ERECTILE DYSFUNCTION MANAGEMENT
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson is an assistant professor of internal medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Topic Overview
Erectile dysfunction (ED) is the inability to maintain or achieve an erection satisfactory for intercourse. It is the most common cause of sexual dysfunction among men in the United States (US). An estimated 50% of men will experience some form of ED their lifetime, making this a significant medical problem. Patients with ED require a patient-centered, holistic approach to care that involves treating underlying conditions and improving the quality and number of erections while avoiding medication side effects. As accessible healthcare providers, pharmacists play an important role in identifying men requiring ED treatment, making referrals, and helping the care team to address medication-related causes of ED. Further, pharmacists can provide crucial counseling on the appropriate use of ED medications and help patients to mitigate side effects and avoid harmful drug interactions. This course will review the etiology and pathophysiology of ED and describe available treatment options in detail, including appropriate administration, mechanisms of action, side effects, and contraindications. The role of the pharmacist in caring for patients with ED will be discussed.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number: The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-039-H01-P
Pharmacy Technician 0669-0000-23-040-H01-T
Credits: 1 hour of continuing education credit
Type of Activity: Continuing education
Media: Internet/Home Study Fee Information: $4.99
Estimated time to complete activity: 1 hour, including Course Test and course evaluation
Release Date: March 18, 2023 Expiration Date: March 18, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From March 18, 2023, through March 18, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Describe the prevalence and underlying causes of erectile dysfunction
Compare and contrast phosphodiesterase-5 inhibitors
Recall indications, contraindications, side effect profiles, and monitoring parameters for erectile dysfunction treatments
Disclosures
The following individuals were involved in the development of this activity:
L. Austin Fredrickson, MD, FACP, and Susan DePasquale, MSN, PMHNP-BC. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
ⓒ RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Erectile dysfunction (ED) is the most common cause of sexual dysfunction among men in the United States. An estimated 50% of men will experience some form of ED their lifetime, making this a significant medical problem. Despite the growing social awareness and acceptance of this disorder, many men remain hesitant to discuss issues related to ED with their partners and healthcare providers. This course will review the etiology and pathophysiology of ED and describe available treatment options in detail, including appropriate administration, mechanisms of action, side effects, and contraindications. The role of the pharmacist in caring for patients with ED will be discussed.
Erectile Dysfunction: An Overview
Erectile dysfunction is the inability to maintain or achieve an erection satisfactory for intercourse.1 Patients with ED require a patient-centered, holistic approach to care that involves treating underlying conditions and improving the quality and number of erections while avoiding medication side effects. Further, ED is too frequently not prioritized over other health issues. This is concerning from a public health perspective, given ED often results from serious underlying conditions, including metabolic syndrome and cardiovascular disease.
As accessible healthcare providers, pharmacists play an important role in identifying men requiring ED treatment, making referrals, and helping the care team to address medication-related causes of ED. Further, pharmacists can provide crucial counseling on the appropriate use of ED medications and help patients to mitigate side effects and avoid harmful drug interactions.
Etiology
The causes of ED are numerous and can be vascular, neurologic, psychologic, or hormonal in nature.1 Many times, the development of ED is multifactorial, making it important for clinicians to determine underlying
etiologies. In older men, diabetes, atherosclerosis, and medications account for more than 80% of cases.1 Table 1 lists common causes of ED.
