FERTILITY MEDICATIONS: A PRIMER FOR PHARMACISTS
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University College of Pharmacy. She serves as Director of Instructional Labs and is course director for the Basic Pharmaceutics Lab and Parenteral Products and Parenteral Products Lab courses.
Topic Overview
Within the United States (US), an estimated 1 in 5 women will experience infertility. Infertility is a disease with health implications and important economic and social ramifications. Management of infertility is highly patient- specific and factors including the underlying cause, patient age, comorbidities, and cost determine the treatment plan. A diagnosis of infertility can be devastating, and attempting to understand related procedures and medications can be overwhelming for patients. It is important for patients to be educated on the causes and risk factors associated with infertility, counseled on nonpharmacologic and pharmacologic medications, and offered resources to decrease the financial burden associated with infertility treatments. This course will provide an overview of the causes and process of diagnosing infertility and discuss available infertility treatment options. Mechanisms of action, side effects profiles, benefits, and success rates will be discussed for various fertility medications.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-064-H01-P
Pharmacy Technician 0669-0000-23-065-H01-T
Credits: 1 hour of continuing education credit
Type of Activity: Knowledge
Media: Internet Fee Information: $4.99
Estimated time to complete activity: 1 hour, including Course Test and course evaluation
Release Date: May 1, 2023 Expiration Date: May 1, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From May 1, 2023, through May 1, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Recall the causes of infertility
Describe available treatment options for infertility
Discuss indications, contraindications, side effect profiles, and monitoring parameters for fertility medications
Describe the role of the pharmacist in managing infertility
Disclosures
The following individuals were involved in developing this activity: Liz Fredrickson, PharmD, BCPS, Pamela M. Sardo, PharmD, BS, and Susan DePasquale, MSN, PMHNP-BC. Pamela Sardo, PharmD, BS, was an employee of Rhythm Pharmaceuticals until March 2022, and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in developing this activity.
© RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Approximately 20% of women in the United States will experience infertility. A diagnosis of infertility can be devastating, and attempting to understand related procedures and medications can feel overwhelming for patients. It is important that patients are educated on the causes and risk factors associated with infertility, counseled on nonpharmacologic and pharmacologic medications and offered resources to decrease the financial burden associated with infertility treatments. This course will provide an overview of the causes and process of diagnosing infertility and discuss available treatment options. Mechanisms of action, side effects profiles, benefits, and failure rates will be discussed for various fertility medications.
Definition and Prevalence of Infertility
Within the United States, an estimated 1 in 5 women are infertile.1 Defined as failure to achieve a pregnancy after 12 months of regular, unprotected sexual intercourse, infertility is a disease with not only health implications, but important economic and social ramifications as well.2 Management of infertility is highly patient-specific and factors including the underlying cause, patient age, comorbidities, and cost will determine the treatment plan.2 The terms defined in Table 1 may be used when discussing infertility (Table 1).
Table 1
| Term | Definition |
| Fecundity | Capacity to have a live birth |
| Fecundability | probability of achieving a pregnancy in a single menstrual cycle with adequate sperm exposure and no contraception that results in a live birth |
| Fertility | the ability to have a clinical pregnancy |
| Time to pregnancy | he length of time, usually measured in months, that it takes a couple to conceive |
Etiology and Risk Factors
An estimated 13% of reproductive-age women in the US seek out infertility treatment each year.3 Current guidelines recommend couples consider infertility treatments after 12 months of regular sexual intercourse with no resulting pregnancy.4 However, this decision should be patient- specific, and older women and those with relevant medical histories or physical findings may require an earlier evaluation.4 It is recommended women 35 years or older seek evaluation by the six-month mark and women older than 40 can do so immediately.4 Patients with known oligomenorrhea (fewer than 6-8 menstrual periods per year), amenorrhea (one or more missing menstrual periods), or uterine or tubal disease should also be evaluated prior to the 12- month mark.3
For most couples, infertility is the result of either an abnormality in physiology or an underlying disease. However, 15% of infertile couples will be given a diagnosis of “unexplained infertility”, with no discernible cause identified.3 Infertility can be subdivided into primary infertility (no previous pregnancies achieved) and secondary infertility (a minimum of one prior pregnancy has been achieved).5 Causes of infertility may be categorized as female, male, or unexplained.2 Table 2 details these common etiologies.2,6
Table 2. Common Causes of Infertility2
| Cause | Percent of Cases | Types |
| Female | 30-40% | Ovulatory Dysfunction Tubal Endocrine Uterine Other |
| Male | 40-50% | Endocrine Anatomic Testicular defects/genetic issues Unknown |
Ovulation disorders account for many cases of infertility and are categorized into three groups by The World Health Organization (Table 3).7 Women with Group 1 disorders will present with amenorrhea and have low levels of gonadotropins and estrogen.7 Causes of Group 1 disorders include eating disorders and excessive exercise.7 Group 2 disorders result from dysfunction within the hypothalamic-pituitary-ovarian axis with related conditions, including polycystic ovarian syndrome (PCOS) and hyperprolactinemic amenorrhea.6 PCOS is the most common cause of anovulatory infertility.2 Group 3 disorders are due to ovarian failure, in which hyper-gonadotropic, hypoestrogenic anovulation is seen.6 Ovarian reserve decreases naturally as women age, especially after age 35. However, many other factors can hasten this process, including prior chemotherapy or radiation, ovarian surgery, and a family history of premature menopause.2
Table 3. World Health Organization Ovulation Disorders6
| Group | Cause | Disorders | Percent of Ovulation Disorders |
| Group 1 (Hypogonadotropic hypogonal anovulation) | Hypothalamic pituitary failure | Hypothalamic amenorrhea Hypogonadotropic hypogonadism | 10% |
Group 2 (Normo- gonadotropic, normo-estrogenic anovulation) | Hypothalamic- pituitary- ovarian axis dysfunction | Polycystic ovarian syndrome (PCOS) and hyperprolactinemic amenorrhea | 85% |
| Group 3 (Hyper- gonadotropic, hypoestrogenic anovulation) | Ovarian failure | — | 5% |
Tubal infertility occurs when the fallopian tubes are blocked or cannot pick up an oocyte due to issues such as pelvic adhesions.3 These cases account for 11 to 67% of infertility diagnoses.3 Tubal infertility can result from pelvic inflammatory disease, salpingitis isthmica nodosa, endometriosis, and prior surgery.2
Infertility can occur in women of all ages, but age does play a role. This may be due to many factors, including an increased risk of disorders that can affect fertility.4 Women younger than 30 have an 85% chance of conceiving within one year.8 By the age of thirty, this decreases to approximately 75%.8 At age 35, the chance is 66% and at age 40 it is 44%.8 Age is also a major consideration in determining the success of infertility treatments. As patients age, the success rates for treatments generally decrease.3
Evaluation and Diagnosis
Evaluating a patient for infertility and determining a diagnosis involves an understanding of both the female reproductive system and menstrual cycle. These are described in detail below.
