HEAD LICE: SOLVING ‘NIT-PICKY’ PEDICULUS CAPITIS
Anna Shurtleff Smith, MPH, BSN-RN
Anna Shurtleff Smith is a graduate of the University of North Texas Health Science Center, School of Public Health with a community health focus, and Texas Tech University School of Nursing. She has clinical experience in both inpatient and outpatient settings. Anna is passionate about patient education, health literacy, and health communications. When not writing, she can be found enjoying the outdoors and enjoying family time.
Pamela Sardo, PharmD, BS
Pamela Sardo, PharmD, BS, is a freelance medical writer and currently licensed pharmacist in 3 states. She is the founder and principal at Sardo Solutions in Texas. Pam received her BS from the University of Connecticut and her PharmD from the University of Rhode Island. Pam’s career spans many years in retail, clinics, hospitals, long-term care, Veterans Affairs, and managed health care responsibilities across a broad range of therapeutic classes and disease states.
Topic Overview
Infestation with head lice is a common problem. The stigma associated with head lice (pediculus humanus capitis) often results in significant social and financial burdens. Healthcare professionals often collaborate regarding head lice to educate the public, enhancing self-care opportunities and dispelling prevalent myths about head lice. Comprehensive training is essential to equip these professionals with the knowledge of proper diagnosis, prevention of misdiagnosis, and treatment protocols, which are vital for addressing patient needs and preventing re-infestation. The topic will discuss accurately differentiating head lice from other scalp conditions. Approaches to precise diagnosis and treatment will be discussed, and interprofessional team communication will be mentioned. This module will also cover diverse strategies for reassuring patients, mitigating resistance, and providing attendees with up-to-date information to combat head lice infestations.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-131-H01-P
Pharmacy Technician 0669-0000-24-132-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Course Test and course evaluation
Release Date: September 23, 2024 Expiration Date: September 23, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
How to Earn Credit: From September 23, 2024, through September 23, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Identify and Dispel at least three common myths about head lice
Distinguish head lice from other scalp conditions
Summarize current head lice treatments
Formulate a collaborative multidisciplinary plan of care for a patient with head lice.
Disclosures
The following individuals were involved in developing this activity: Anna S. Smith, MPH, BSN-RN, and Pamela Sardo, PharmD, BS. Anna S. Smith and Pamela Sardo have no conflicts of interest or financial relationships regarding this subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Head Lice: Solving 'Nit-Picky' Pediculus Capitis Introduction
Head louse infestations have existed in the human population for thousands of years. This course focuses on improving knowledge by identifying and dispelling common myths about head lice, distinguishing head lice from other scalp conditions, discussing over-the-counter and FDA- approved treatments, and recognizing resistance management strategies for head lice.
Prevalence of Head Louse Infestations
Human head louse infestations have existed for at least 10,000 years.1 Each year, $1 billion is estimated to be spent treating head lice in the United States.2 Head lice infestations can impact individuals physically, financially, and emotionally.
The life cycle of head lice begins with the egg (“nit”) stage, followed by nymphal stages, and then the adult stage.1 The lifecycle of head lice can be observed in Figure 1 below.1 The types of lice are depicted in Figure 2.1
Eggs/Nits
Adults
Nymphs
Figure 1 Lifecycle of Head Lice
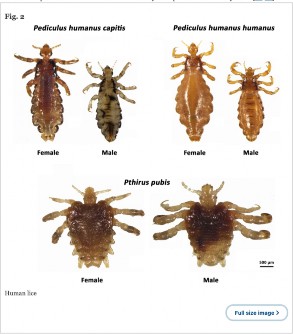
Figure 2 Types of Lice
Myths, Barriers, And Complications Around Head Lice (Pediculus Humanus Capitis)
| Myth | Fact |
| Poor Hygiene Causes Head Lice | Head lice affect anyone, regardless of hygiene habits. |
| Head Lice Can Jump or Fly | Head lice only crawl; transmission is primarily through head-to-head contact. |
| Pets Can Spread Head Lice | Head lice are human-specific and cannot be transferred from pets. |
| Only Children Get Head Lice | Adults can also get head lice, especially in communal settings. |
Table 1 Myths3,4
Myth: Poor Hygiene Causes Head Lice
Head lice are not a sign of poor hygiene or uncleanliness. They can affect anyone, regardless of how often they wash their hair.3,4 Family involvement in effective early treatment is important to reduce the spread of head lice. Due to this poor hygiene myth, if head lice are discovered by families or individuals with this belief, they are less likely to seek out effective early treatment. This can lead to the spread of the head lice to other family members.3,4
Myth: Head Lice Can Jump or Fly
