. doi: 10.1016/j.jpainsymman.2020.04.027
McAteer R, Wellbery C. Palliative care: benefits, barriers, and best practices. Am Fam Physician. 2013;88(12):807-813.
National Hospice and palliative Care Organization. NHPCO Facts and Figures. 2022 edition. NHPCO. Updated December 2022. https://www.nhpco.org/wp-content/uploads/NHPCO-Facts-Figures- 2022.pdf. Accessed June 16, 2023.
National Hospice and palliative Care Organization. Explanation of Palliative Care. NHPCO. Updated 2023. www.nhpco.org/palliativecare/explanation-of-palliative-care. Accessed June 16, 2023.
Downar J, Goldman R, Pinto R, Englesakis M, Adhikari NK. The "surprise question" for predicting death in seriously ill patients: a systematic review and meta-analysis. CMAJ. 2017;189(13):E484-E493. doi: 10.1503/cmaj.160775
Duncan I, Ahmed T, Dove H, Maxwell TL. Medicare Cost at End of Life. Am J Hosp Palliat Care. 2019;36(8):705-710. doi:10.1177/1049909119836204
Kaiser Family Foundation. 10 FAQs: Medicare’s role in end-of-life care.
KFF. September 26, 2016. https://www.kff.org/medicare/fact-sheet/10-
faqs-medicares-role-in-end-of-life-care/. Accessed June 16, 2023.
Ornstein KA, Roth DL, Huang J,et al. Evaluation of Racial Disparities in Hospice Use and End-of-Life Treatment Intensity in the REGARDS Cohort. JAMA Netw Open. 2020;3(8):e2014639. doi: 10.1001/jamanetworkopen.2020.14639
Hawley P. Barriers to Access to Palliative Care. Palliat Care. 2017;10:1178224216688887. Published 2017 Feb 20. doi:10.1177/1178224216688887
Centers for Medicare & Medicaid Services. Hospice determining terminal status. Medicare Coverage Database. CMS.gov. Updated June 30, 2022. https://www.cms.gov/medicare-coverage- database/view/lcd.aspx?LCDId=34538. Accessed June 17, 2023.
Centers for Medicare & Medicaid Services. Hospice. CMS.gov. 2023. https://www.cms.gov/Medicare/Medicare-Fee-for-Service- Payment/Hospice. Accessed June 19, 2023.
Centers for Medicare & Medicaid Services. Creating an effective hospice plan of care. Medicare Learning Network. CMS.gov. May10,2023. https://www.cms.gov/files/document/creating-effective-hospice-plan- care.pdf. Accessed June 16, 2023.
Mayo Clinic. Hospice. Overview. Mayo Clinic. May 17, 2023. https://www.mayoclinic.org/departments- centers/hospice/sections/overview/ovc-20481745. Accessed June 16, 2023.
Herndon CM, Nee D, Atayee RS, et al. ASHP Guidelines on the Pharmacist's Role in Palliative and Hospice Care. Am J Health Syst Pharm. 2016;73(17):1351-67. doi: 10.2146/ajhp160244
Hospice Foundation of America. What is hospice? HFA. 2023. https://hospicefoundation.org/Hospice-Care/Hospice-Services. Accessed June 19, 2023.
Ali H. Hospice Comfort Kit. Melodia. 2021. https://www.melodiacare.com/hospice-comfort-kit/. Accessed June 16, 2023.
Far Eastern Memorial Hospital. Natural Virtual Reality in the Application of Hospice Care. ClinicalTrials.gov identifier: NCT04522440. Updated August 16, 2022. https://clinicaltrials.gov/study/NCT04522440?cond=Hospice&term=virt ual%20pain&rank=1. Accessed July 15, 2023.
Blanton T, The University of Texas Health Science Center, Houston. Aromatherapy Protocol for Pain Reduction in Hospice Patients. ClinicalTrials.gov identifier: NCT05617144. Updated January 4, 2023. https://clinicaltrials.gov/study/NCT05617144?cond=Hospice&term=aro matherapy&rank=1. Accessed July 15, 2023.
Chuang E, Montefiore Medical Center. ATargeting Bias to Reduce Disparities in End of Life Care (BRiDgE). ClinicalTrials.gov identifier: NCT05165888. Updated May 6, 2023.
https://clinicaltrials.gov/study/NCT05165888?cond=Hospice&aggFilters
=status:rec&rank=7. Accessed July 15, 2023.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2023: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.