Female Reproductive System
The female reproductive system (Figure 1) consists of the vagina, ovaries, uterus, cervix, and fallopian tubes.9 The uterus is a pelvic organ that serves many functions, including as a site of implantation for a blastocyst and later providing support for a developing fetus.10 It also has a membrane lining called the endometrium, which is shed during the menstrual period.10 The ovaries are the main organs of the female reproductive system and contain thousands of follicles.10 A woman is born with all the oocytes she will have during her lifetime (between 1 and 2 million); by the age of menopause, this number is approximately 1000.4 The ovaries connect to the uterus via the fallopian tubes, which carry a fertilized egg cell (zygote) to the uterus for implantation.10 The vagina serves as an entryway for the sperm, and the cervix is a passageway into and out of the uterus that allows for sperm entry.10
Figure 1. The Female Reproductive System9
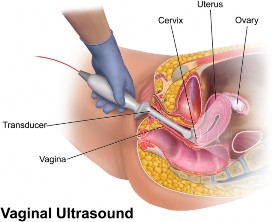
For the female reproductive system to function in a normal manner, hormonal signals from the hypothalamus, pituitary gland and ovaries must integrate to promote follicle development and ovulation.11
Menstrual Cycle
An understanding of the menstrual cycle can assist pharmacists in understanding the causes of infertility. The menstrual cycle begins with menarche (the occurrence of a first menstrual cycle) which occurs between the ages of 10 to 16, and continues until menopause is reached, typically around age 50.11 During a cycle, various hormones interact to stimulate ovulation. The menstrual cycle is divided into three phases, including the follicular phase, the ovulatory phase, and the luteal phase.11 The length of a menstrual cycle is the number of days from the first day of bleeding to the onset of menstruation in the next cycle.12 The average length of a menstrual cycle is 28 days, but this can vary widely (a common range is 21 to 40 days) and be impacted by numerous factors, including body weight, nutritional status, and medical conditions.11 Figure 2 visually depicts the menstrual cycle, and the three phases are described in more detail below.13
Figure 2. The Menstrual Cycle13
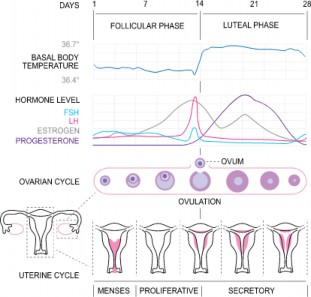
The Follicular (Proliferative) Phase
The first day of menses (bleeding) is considered Day 1 of the menstrual cycle and commences the follicular, or proliferative, phase.11,12 In a standard, 28-day cycle, the follicular phase will continue until day 14.11,12 The range of normal menstrual cycle lengths is due to variations in the length of the follicular phase.12,13 At the onset of the follicular phase, levels of FSH increase, which aids in recruiting follicles to grow and develop.11 A follicle is a small, fluid-filled sac that contains an immature egg.14 One of these follicles will become the dominant follicle and release the oocyte (egg cell) via rupturing.11,12 This dominant follicle is able to keep the remaining follicles from development by increasing levels of two hormones: estradiol and inhibin.11 These hormones act on the hypothalamus to prevent the release of gonadotropin-releasing hormone (GnRH) and on the pituitary gland to prevent the release of FSH in a negative feedback manner.11 The more estradiol a woman’s body produces, the less GnRH and FSH will be released. As the dominant follicle grows, it produces three other hormones: estradiol, progesterone, and androgen.11 Estradiol acts to stop menses from the
previous cycle, which thickens the uterine lining.11 At the end of the follicular phase, the dominant follicle is ready for ovulation.