Head lice remain on the person’s hair and scalp: they cannot jump or fly, they can only crawl; and, head lice do not burrow into the skin. Transmission is primarily through direct head-to-head contact. Many individuals can remember being told not to wear hats or brush with another person’s hairbrush for fear of getting head lice. Research has shown that head lice do not spread outside of direct head-to-head contact.1 However, this myth has led to many individuals with a head lice infestation being unfairly isolated from other individuals for fear of spreading head lice.4
Myth: Pets Can Spread Head Lice
Head lice are specific to humans and cannot be transferred between humans and pets.2 3 Belief in this can lead to using treatments for pets on humans to remove the infestation. Veterinarian-formulated medications should NEVER be used on humans.3
Myth: Only Children Get Head Lice
While more common in children, adults can also get head lice, particularly in communal living environments.4
Barriers to Head Lice Treatment and Eradication
There are many barriers to head lice treatment and eradication. Infestations can lead to significant stigma, causing affected individuals, especially children, to be excluded from social activities.4 If head lice are diagnosed in a child or adolescent, confidentiality is important to minimize social stigma.4 Stigma may occur if communication inadvertently reveals the affected individual’s identity. In one study, 25.5% of individuals with pediculosis reported being upset, 19.5% felt shame, 9% feared becoming an outcast, and 12.5% feared being mocked.5
.
Misconceptions about head lice and ineffective home remedies can hinder proper treatment and prevention efforts. Caregivers and non-clinicians frequently make the diagnosis of head lice.4 The availability of safe and effective over-the-counter (OTC) pediculicides often removes medical providers from the treatment process.4 Overcoming misconceptions with increased clinician involvement in diagnosis and treatment can reduce the potential for misidentification resulting in improper use of pediculicides or resistance to products.4 Medical providers are optimally positioned to address head lice questions, including requests for alternative approaches that often lack proof of efficacy and safety data.
Misdiagnosis is a barrier and one cause of treatment failure.6 A misdiagnosed itchy rash may be treated with a topically administered steroid, for example, which leads to crusting and diffuse erythema, but no eradication of the head lice.6
Several studies have found that, over the past 40 years, the clinical effectiveness of permethrin and pyrethrins has declined from nearly 100% to as low as 25% in some communities.4 Researchers are exploring the genetics of head lice to determine whether the findings might predict resistance.4
Barriers to access to treatment may be a factor hindering eradication. Limited access to effective treatments and healthcare resources has been reported in low-income and communal settings. War and natural disasters
displace populations and disrupt infrastructure and access to medical care.7 These populations may include refugee populations. Infestations are common when there are barriers to basic hygiene, crowded living, or travel conditions. Infestations also can occur in individuals lacking access to regular bathing or laundering.7
Direct and indirect costs for individual patients are important factors to be discussed and considered.4 The economic burden of treatment and missed school or work are often significant. Misdiagnosis and unneeded treatment also are economic burdens to the patient. Treatment failure due to misuse of pediculicides or other agents. Resistance can result in large, unexpected costs.8
Complications from Head Lice Infestation
Not all cases of head lice are without complications. Head lice rashes have been reported, which can result in secondary infection with Staphylococcus aureus or streptococci. Hairs can become encrusted and stuck together, and lymph nodes may swell.9 An additional complication is that head lice may appear in eyelashes and need to be eliminated.10
When an infestation is significant,9 pediculosis is a risk factor for iron- deficiency anemia in populations that lack access to regular healthcare.10 One published case reported a 12-year-old died from an apparent cardiac arrest. The secondary cause of death was listed as severe iron deficiency anemia that had resulted from a massive head lice infestation. The parents were arrested and charged with second-degree murder in addition to cruelty to children in the second-degree.11 Forensic teams have discussed that head lice infestations may serve, in limited situations with other evidence, as a sign of conditions such as mental illness, abuse, neglect, and even rape.11
Medical Team Approaches to Preventing Infestation Prevention Through Education
Educating families and individuals on the importance of keeping head- to-head contact to the minimum is essential to primary prevention.4,12 However, primary prevention is unlikely to occur. Secondary prevention measures are cleaning bedding, clothing, and personal items that were in contact with the head of the person with infestation two days before treatment in hot water (>130°F) to kill head louse and nits. Do not use pediculicide spray, as any exhaustive cleaning measures are unnecessary.4