Table 1. Selected Causes of Erectile Dysfunction
| Etiology | Condition |
| Neurologic | Multiple sclerosis Stroke |
| Hormonal | Hypogonadism Thyroid disorders |
| Trauma | Spinal cord injuries |
| Metabolic | Diabetes mellitus |
| Psychologic | Depression Anxiety Post-traumatic stress disorder Substance use disorders |
| Other | Sleep apnea COPD CHF Urologic disorders Medications Glaucoma (correlated) |
Taken from Harrison's Principles of Internal Medicine1
The chance of developing ED increases with age, with prevalence estimated at 52% among men between the ages of 40 and 70, and 80% in men older than 70 years of age.2 This occurrence of ED may not be so much a result of advanced age but rather a product of medical conditions experienced by older patients and the medications used to manage them. Erectile dysfunction and metabolic syndrome are notably correlated.3 In patients with cardiovascular disease (CVD), ED has been called a sentinel symptom, and many of the same risk factors for CVD—including hypertension, obesity, and smoking—also increase the risk of developing ED.1,3 Additionally, people with diabetes mellitus are three times more likely to develop ED than those without.4 Psychological issues such as anxiety and depression can cause ED in isolation but also tend to occur alongside cardiovascular conditions.1,2
Many men experience feelings of anxiety, low self-esteem, and decreased masculinity, which can worsen ED.5
Medications may cause up to 25% of ED cases, and pharmacists can assist care teams in identifying medications that may cause or exacerbate ED.2,4 To determine if a particular drug is a cause of ED, pharmacists should look for an association between the start of the medication and the onset of ED.1 Antidepressants are one of the most notorious classes known to cause ED, in particular the selective serotonin reuptake inhibitors (SSRIs) citalopram, fluoxetine, paroxetine, and sertraline.2,4 Illicit drug use, tobacco, and use of alcohol can exacerbate ED as well.4 A more comprehensive list of medications associated with ED is included in Table 2.2
Table 2. Medications that Cause Erectile Dysfunction
| Medication Class | Examples |
| Diuretics and antihypertensive agents | Hydrochlorothiazide Benazepril Chlorthalidone Propranolol |
| Antidepressants | Fluoxetine Sertraline Citalopram Paroxetine |
| Antihistamines | Diphenhydramine Meclizine Promethazine |
| NSAIDs | Naproxen Indomethacin |
| H2-receptor antagonists | Cimetidine Famotidine |
Taken from Pharmacotherapy: A Pathophysiologic Approach, 11th ed.2
Erectile Dysfunction Pathophysiology
Understanding penile erection physiology and pathophysiology can assist clinicians in evaluating patients and determining appropriate treatment modalities. Penile erections involve a complex interaction between the central
nervous system (CNS), peripheral nervous system (PNS), and vascular and cavernosal smooth muscle in the penis.1,7 The penis is comprised of the corpora cavernosa and the corpus spongiosum.1,7 (See Figure 1.)6 For an erection to occur, the smooth muscle of the corpus cavernosum must relax and allow blood to flow into the penis.1 increased blood flow results in increased intra-cavernosal pressure, and venous outflow from the corpora cavernosa decreases.1,7
Figure 1. Anatomy of Male Reproductive System

Taken from WikiCommons6
To achieve an erection, the CNS must coordinate sensory information from visual, auditory, tactile, and imaginative sources.7 Within the PNS, the neurotransmitter nitric oxide (NO) is released from parasympathetic nerve terminals and activates guanylate cyclase (sGC).7 This is depicted in Figure 2 below.8
Activation of sGC causes an increase in intracellular levels of cyclic 3′,5′- guanosine monophosphate (cGMP), which activates subsequent second messenger systems to produce cavernosal smooth muscle relaxation.1,7 cGMP is later metabolized by an enzyme called phosphodiesterase-5 (PDE-5).7 The vasoactive prostaglandins PGE1 and PFG2a, which are made within cavernosal tissue, also cause the relaxation of cavernosal smooth muscle cells.1,7
Figure 2. Nitric Oxide Pathway
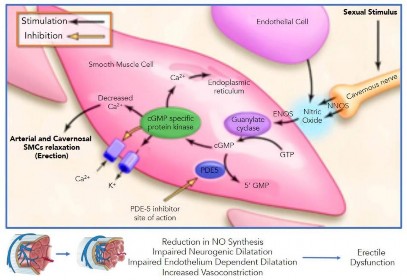
Taken from Sangiorgi, et al. (2021)8
Three different mechanisms contribute to ED: 1) a failure to initiate, which can be psychogenic, hormonal, or neurogenic in nature, 2) a failure to fill, which is an arterial issue, and 3) a failure to store blood volume, which results from veno-occlusive dysfunction.1 Erectile dysfunction is typically a result of endothelial dysfunction secondary to decreased synthesis and/or activity of NO.1