Ovulatory Phase
Ovulation occurs 14 days before menses, so would occur around day 14 during an average 28-day cycle.11 The ovulatory phase is the time during which the oocyte ruptures from the follicle.11 When critical levels of estradiol are reached, the pituitary gland releases high levels of a hormone called luteinizing hormone (LH).11,12 This is known as the “LH surge”.11,12 The rapid rise in LH causes the final maturation of the follicle and release of the oocyte.12 Ovulation will generally occur sometime between 24 and 36 hours after estradiol peaks and 10 to 12 hours after LH peaks.11,12 Once ovulation has occurred, the oocyte is able to travel via the fallopian tube for fertilization and then to the uterus for implantation of the embryo if fertilization was successful.11,12
Luteal Phase
The final phase of the menstrual cycle is the luteal or secretory phase, which follows ovulation and lasts until the next menstrual cycle begins.11,12 A typical luteal phase is 14 days in length.12 The dominant hormone in this phase is progesterone, which acts in a negative feedback manner to decrease LH and FSH levels.12 During the luteal phase, the dominant follicle becomes the corpus luteum.12 Progesterone produced by the corpus luteum is key in maintaining the endometrial lining to support the implanted embryo and maintain a pregnancy.11 If pregnancy does occur, a hormone called human chorionic gonadotropin (HCG) will sustain the corpus luteum and stimulate continued production of estrogen and progesterone until the placenta takes over.11,12 Progesterone levels decrease if pregnancy does not occur as a result of failed fertilization or implantation.11,12 This rapid drop in progesterone causes the endometrial lining to shed, and a new menstrual cycle then begins.11,12
Fertility Evaluation
Fertility evaluations should involve both partners, given the broad range of causes and high prevalence of unexplained infertility.2 Initial evaluations include a medical history, laboratory testing, and physical exam.2 Medical histories can uncover potential risk factors for infertility, such as alcohol and tobacco use and intense exercise.2 Clinicians should also determine how well a couple understands ovulation; and, if they are using the correct methods to detect ovulation, and if they are timing intercourse appropriately.2 The female partner should undergo a physical assessment, including body weight, blood pressure, and thyroid, breast, and pelvic examinations.2 Ultrasound can detect uterine abnormalities and evaluate ovarian reserve via counting the number of antral follicles.2 Fallopian tube patency can be determined via a hysterosalpingogram (HSG), which is completed by injecting a radiopaque contrast into the uterus and imaging the flow through the fallopian tubes.2 Obtaining an FSH level and estradiol level on day 2 or 3 of the menstrual cycle can assist with assessing ovarian reserve.2 Serum anti-mullerian hormone (AMH) levels can be used in combination with ultrasound findings and the patient’s age to identify diminished ovarian reserve.2 Other lab work to consider in women with irregular menstrual cycles includes TSH, prolactin, and androgens.2
Treatment of Infertility Nonpharmacologic Management
Managing infertility from a nonpharmacologic perspective involves reducing risk factors that may contribute to infertility. Prior to initiating infertility treatment, it is important to manage identified underlying causes, including excess body weight, lack of exercise, poor diet, and medication use.6 A 2017 review sought to assess the effect of physical activity on ovulation.15 Cohort studies within this review found the risk of anovulation increased in those who engaged in extremely heavy exercise (> 60 minutes per day) but exercising between 30 and 60 minutes per day reduced the risk of anovulatory
infertility.15 In patients with PCOS, exercising, even without changes in diet, can assist with the resumption of ovulation.15
Patients should also focus on consuming a healthy diet—one low in saturated fat, high in fiber, and low in animal protein.6 Other recommendations include avoiding alcohol, tobacco, and recreational drug use.6 A review of the effects of diet on infertility suggests the use of antioxidant supplements is not likely to make a difference in terms of improving fertility, but this is limited by a lack of data to make this determination.16 Use of folic acid in conjunction with assisted reproductive technology may lead to increased rates of fertility and live births.16 Higher doses of folic acid with additional vitamin B12 may also be of value.16 Literature assessing vitamin D use has focused only on women with levels close to normal, so while adequate supplementation does not appear to play a role in fertility, the effects of severe deficiency cannot be ruled out.16 While few studies have investigated the effects of dairy foods, these likely do not have an important effect on fertility.16 In general, consuming a “healthy” diet will likely assist in improving fertility and live birth rates in those undergoing ART.
Assisted Reproductive Technology
Within the United States, the use of assisted reproductive technology (ART) has risen significantly over the past few decades, with 182,111 procedures completed in 2015.17 Assisted reproductive technology encompasses several procedures that involve handling embryos or oocytes and sperm in vitro.17 Each protocol may vary and is specific to the fertility clinic, including intrauterine insemination (IUI) and in vitro fertilization (IVF).6 For IUI, sperm is prepared and placed into the uterus directly.6 Intrauterine insemination procedures are often done in conjunction with a medication regimen that stimulates ovulation prior to the procedure.6 Intrauterine insemination can assist not only in cases of unexplained infertility, but also for couples with male factor infertility, those who cannot engage in vaginal intercourse, or those in same-sex relationships.6 In-vitro fertilization is a procedure in which oocytes are fertilized in a laboratory and then transferred directly to the uterus, bypassing the fallopian tubes.2 IVF provides couples
with tubal infertility the best chance of success.2 These procedures are more involved (and typically more expensive) than IUI.