Clinical Manifestations
Knowing the clinical manifestations and acting early is an important part of preventing infestation. Itching due to the allergic reaction from the louse’s saliva during the initial infestation is typically the first clinical manifestation. During the initial infestation, this can take four to six weeks; however, in subsequent infestations, the itching can be triggered more quickly, usually within two days. Additional clinical manifestations are an itchy scalp, scratching, crawling sensations, seeing louse, finding lice eggs, swollen lymph nodes in the neck, and pink eye.13
Carefully using a louse comb with sharp teeth is the most effective way to remove the lice and nits. Using a handheld magnification or microscope to distinguish what the item in the hair might be. That differential diagnosis must be explored through the magnification and microscope to avoid misdiagnosis. The most common misdiagnoses are scalp conditions like dandruff or hair debris.7,13
Differential Diagnosis
Identifying the type of lice and its characteristics and differentiating between head lice and body lice are essential to making a proper diagnosis. Proper identification of the adult head louse is important. They are “2–3 mm
in length, elongated, flattened dorsoventrally and without wings.”14 Head louse/lice remain their entire lifecycle on the host. This differs from body lice whose lifecycle is mostly in clothing and bedding.1 Frequent head-to-head contact is necessary for the spread of these obligate (cannot survive without a host) ectoparasites (a parasite that lives outside their host).15
Louse types, characteristics, and potential impact are described in Table
2. Table 3 summarizes the differences between head lice and body lice.16-18
Table 2
Characteristics and Potential Impact of Pediculus
| Type of Lice | Characteristics | Impact |
| Head Lice (Pediculus humanus capitis)16 | Found on scalp and neck; spread through head-to- head contact; causes itching. | Do not transmit diseases; primarily a nuisance. |
| Body Lice (Pediculus | Reside in clothing seams; | Transmit diseases like |
| humanus corporis)17 | known vector for diseases; common in | typhus, trench fever, relapsing fever; can be |
| unsanitary conditions. | severe in crowded | |
| settings (e.g. war, civil | ||
| unrest and natural | ||
| disasters). | ||
| Pubic Lice (Pthirus | Infest pubic hair; | Do not transmit |
| pubis)18 | primarily spread through sexual contact; causes | diseases; associated with sexual health issues. |
| itching. |
*Note: Lice listed above are NOT public health-required notifiable conditions.
Table 316
Differentiation Between Head and Body Louse
| Characteristic | Head louse | Body louse |
| Abdominal indention | More obvious | Less obvious |
| Antenna shape | Shorter and thicker | Longer and thinner |
| 3rd antennal segment | As long as wide | Slightly longer than wide |
| Color (not always reliable) | Darker | Lighter |
| Oviposition site | Base of the hair | On clothing fibers |
| Primarily found | On human head | On clothing |
Treatments for Head Lice Infestation
Most treatments focus on the adult and nymph stages; however, new research has been focusing on ovicidal (egg/nits) drugs in the past few years.19,20 Treatments include the following:
FDA-Approved Pediculicides: Using approved treatments such as permethrin, pyrethrins, and ivermectin, following specific application guidelines.20,21
Manual Removal: Combining chemical treatments with manual removal of nits using fine-toothed combs.14,20
Alternative Treatments: Considering non-chemical treatments like dimethicone or occlusive agents for those who prefer or require them.20
Treatment of Contacts: Treating close contacts of infested individuals to prevent reinfestation.14
Monitoring for Resistance: Being aware of and testing for resistance to common treatments and switching to alternative treatments if necessary.14,20
Available treatments for head lice, dosage, administration, mechanism of action, limitations of use, and select common adverse effects are summarized in Table 4.4
Table 44,6,10,23-28
Treatments for Head Lice
| Agent | Dosing and Administration* | Mechanism of Action | Common Adverse Events or Limitations |
| First-Line Treatments | |||
Pyrethrins (with piperonyl butoxide, shampoo) | Wash off after 10 minutes and repeat in 7-10 days Recommended for ≥24 months | Sodium channel blocker, neurotoxic, leads to paralysis and death of head lice | Local irritation, allergy to ingredients |
Permethrin 1% Lotion
cream rinse | Lotion is applied to the hair and scalp and left on for 10 minutes to approximately 8 hours, usually overnight, depending on product Wash off after 10 minutes, repeat after 7-10 days Recommended for patients aged ≥2 months, and pregnant females | Synthetic, similar to pyrethrins, sodium channel blocker | Local irritation, allergy, evidence of developing resistance |
| Second-Line Treatments | |||
| Malathion 0.5% lotion | Wash off after 8- 12 hours Recommended for ≥6 years | Organophosphate; Acetylcholinesterase inhibitor, leads to spastic paralysis and death of head lice | Scalp dryness, local irritation, dandruff, chemical conjunctivitis if contact with eyes, unappealing odor |
Ivermectin 0.5% lotion
3 mg tablets | Use only the amount needed to completely cover the hair and scalp, leave on for 10 minutes and rinse with only water Recommended for ≥6 months Oral: 200 µg/kg, repeat after 7 days. Recommended for any age if weight ≥15 kg In severe cases, 400 µg/kg, repeat after 7 days | binds chloride ion channels in muscle and nerve cells and results in hyperpolarization of the cell, leading to paralysis and death of head lice | Kills nymphs and lice, but not eggs. Neurotoxicity risk? Not FDA- approved for this use and not labeled for use in children < 15 kg (33 lb) |
| Other Treatments | |||
| Ivermectin 0.5% lotion (topical) | apply to suspected and remove nits (combing, using tweezers). Reapply after 7- 10 days. | Increases chloride in muscle cells, causing hyperpolarization and paralysis of head lice | Burning, scalp irritation, dandruff |
| Benzoyl benzoate Lotion 25% | apply to suspected and remove nits (combing, using tweezers). Reapply after 7- 10 days. | The mechanism is not fully known but is believed to be absorption and impact on the nervous system of head lice | Blisters, crusting, itching |
| Trimethoprim/ sulfamethoxazole | Kills essential bacteria in the lice’s gastrointestinal tract | Blocks two consecutive steps in the biosynthesis of nucleic acids and proteins of head lice | Frequent allergic reactions and treatment failure Not toxic to the louse |
| Fine combs | Physical combing or electronic combing | Manual removal | 38% limited efficacy alone, repeat treatment often required |
Spinosad 0.9% suspension | Apply directly to dry hair and scalp one time only. Leave in for 10 minutes. Recommended for ≥6 months | Provokes hyperexcitation, causing paralysis and death of head lice | Application site erythema and ocular erythema |
Patient Case Study
A healthy, 9-year-old girl presented with abdominal pain and loose stools in the preceding week.29 Laboratory investigations showed significant eosinophilia. Investigating common causes of eosinophilia did not identify a cause. Her vital signs were normal. Her blood pressure was 100/50 mmHg, and her temperature was 98oF).29 A physical examination and history revealed a persistent scalp infestation with head lice. Successful pediculosis management with two applications of an anti-lice lotion coincided with the gradual resolution of eosinophilia without recurrence.29 As no other cause was identified for the increased eosinophils, pediculosis capitis emerged as a possible association because eosinophilia coincided with the diagnosis and
resolved with treatment.29 Eosinophilia could be associated with iron deficiency anemia, which is occasionally observed in adults or children with severe, chronic infestations.29
Treatments for head lice may cause adverse effects on patients, such as itching, burning, dry skin, rash, and ocular irritation.9 Read each package labeling for comprehensive information. Malathion is flammable. The product and treated hair should not be exposed to open flames or electric heat sources, including hair dryers and electric curlers.30 Acute malathion toxicity has occurred with excessive cholinergic activity, increased sweating, salivary and gastric secretions, gastrointestinal and uterine motility, and bradycardia.31
Patient Follow-Up and Support
Medical staff play a crucial role in supporting individuals diagnosed with head lice by addressing both the physical and psychological impacts of infestations.4,32 By providing psychological support, healthcare professionals can help alleviate the anxiety and stress commonly associated with head lice. This support may include counseling services to help individuals and families cope with the stigma and emotional distress of dealing with lice. Additionally, establishing peer support groups in schools and communities can offer affected individuals a platform to share experiences and solutions, fostering a sense of community and understanding. Family counseling sessions can also be beneficial in addressing the impact of lice on family dynamics, ensuring that the emotional well-being of all family members is considered.33
Furthermore, medical staff can contribute significantly to prevention and education efforts. Re-educating patients and caregivers on effective prevention and treatment strategies is essential to avoid future infestations. This includes distributing educational materials that provide clear and accurate information about head lice management. Implementing community health initiatives can help reduce the stigma associated with head lice and promote a widespread understanding of effective treatment methods.34 Ensuring access to affordable and effective treatment options, particularly in low- income or communal settings, is critical. Additionally, establishing long-term
monitoring programs in schools and communal living environments can help track and manage infestations, ultimately reducing their prevalence and impact. By connecting individuals with social services, healthcare providers can also address underlying issues that may contribute to recurrent infestations, providing a comprehensive approach to managing head lice.