The following steps are included within a typical ART cycle:18
Medications are started to stimulate the growth of multiple ovarian follicles while other drugs are given to suppress the natural menstrual cycle and down-regulate the pituitary gland
Ovarian stimulating drugs are started
Follicle growth is monitored
Ovulation-triggering medication is given to cause egg maturation once follicles have reached an appropriate size
Eggs are collected and sperm is retrieved (if needed)
Fertilization via IVF or ICSI is completed
Laboratory procedures are done for embryo culture
Embryos are placed in the uterus
The luteal phase is supported via progesterone, estrogen, and/or hCG
Pharmacologic Therapies
Pharmacologic infertility treatments involve ovulation induction.
Table 4. Medications Used to Treat Infertility6
| Medication(s) | Indications | Dosing | Storage conditions | Adverse reactions, contraindications |
| Clomiphene citrate (Clomid) | Treatment of ovulatory disorders | 50-150 mg once daily by mouth for 5 days (starting on days 3, 4, or 5 of the cycle) | Store at room temperature Avoid excessive exposure to heat, light, humidity | Ovary enlargement, hot flashes, headache, abdominal distension, vomiting, breast discomfort.
Potential visual changes and OHSS |
| Contraindicated in thyroid and adrenal dysfunction |
| Letrozole (Femara) | Ovulation stimulation in anovulatory women with PCOS | 2.5-7.5 mg once daily by mouth for 5 days starting on day 3, 4, or 5 of the cycle | Store at room temperature | Flushing, edema, headache, dizziness, fatigue, night sweats, weight gain, nausea |
| Follitropin alpha (Gonal-f; Follitropin beta (Follistim AQ) | Ovulation induction and multifollicular development during ART | Dose is individu- alized based on thera- peutic response. Doses can vary from 37.5 to 450 IU daily | Follitropin alpha: refrigerate or store vials at room temperature; after reconstitution store them at room temperature or in a refrigerator for up to 28 days | Headache, ovarian cysts, abdominal pain, nausea, injection site reaction, potential OHSS |
| Follitropin beta should be refrigerated before dispensing and stored in a refrigerator or at room temperature for up to 28 days | ||||
| Menotropin | Ovulation | Doses vary. | Refrigerate or | Headache, OHSS, |
| (Menopur) | induction and | store at room | abdominal pain, | |
| mutifollicular | temperature | vomiting, diarrhea | ||
| development | ||||
| during ART | ||||
| Leuprolide (Lupron- Depot) | Ovulation trigger (off- label use) | Dosing protocols vary. | Refrigerate | Pain at injection site; mood changes, headache, skin rash |
| Cetrorelix | Adjunct to | Varying | Refrigerate and | Headache, OHSS, |
| (Cetrotide) and | controlled | dosing | protect from | nausea, pelvic pain, |
| Ganirelix (Fyremadel) | ovarian stimulation | protocols. | light | injection site reaction |
Physiologically, only one follicle typically becomes dominant during the menstrual cycle, but ovulation induction seeks to develop and mature many follicles.2 Use of these medications is commonly paired with either IUI or IVF.2 Patients may also have the option of having timed intercourse.2 Oral and parenteral medications are available and summarized in Table 4 above.
Clomiphene
Clomiphene citrate (CC), brand name Clomid, is a selective, nonsteroidal estrogen receptor modulator (SERM).19 It has FDA approval for the treatment of ovulatory dysfunction in women with infertility.6 SERMs are a class of medications with tissue-specificity and can function as estrogen receptor agonists or antagonists depending on the tissue.6,19 Clomiphene citrate exerts its effects at the hypothalamus, where it binds estrogen receptors (ER) longer than estrogen does.19 By doing so, clomiphene interferes with receptor recycling and inhibits normal estrogenic negative feedback, increasing GnRH secretion and release of FSH and LH.19 This leads to ovarian follicle development and ovulation.
Ovulation is expected 5 to 10 days following a course of CC, and because of this, it is generally taken around the fifth day of a menstrual cycle.19 The starting dose of clomiphene is 50 mg once daily for five days.19 The dose can be increased to 100 mg once daily if ovulation does not occur at the 50 mg dose.19 While doses up to 250 mg once daily have been used, doses greater than 100 mg daily have not been shown to increase pregnancy rates, and this is the recommended maximum dose.19 It is recommended to discontinue the use of CC if ovulation does not occur after three courses of treatment or if ovulation occurs three times, but no pregnancy is achieved.19 No dose adjustments are needed for impaired renal function, but use is contraindicated in patients who have a history of liver disease.19
Clomiphene is associated with many side effects, including ovary enlargement, hot flashes, gastrointestinal distress, bloating, and breast discomfort.19 A serious potential side effect is ovarian hyperstimulation syndrome (OHSS), which is categorized by severe abdominal pain, severe
nausea and vomiting, excessive weight gain, and shortness of breath. Another serious side effect is visual changes.19 These are rare, and more likely to occur with higher doses and longer durations of therapy, and in some cases, the changes will be irreversible.19 If OHSS or visual changes occur, CC should be discontinued, and the patient seen as soon as possible for evaluation.19 Contraindications include hypersensitivity to clomiphene, uncontrolled thyroid or adrenal dysfunction, pregnancy, and organic intracranial lesions.19