Unique Populations and Special Considerations
Children are susceptible to getting head lice but are not the only populations. People who suffer from lice infestation and reside in correctional facilities, community housing (e.g., shelters, hostels), care homes, and mental health facilities are also candidates for infestation.34-37 Other individuals, like those who take selfies and live in college dormitories, may also get head lice.38,39 Each of these populations will have different needs around head lice awareness, prevention and elimination.
One of the most challenging populations is patients with mental health diagnoses. Delusional parasitosis is when individuals come to a healthcare provider convinced they have an arthropod or parasite. Although this is a more common occurrence in individuals who have traveled outside the United States, in settings where mental illness diagnoses are more frequent, medical professionals might see this as a more common occurrence. Patients must be evaluated fully through microscopic evaluation for head louse, not just egg presence, before treating any patients, especially those with mental health diagnoses.37
Ways Medical Teams Can Work Together to Improve Outcomes for Head Lice Infestation Patients
Collaborative Education Programs
Overuse of head lice medications has led to widespread treatment resistance.23 It is essential that those involved in communicating with those recommending or prescribing head lice medication are using evidence-based methods of diagnosing patients. Providing educational programs to medical
professionals encountering individuals seeking head lice medication is a good first step to help slow down treatment resistance head lice spread.40,41
Integrated Treatment Protocols
A desirable goal is to develop and implement standardized treatment protocols across different settings to ensure consistent and effective management of head lice. 20,23 This may not always be feasible; however, due to an individualized approach needed to address infection across broad ages, cultures, and extremely distinct environments, such as shelters, prisons, immigration centers, or schools. Hair stylists and dentists may also see cases of head lice.42
The American Academy of Pediatrics (AAP) recommends that after diagnosis, the first-line treatment of 1% permethrin should be used because this agent encompasses the widest group of individuals potentially affected.4 Recommendations include establishing follow-up care protocols specific to the care setting to ensure that infestations are fully resolved and to prevent re- infestation. After treatment, close follow-up of individuals in the next three weeks is prudent to detect any live lice that survived hatching from nits not killed by the treatment. The AAP and the National Association of School Nurses have published that children should not be restricted from school attendance because of head lice, given the low contagion within classrooms.4 Forming multidisciplinary teams that include healthcare providers, social workers, educators, and other facility workers may facilitate addressing head lice infestations holistically.
Environmental Management
Machine wash and dry clothing, bed linens, and other items used during the two days before the patient was treated. Use the hot water and high heat drying cycle. Clothing and items that are not washable can be dry-cleaned or sealed in a plastic bag for two weeks. Headphones can be bagged for two weeks. Alternatively, small items, like hair accessories, may also be placed in the freezer overnight.24
Soak combs and brushes in hot water for five to 10 minutes. Although the risk is very low, it is a good idea to vacuum the floor and furniture, particularly where the patient with lice sat.41
Providing personal hygiene supplies, such as combs and shampoos, to individuals in shelters and care homes may be helpful. These items should not be shared.41 Regular inspections of living environments may identify and address potential sources of head lice infestations. Teach individuals not to share clothing such as scarves, coats, or sports uniforms, or towels.43 To prevent new outbreaks, encourage individuals to feel comfortable about speaking up if they feel itchy.44
Summary
Medical providers, educators, families, and facility workers where crowded conditions exist should be aware of head lice infestations and treatments. Pyrethroids are generally recommended as first-line therapy for active infestations if pediculicide therapy is required. Head lice treatment should be effective, safe, affordable, and appropriate for the patient. The healthcare team has an active role in reassuring patients and engaging in shared decision-making to manage and eradicate the infestation optimally.