In clinical trials, CC pregnancies occurred in approximately 30% of patients, with an incidence of multiple pregnancies (twins, triplets, or more) of around 8 percent.6 Up to 15% of patients may be clomiphene resistant and not respond to treatment.20
Letrozole
Letrozole, brand name Femara, is a third-generation, nonsteroidal, highly selective aromatase inhibitor (AI).20,21 It was first used for inducing ovulation in animals in 1993.20 The aromatase enzyme catalyzes the conversion of androstenedione to estrone and testosterone to estradiol.20 Letrozole reversibly binds to and inhibits the aromatase enzyme in a competitive manner (more than 99%), thereby reducing plasma estrogen levels.20,21 This decrease in estrogen leads to an increase in the secretion of FSH, which stimulates ovulation.21 Letrozole may also work peripherally via blocking the conversion of androgen substrates to estrogen, thereby increasing follicle sensitivity by increasing the expression of the FSH receptor gene.20 Letrozole reaches steady-state levels between 2 and 6 weeks and is rapidly and well-absorbed (mean bioavailability is 99.9%).20,21 It undergoes hepatic metabolism via CYP3A4 and CYP2A6.21 It can be taken with or without food.21
Use of letrozole is off-label for infertility, but it is common for females with ovulatory disorders, normal or elevated estrogen concentrations, and irregular ovulation.21 It is recommended first-line for patients with PCOS, given the results of the Polycystic Ovary 2 Trial, which found letrozole resulted in higher live births than clomiphene (27.5% vs. 19.1%).22 These results were
echoed by a 2018 Cochrane review that included 42 RCTS.23 Within this review, live birth rates were higher with letrozole, and there was no difference between rates of OHSS, miscarriage, and multiple pregnancies.23 Letrozole has also demonstrated effectiveness in preparing the endometrium for thawed-embryo transfers (FET) and can be used in women who ovulate to better their chances of pregnancy.20,21 Diagnoses that may benefit include endometriosis, pelvic factors, and advanced maternal age.20
Letrozole protocols mirror those used for clomiphene.20 For use as an ovulation induction agent, letrozole is started at 2.5 mg once daily for 5 days, typically on days 3, 4, or 5 of the menstrual cycle or following a progestin- induced bleed.21 Typical follicle sizes as this time range from 6 to 8 mm, and these follicles have high levels of androgen receptors and increased androgen levels, encouraging FSH receptor induction.21 The dose may be increased to 5 mg daily for five days if ovulation does not occur with use of the 2.5 mg dose.21 The maximum recommended dose is 7.5 mg/day. It is not clear how often letrozole can be used, but one study dosed letrozole for a maximum of five cycles.20
The adverse effects of letrozole were demonstrated in its use for post- menopausal women with breast cancer who were on the treatment much longer than those using it for ovulation induction.20 However, women using letrozole for infertility may still experience headache, flushing, diaphoresis, night sweats, and hot flashes.21 OHSS may also occur.21 Three significant letrozole side effects include decreased bone mineral density, ischemic cardiovascular events, and musculoskeletal effects, but these are not as likely with the short-time use associated with ovulation induction.20,21 Letrozole is safe from a teratogenic perspective, but additional research is needed to determine the long-term effects on children.20
Letrozole use can be paired with timed intercourse or IUI. The use of letrozole is associated with pregnancy rates of 23% and an incidence of multiple pregnancies of 13%.6 Studies have not found a significant difference in many side effects when comparing letrozole and clomiphene, though letrozole may cause more fatigue and dizziness while clomiphene may cause
more hot flashes.6 Compared to clomiphene, letrozole tends to promote the development of only one follicle, as it does not inhibit negative feedback of estrogen.6 Also compared to clomiphene, letrozole has a short half-life and, therefore, may not cause the adverse effects on cervical mucus and endometrium that clomiphene does.21
Patients in WHO Group 2 anovulation who use letrozole may have higher ovulation rates, pregnancy rates, and live birth rates, but no differences in multiple pregnancies and miscarriage rates.20 Additional studies are needed to determine the role of letrozole in unexplained infertility.
Gonadotropins
Patients with a condition called hypogonadotropic hypogonadism have little or no response to pituitary gonadotropin release.2 Because of this, clomiphene and letrozole are of little use.3 Instead, exogenous gonadotropins can be used to stimulate ovarian follicles.3 Women who benefit from gonadotropins include those with PCOS who have not ovulated or conceived despite weight loss or use of clomiphene or letrozole therapy; those with hypothalamic anovulatory hypopituitarism disorders; and those with hypothalamic amenorrhea.3 A 2019 Cochrane review found gonadotropins resulted in a greater percentage of live births than clomiphene after six cycles for those with PCOS but also a higher rates of multiple pregnancies.24
Gonadotropins are injectable medications used as ovarian stimulators.6 They enhance ovulation function by providing FSH and LH activity, leading to the recruitment and growth of many follicles.6 Menotropins (brand name Menopur) are one category of gonadotropins.25 These are a purified combination of FSH and LH in a 1:1 ratio that has been extracted from the urine of postmenopausal women.25 Menopur is available as a powder for reconstitution and contains 75 units of menotropins, which represents 75 units of FSH and LH activity.25 The half-life of Menopur is 11-13 hours and it peaks within 18 hours following a single subcutaneous dose.25 Menopur is dosed as 225 units once daily beginning on cycle day 2 or 3.25 The dose can be adjusted after 5 days based on ultrasound monitoring of ovarian response and/or