Course Test
are generally preferred as a head lice treatment if pediculicide therapy is required and resistance is not a concern.
Pyrethroids
Benzyl benzoate
Home remedies
Physical combing
Can head lice jump or fly?
Yes, they can jump, signifying close contact is not required
Yes, they can fly, signifying direct close contact is required
No, they only crawl, signifying direct close contact is required
Yes, they can do both because close contact is not required
Do head lice burrow into the skin?
Yes, they burrow deeply
Only occasionally
No, they remain on hair and scalp
Only in severe cases
What role does community engagement play in managing head lice?
It is unnecessary
It reduces stigma and improves prevention
It is only useful in rural areas
It complicates treatment
Which option below is NOT a myth about head lice?
They are caused by poor hygiene
They can jump or fly
Pets can spread them
Treatment cost is a concern
Is it important to differentiate head lice from other scalp conditions?
No, because treatments are the same for all lice types.
Yes, to ensure proper treatment.
Yes, but only for children.
No, this unnecessarily increases costs.
What is an effective way to remove head lice?
Over-the-counter dandruff shampoos if over age 1 year
Ivermectin 80 mg tablets if under age 6 years
Permethrin if over the age of 2 months
Shaving the head if over age 60 years
Which treatment can be left on the hair for about 10 minutes?
Spinosad and pyrethrins
Malathion and pyrethrins
Ivermectin and malathion
Spinosad and malathion
What are the important steps after treating head lice with malathion?
Washing bedding and clothing and freezing the malathion treatment
Checking close contacts of the patient for lice and washing toothbrushes
Wash off the treatment after 8-12 hours and wash bedding and clothes
Checking close contacts for lice and using a hair dryer with malathion
A 30-year-old woman presents with an itchy scalp and pink eye. Upon questioning, she revealed that she had shared a brush with her daughter, who also has an itchy scalp. A physical examination reveals white lice at the base of the hair shaft. Which of the following is a sodium channel blocker treatment?
Pyrethrins
Malathion
Ivermectin
Spinosad
References
Fu YT, Yao C, Deng YP, et al. Human pediculosis, a global public health problem. Infect Dis Poverty. 2022;11(1):58. Published 2022 May 26. doi:10.1186/s40249-022-00986-w
Dutra JM, Alves AD, Pessanha T, et al. Prehistorical Pediculus humanus capitis infestation: quantitative data and low vacuum scanning microscopy. Rev Inst Med Trop Sao Paulo. 2014;56(2):115-119. doi:10.1590/S0036-46652014000200005
Leonard V. How to Manage Pests Pests of Homes, Structures, People, and Pets: Head Lice. UC Statewide Integrated Pest Management Program. https://ipm.ucanr.edu/PMG/PESTNOTES/pn7446.html. Accessed September 23, 2024.
Nolt D, Moore S, Yan AC, Melnick L; COMMITTEE ON INFECTIOUS DISEASES, COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE,
SECTION ON DERMATOLOGY. Head Lice. Pediatrics. 2022;150(4):e2022059282. doi:10.1542/peds.2022-059282
Kartashova OV, Lobuteva LA, Zakharova OV, Lobuteva AV, Goykhman
AA. Medical and Social Factors of Pediculosis. Maced J Med Sci.
2019;7(19):3240-3244. doi: 10.3889/oamjms.2019.699
Flinders DC, De Schweinitz P. Pediculosis and scabies. Am Fam Physician. 2004;69(2):341-348.
Strahan AG, Elston DM. Dermatologic Care for Refugees: Effective Management of Scabies and Pediculosis. Cutis. 2024;113(4):E16-E21. doi: 10.12788/cutis.0999.
Hansen RC, O'Haver J. Economic considerations associated with Pediculus humanus capitis infestation. Clin Pediatr. 2004;43(6):523-7. doi: 10.1177/000992280404300603
Meister L, Ochsendorf F. Head Lice. Dtsch Arztebl Int.