measurement of serum estradiol levels.25 It is recommended to not make additional adjustments more frequently than once every 2 days or by >150 units.25 The maximum daily dose is 450 units.25
Follitropin alpha (Gonal-f) is another type of gonadotropin used for ovarian stimulation.26 For use in ovulation induction, it is dosed subcutaneously as 75 units for 14 days in an initial cycle, with doses increased by 37.5 units after 14 days, based on ovarian response.26 The dose can continue to be adjusted to a maximum of 300 units daily.26 Gonal-f is continued until serum estradiol levels and/or follicle growth indicate an appropriate ovarian response.26 It is generally recommended therapy does not exceed 35 days.26 For use in multi-follicular development during ART, Gonal- f is dosed around day 2 or 3 of the cycle at 150 units daily until appropriate follicular development is attained.26
Follitropin beta, brand name Follistim AQ, can be used for ovulation induction in anovulatory patients.27 It is available as a cartridge that contains a prefilled solution and is administered via a pen injector device.27 Dosing for Follistim AQ cartridge is done via a stepwise approach, with an initial dose of 50 units per day for the first 7 days.27 The dose is then increased by 25 or 50 units weekly until follicular growth or estradiol levels demonstrate an adequate ovarian response.27 The dose can be adjusted to prevent the development of too many follicles, which would result in cancellation of the cycle.26 The maximum recommended dose is 250 units.27
Another gonadotropin used is recombinant chorionic gonadotropin.28 This medication, brand name Ovidrel, causes ovulation to occur following use of other fertility medications.28 Ovidrel is injected subcutaneously at a dose of 250 mcg 1 day after the final dose of a follicle stimulating agent.28
Gonadotropin therapy is monitored with transvaginal ultrasound and measuring levels of FSH, LH, and estradiol.25-27 Depending on the protocol, an ovulation trigger is given once the target number of follicles are developed.6 Cycles may be canceled if follicles do not reach target size (>15 mm) or an inadequate number develop.6 Use of gonadotropins is associated with injection
site reactions.25-27 These medications also put patients at a much higher risk of multiple gestation compared to clomiphene and letrozole.25-27 Other side effects include headache, abdominal pain, nausea, and OHSS.25-27
GnRH Agonists and Antagonists
Some women will undergo controlled ovarian hyperstimulation (COH) to develop many follicles that can be retrieved and fertilized.6 These agents are used along with medications that cause ovulation induction.6 Leuprolide (Lupron-Depot) is a GnRH agonist.29 By inhibiting gonadotropin secretion, leuprolide increases levels of LH and FSH.29 Leuprolide has a half-life of about 3 hours and has a bioavailability of 94%.29 It is administered subcutaneously, and typical starting doses are 0.5 to 1 mg daily.29 Common side effects include pain at the injection site, emotional lability, headache, mood changes, weight gain, and skin rash.29
Cetrorelix (Cetrotide) and ganirelix (Fyremadel) are GnRH antagonists. These agents compete with GnRH to bind to pituitary receptors, which delays the LH surge and prevents ovulation until follicles are the appropriate size.30,31 Cetrorelix and ganirelix are used as adjuncts for controlled ovarian stimulation.6,30,31 They are given subcutaneously, and dosing protocols vary based on the patient.30,31 Possible side effects include headache, OHSS, nausea, and injection site reactions.30,31
Determining a Management Strategy
Once a patient has been evaluated, a treatment recommendation will be made based on results and findings. Success rates vary and will depend on many factors, including the female partner’s age, ovarian reserve, history of smoking, BMI, and race.2 Table 5 summarizes recommendations based on the underlying cause of infertility.2
Table 5. Management Recommendations
| Condition | Recommendation |
| Ovulatory dysfunction that is the result of endocrine disorders (hypothyroidism) | Treat conditions prior to undergo fertility treatments |
| Anovulatory infertility | Clomiphene citrate and letrozole to induce ovulation. Second-line medications, such as metformin, may also be needed, especially in women with obesity |
| Hypothalamic amenorrhea | Weight gain and decreased exercise and resume ovulation following these changes. If this is not successful, gonadotropins can be used in low doses. |
| Diminished ovarian reserve | Proceed to IVF |
| Unexplained infertilitya | Oral medications can be started to increase the number of oocytes and these can be used in conjunction with IUI to time ovulation. It is recommended to attempt this 3-6 times prior to starting IVF. |
a: The Fast Track and Standard Treatment Trial randomized women into two groups: 3 cycles of clomiphene-IUI followed by 3 cycles of clomiphene gonadotropins-IUI prior to IVF or 3 cycles of clomiphene-IUI followed by 6 cycles of IVF.32 Authors found the time to pregnancy was significantly shorter with the clomiphene to IVF group.32 Because of this, gonadotropin-IUI is not recommended for unexplained infertility.32
Frequently Asked Questions3
Do fertility medications cause birth defects?