2016;113(45):763-772. doi:10.3238/arztebl.2016.0763
Salavastru CM, Chosidow O, Janier M, Tiplica GS. European guideline for the management of pediculosis pubis. J Eur Acad Dermatol Venereol. 2017;31(9):1425-1428. doi: 10.1111/jdv.14420
Lowenstein EJ, Parish LC, Van Leer-Greenberg M, Hoenig LJ. The darker side of head lice infestations. Clin Dermatol. 2022;40(1):81-84. doi: 10.1016/j.clindermatol.2021.01.010
Department of Defense United States of America. Armed Forces Pest Management Board Technical Guide No. 6 Delousing Procedures for Contingency Operations Delousing Procedures for the Control of Louse- Borne Disease during Contingency Operations. Department of Defense United States of America; 2024. https://www.acq.osd.mil/eie/afpmb/docs/techguides/tg6.pdf. Accessed August 6, 2024.
American Academy of Dermatology Associates. Head lice: Signs and symptoms. AAD. 2024. https://www.aad.org/public/diseases/a-z/head- lice-symptoms. Accessed September 23, 2024.
Leung AKC, Lam JM, Leong KF, Barankin B, Hon KL. Paediatrics: how to manage pediculosis capitis. Drugs Context. 2022;11:2021-11-3. Published 2022 Mar 14. doi:10.7573/dic.2021-11-3
Galassi FG, Picollo MI, González-Audino P. Cuticular extracts induce aggregation in head lice. Med Vet Entomol. 2024;38(2):227-233. doi:10.1111/mve.12711
Taravati S. Distinguishing Between Crab, Body, and Head Lice. ANR Blogs. Published December 20, 2020. Accessed August 26, 2024. https://ucanr.edu/blogs/blogcore/postdetail.cfm?postnum=44339&. Accessed August 26, 2024.
Khais Muri Laabusi A, Mohsan Rhadi M. Prevalence of Pediculus humunus capitis, Pediculus humanus corporis, and Pthirus pubis in Al- Kut, Iraq. Arch Razi Inst. 2022;77(1):497-501. Published 2022 Feb 28. doi:10.22092/ARI.2022.357091.1969
Nie J, Shen X, Li Y, Wang W. Case Series of Phthirus pubis Infestation in Non-Perineal Regions. Clin Cosmet Investig Dermatol. 2023;16:2277- 2281. Published 2023 Aug 22. doi:10.2147/CCID.S422318
Álvarez-Fernández BE, Valero MA, Nogueda-Torres B, Morales-Suárez- Varela MM. Embryonic Development of Pediculus humanus capitis: Morphological Update and Proposal of New External Markers for the Differentiation Between Early, Medium, and Late Eggs. Acta Parasitol. 2023;68(2):334-343. doi:10.1007/s11686-023-00667-0
Gunning K, Kiraly B, Pippitt K. Lice and Scabies: Treatment Update. Am Fam Physician. 2019;99(10):635-642.
Centers for Disease Control and Prevention. Clinical Care of Head Lice. CDC. April 8, 2024. https://www.cdc.gov/lice/hcp/clinical- care/index.html#:~:text=Many%20head%20lice%20medications%20ar e,allergic%20to%20chrysanthemums%20or%20ragweed. Accessed August 26, 2024.
United States Environmental Protection Agency. About Lice and Their Control. EPA. June 13, 2024. https://www.epa.gov/ipm/about-lice-and-
their-control. Accessed August 26, 2024.
Stevenson B, Tesfaye W, Christenson J, et al. Comparative efficacy and safety of interventions for treating head lice: a protocol for systematic review and network meta-analysis. BMJ Paediatr Open. 2021;5(1):e001129. Published 2021 May 10. doi:10.1136/bmjpo-2021-
001129
American Academy of Dermatology. Head lice: Diagnosis and treatment. AAD. 2024. https://www.aad.org/public/diseases/a-z/head- lice-treatment. Accessed August 24, 2024.
Mazurek CM, Lee NP. How to manage head lice. West J Med.
2000;172(5):342-345.
Srtomectol. Prescribing information. Merck&Co., Inc. 2022. https://www.merck.com/product/usa/pi_circulars/s/stromectol/stromec tol_pi.pdf. Accessed September 2, 2024.