In 2012, a meta-analysis of 46 studies that included 124,468 children who were conceived via IVF or ICSI was completed to compare risk of birth defects. A higher risk of birth defects was associated with ART (RR 1.37).33 A separate study in Australia that included 327,420 births did
not find an association between assisted conception and risk of birth defects (an exception was ICSI births). Further, no studies have found an increased risk between use of letrozole or clomiphene in rates of birth defects.34 A third meta-analysis found pregnancies from ART had a significantly higher risk of congenital malformation than spontaneous conceptions, but the risk was small and no absolute risk rates were provided in the study.35
Infertility itself places a woman at a higher risk for breast, endometrial, and ovarian cancers.3 However, it is unclear if undergoing fertility treatments incurs these same risks.3 One Cochrane review found women who used clomiphene citrate to conceive were at a higher risk of endometrial cancer than controls, but it is unclear if this was due to underlying medical conditions or the clomiphene itself.36 Available evidence regarding risk of ovarian cancer has not identified a strong association between use of these ovarian-stimulating drugs and this risk. Additionally, numerous systematic reviews have not found an association between risk of breast cancer and use of ovulation induction agents.3 Overall, there is currently no good evidence to suggest use of fertility medications increases a patient’s risk of breast, ovarian, or endometrial cancer.3
The Role of the Pharmacist
It is important for pharmacists to provide patient-centered care as part of multidisciplinary teams to maximize patient education and outcomes. To date, more than 100 pharmacies specialize in fertility therapies.6 Pharmacists can assist patients within 6 different realms related to fertility treatment. These include effectiveness, burden time, financial costs, potential risks, and genetic parentage.6 Provision of patient education is especially important considering how important medication therapy plays a role in treatment. With any regimen, patients may utilize several different medications and doses of these medications may change over the course of treatment depending on ovarian response.6 Demonstrating appropriate administration technique,
counseling on potential side effects, and assisting with affording these medications can help patients greatly.6
Pharmacists and pharmacy staff can also provide vital emotional support for patients undergoing infertility treatment.6 When patients feel knowledgeable and empowered regarding their regimen, this can help to alleviate stress and anxieties. Pharmacists and their staff can assist by anticipating urgently needed medications as doses and therapies change. They can also anticipate when patients may require referrals for emotional support, such as to RESOLVE: The National Infertility Association.37
Summary
Within the United States, an estimated 1 in 5 women are infertile. Defined as failure to achieve a pregnancy after 12 months of regular, unprotected sexual intercourse, infertility is a disease with not only health implications but important economic and social ramifications as well. Current guidelines recommend couples consider infertility treatments after 12 months of regular sexual intercourse with no resulting pregnancy.
Fertility evaluations should involve both partners, given the broad range of causes and high prevalence of unexplained infertility. Managing infertility from a nonpharmacologic perspective involves reducing risk factors that may contribute to infertility. Prior to initiating infertility treatment, it is important to manage identified underlying causes, including excess body weight, lack of exercise, poor diet, and medication use. Pharmacologic infertility treatments involve ovulation induction. It is important for pharmacists to provide patient- centered care as part of multidisciplinary teams to maximize patient education and outcomes.
Course Test
Which of the following ovulation disorders is caused by hypothalamic-pituitary failure?
Group 1 (Hypogonadotropic hypogonal anovulation)
Group 2 (Normo-gonadotropic, normo-estrogenic anovulation)
Group 3(Hyper gonadotropic, hypoestrogenic anovulation)
Group 4 (Hypogonadotropic, normo-estrogenic anovulation)
Unexplained infertility accounts for what percent of infertility cases?
5%
15%
25%
50%
Which of the following is a nonpharmacologic management strategy for infertility?
Exercise vigorously for more than 60 minutes a day
Take 5000 IU of vitamin D daily
Consume a low-fat, high-fiber diet
Avoid the use of folic acid and vitamin B12
Which of the following is true regarding in vitro fertilization (IVF)?
It is a procedure in which sperm is directly placed in the uterus
It requires the use of clomiphene citrate
It involves placing fertilized oocytes directly in the uterus
It is a low-cost method of treating infertility
Which of the following is true regarding clomiphene citrate?
The brand name of clomiphene citrate is Femara
The starting dose of clomiphene citrate is 10 mg daily for three days
Side effects of clomiphene citrate include hot flashes, gastrointestinal distress, and bloating
The use of clomiphene citrate is associated with a low incidence of twin pregnancies
Which of the following medications is recommended first-line for the treatment of infertility associated with PCOS?
Clomiphene citrate
Letrozole
Menotropins
Follitropin alpha
Which of the following gonadotropins is a mixture of purified FSH and LH in a 1:1 ratio?
Menopur
Gonal-f
Ovidrel
Follistim AQ
Which of the following infertility treatments is associated with the greatest risk of multiple (twins or more) pregnancies?
Clomiphene
Letrozole
Gonadotropins
Metformin
Women with hypothalamic amenorrhea would likely benefit most from which of the following medications?
Gonadotropins
Clomiphene citrate
Letrozole
Metformin
Which of the following are ways in which pharmacists can assist in the management of infertility?
Finances
Counseling on side effects
Educating on administration technique
All of the above
References
Infertility. Centers for Disease Control and Prevention. March 2022. https://www.cdc.gov/reproductivehealth/infertility/index.htm#:~:text= Is%20infertility%20a%20common%20problem,year%20of%20trying% 20(infertility). Accessed February 23, 2023
Dokras A, Hall JE. Infertility and Contraception. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson J. eds. Harrison's Principles of Internal Medicine, 21e. McGraw Hill; 2022.
Carson SA, Kallen AN. Diagnosis and Management of Infertility: A Review. JAMA. 2021;326(1):65-76. doi:10.1001/jama.2021.4788
American College of Obstetricians and Gynecologists Committee on Gynecologic Practice and Practice Committee. Female age-related fertility decline: committee opinion No. 589. Fertil Steril. 2014;101(3):633-634. doi:10.1016/j.fertnstert. 2013.12.032
Ordonez ND. Infertility. In: O'Connell M, Smith JA. eds. Women's Health Across the Lifespan, 2e. McGraw Hill; 2019.