Sklice. Azurity Pharmaceuticals. 2024. https://www.sklice.com/pages/how-to-use. Accessed September 2, 2024.
Spinosad Topical Suspension. Prescribing Information. Allegis Pharmaceuticals, LLC. April 2021. https://www.spinosadrx.com/wp- content/uploads/2021/07/spn-pi-002-spinosad-ts-pi-full-prescibing- and-patient-information-04282021.pdf. Accessed September 2, 2024.
Panagopoulou P, Ioannidou G, Beropouli S, Fotoulaki M. Head lice presenting with isolated severe eosinophilia in a child. Hippokratia. 2023;27(3):112-114.
Ovide Prescribing information. Drugs.com. August 5, 2024.
https://www.drugs.com/pro/ovide.html. Accessed August 30, 2024.
Malathion (topical route). Mayo Clinic. February 1, 2024. https://www.mayoclinic.org/drugs-supplements/malathion-topical- route/proper-use/drg-20067289. Accessed August 30, 2024.
Babazadeh T, Chollou KM, Abedi-Nerbin S, Abedi-Nerbin S, Shahnavaz- Yoshanluie F, Ranjbaran S. Head lice infestation and the role of some cognitive-behavioral factors in its spread and prevention among adolescent girls: A cross-sectional study in Northwest Iran. Health Sci Rep. 2023;6(11):e1679. Published 2023 Nov 1. doi:10.1002/hsr2.1679
Bever L. In head lice outbreaks, “selfies” may be a surprising culprit. WELL+BEING. Published June 28, 2024. https://www.washingtonpost.com/wellness/2024/06/28/head-lice- infestations/. Accessed September 23, 2024.
Mumcuoglu KY, Pollack RJ, Reed DL, et al. International recommendations for an effective control of head louse infestations. Int J Dermatol. 2021;60(3):272-280. doi:10.1111/ijd.15096
Federal Bureau of Prisons. Lice Protocol: Federal Bureau of Prisons Clinical Practice Guidelines. Federal Bureau of Prisons. Published October 2014. https://www.bop.gov/resources/pdfs/lice.pdf. Accessed September 23, 2024.
Campos Nogueira R, Nonato FR, Duchene Veauvy MC, Cavin AL, Al- Anbaki M, Graz B. Head Lice at School: Traditional Medicine and Community Engagement. Health Equity. 2021;5(1):310-315. Published 2021 May 13. doi:10.1089/heq.2020.0065
McLellan S. Perspectives: Delusional Parasitosis. CDC Yellow Book 2024. Published May 1, 2023. https://wwwnc.cdc.gov/travel/yellowbook/2024/posttravel- evaluation/delusional-parasitosis. Accessed August 26, 2024.
Bever L. In head lice outbreaks, “selfies” may be a surprising culprit. WELL+BEING. Published June 28, 2024. https://www.washingtonpost.com/wellness/2024/06/28/head-lice- infestations/. Accessed August 26, 2024.
Bell M. The Adventures of “Lice Girl” - College Magazine. College Magazine. Published November 14, 2016. Accessed August 26, 2024. https://www.collegemagazine.com/adventures-lice-girl/. Accessed August 26, 2024.
Toghroli R, Hosseini Z, Ziapour A, Yari A, Rahimi SF, Mehedi N. Explaining the Determinants of Pediculosis Control and Prevention: A Qualitative Study in Southern Iran. Inquiry. 2022;59:469580221086369. doi:10.1177/00469580221086369
US Department of Health and Human Services. Head Lice. Head Start | ECLKC. Published March 24, 2024. https://eclkc.ohs.acf.hhs.gov/physical-health/article/head-lice. Accessed August 26, 2024.
Leary K, Hechler E, Qian F, Weber-Gasparoni K. Management of Head Lice in Dental Offices: A Call for Updated Policies. J Dent Child. 2021;88(2):108-113.
Centers for Disease Control and Prevention. About Head Lice. CDC. June 4, 2024. .https://www.cdc.gov/lice/about/head-lice.html. Accessed
August 25, 2024.
The National Pediculosis Association. Child Care Provider’s Guide to Controlling Head Lice. NPA. 2001. http://www.headlice.org/downloads/ccguide.pdf. Accessed August 25, 2024.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information
prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.