Hutcherson NEC, Harris JB, Karaoui LR, et al. Infertility Management and Pharmacotherapy:What Every Pharmacist Should Know. J Pharm Pract. 2021;34(4):635-647. doi:10.1177/0897190020930969
National Collaborating Centre for Women’s and Children’s Health (UK). Fertility: Assessment and Treatment for People with Fertility Problems. London: Royal College of Obstetricians & Gynaecologists; 2013 Feb. (NICE Clinical Guidelines, No. 156.) 8, Ovulation disorders.
Delbaere I, Verbiest S, Tydén T. Knowledge about the impact of age on fertility: a brief review. Ups J Med Sci. 2020;125(2):167-174. doi:10.1080/03009734.2019.1707913Female repro anatomy
Wikicommons. Female Reproductive System. https://commons.wikimedia.org/wiki/Category:Human_female_reprodu ctive_system#/media/File:Vaginal_Ultrasound.png. Accessed February 10 2023.
Hall JE, Dokras A. Disorders of the Female Reproductive System. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson J. eds. Harrison's Principles of Internal Medicine, 21e. McGraw Hill; 2022.
El-Ibiary SY, Shrader SP, Ragucci KR. Contraception. In: DiPiro JT, Yee GC, Posey L, Haines ST, Nolin TD, Ellingrod V. eds. Pharmacotherapy: A Pathophysiologic Approach, 11e. McGraw Hill; 2020.
Reed BG, Carr BR. The Normal Menstrual Cycle and the Control of Ovulation. [Updated 2018 Aug 5]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.
Menstrual Cycle. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:MenstrualCycle2_en.svg. Accessed January 30, 2023.
Hall JE, Dokras A. Disorders of the Female Reproductive System. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson J. eds. Harrison's Principles of Internal Medicine, 21e. McGraw Hill; 2022.
Hakimi O, Cameron LC. Effect of Exercise on Ovulation: A Systematic Review. Sports Med. 2017;47(8):1555-1567. doi:10.1007/s40279-016- 0669-8
Gaskins AJ, Chavarro JE. Diet and fertility: a review. Am J Obstet Gynecol. 2018;218(4):379-389. doi:10.1016/j.ajog.2017.08.010
Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention. 2018. https://www.cdc.gov/mmwr/volumes/67/ss/ss6703a1.htm. Accessed February 23, 2023
Farquhar C, Marjoribanks J. Assisted reproductive technology: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2018;8(8):CD010537. Published 2018 Aug 17. doi:10.1002/14651858.CD010537.pub5
Lexicomp Online, Clomiphene. Waltham, MA: UpToDate, Inc.; January 24, 2023. https://online.lexi.com. Accessed February 23, 2023.
Yang AM, Cui N, Sun YF, Hao GM. Letrozole for Female Infertility. Front Endocrinol (Lausanne). 2021;12:676133. Published 2021 Jun 16. doi:10.3389/fendo.2021.676133
Lexicomp Online, Letrozole. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119-29. doi: 10.1056/NEJMoa1313517
Franik S, Eltrop SM, Kremer JA, Kiesel L, Farquhar C. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2018;5(5):CD010287. Published 2018 May 24. doi:10.1002/14651858.CD010287.pub3
Weiss NS, Kostova E, Nahuis M, Mol BWJ, van der Veen F, van Wely M. Gonadotrophins for ovulation induction in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;1(1):CD010290. Published 2019 Jan 16. doi:10.1002/14651858.CD010290.pub3
Lexicomp Online, Menopur. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Gonal f. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Follistim AQ. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Ovidrel. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Leuprolide. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Cetrorelix. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Lexicomp Online, Ganirelix. Waltham, MA: UpToDate, Inc.; February 9, 2023. https://online.lexi.com. Accessed February 23, 2023.
Reindollar RH, Regan MM, Neumann PJ, et al. A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril. 2010;94(3):888- 899.doi:10.1016/j.fertnstert.2009.04.022
Wen J, Jiang J, Ding C, et al. Birth defects in children conceived by in vitro fertilization and intracytoplasmic sperm injection: a meta-analysis. Fertil Steril. 2012;97(6):1331-1337. doi:10.1016/j.fertnstert.2012.02.0
Davies MJ, Moore VM, Willson KJ, et al. Reproductive technologies and the risk of birth defects. N Engl J Med. 2012;366(19):1803-1813. doi: 10.1056/NEJMoa1008095
Qin J, Wang H, Sheng X, Liang D, Tan H, Xia J. Pregnancy-related complications and adverse pregnancy outcomes in multiple pregnancies resulting from assisted reproductive technology: a meta-analysis of cohort studies. Fertil Steril. 2015;103(6):1492-508.e1, 7. doi:10.1016/j.fertnstert. 2015.03.018
Skalkidou A, Sergentanis TN, Gialamas SP, et al. Risk of endometrial cancer in women treated with ovary-stimulating drugs for subfertility. Cochrane Database Syst Rev. 2017;3(3):CD010931. doi:10 1002/14651858.CD010931.pub2
Resolve. National Infertility Association. https://resolve.org/about- us/#:~:text=RESOLVE%3A%20The%20National%20Infertility%20Asso ciation%2C%20established%20in%201974%2C%20is,advocacy%2C%2 0and%20inspired%20to%20act. Accessed February 23, 2023.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.