Diagnosing Erectile Dysfunction
The 2018 American Urological Association (AUA) Erectile Dysfunction guidelines offer clinician strategies for both the diagnosis and treatment of ED.9 Clinicians should be cognizant of initiating this topic as many patients are often embarrassed or hesitant to start the conversation. A medical history, including a thorough sexual and psychosocial history, should be obtained.9 A current list of medications, including over-the-counter and prescription drugs, should be obtained as well.9 Validated questionnaires are available to assess the severity of ED and determine the effectiveness of treatment. These include the International Index of Erectile Function (IIEF) and the Sexual Health Inventory for Men or SHIM.9
The IIEF is the most widely used index for evaluating men's sexual issues.10 It evaluates erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction.10 A shorter version known as IIEF-5 evaluates ED specifically.10 The IIEF-5 is depicted in Figure 3.11
Figure 3. IIEF-5
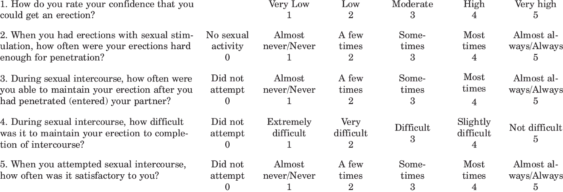
Taken from Roberson, et al. (2013)11
The Prostate Cancer Foundation provides the SHIM, adapted from Rosen, et al. (1999) IIEF-5.12 The SHIM asks the following: Over the past six months:
How do you rate your confidence that you could get and keep an erection?
Very low
Low
Moderate
High
Very high
When you had erections with sexual stimulation, how often were your erections hard enough for penetration (entering your partner)?
No sexual activity
Almost never or never
A few times (much less than half the time)
Sometimes (about half the time)
Most times (much more than half the time)
Almost always or always
During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner?
Did not attempt intercourse
Almost never or never
A few times (much less than half the time)
Sometimes (about half the time)
Most times (much more than half the time)
Almost always or always
During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse?
Did not attempt intercourse
Extremely difficult
Very difficult
Difficult
Slightly difficult
Not difficult
When you attempted sexual intercourse, how often was it satisfactory for you?
Did not attempt intercourse
Almost never or never
A few times (much less than half the time)
Sometimes (about half the time)
Most times (much more than half the time)
Almost always or always
Total:
| SHIM Scores | You may have |
| 1-7 | Severe ED |
| 8-11 | Moderate ED |
| 12-16 | Mild to Moderate ED |
| 17-21 | Mild ED |
| 22-25 | No signs of ED |
The score from each question above is added together for a total score.
A lower score indicates a potentially more severe case of ED.11
A physical examination should be completed that includes a genital examination and measuring blood pressure and BMI.1,4 Depression and substance use screening may also be administered.1,4 Lab testing may include fasting glucose levels and/or a hemoglobin A1C level, lipid panel, and thyroid stimulating hormone level.4 Total testosterone levels should be measured only if clinically indicated.4 If an underlying cause is not obvious, physicians can consider cardiac stress testing, further neurologic, endocrine, or psychological testing, or a sexual health evaluation. The decision to pursue specialized testing should be balanced with potential costs, invasiveness, patient motivation, and impact on treatment.1
Treating Erectile Dysfunction
The goals of treating ED are 1) to improve both the quality and quantity of penile erections to an extent that is satisfactory to the patient and their partner(s) 2) to improve overall physical health, and 3) to optimize quality of life and well-being.1 A reasonable understanding of the expectations of therapy should be discussed with the patient.1 Healthcare providers should strive to provide treatment that is well-tolerated by the patient and affordable.
The 2018 AUA guidelines offer treatment recommendations for men with ED. Notably, the panel does not promote using a treatment framework that involves a progression from the least to most invasive treatment option.9 The guidelines state any initial treatment is valid, given the patient understands the risks and benefits associated with their choice.9
A general treatment approach should begin with identifying the underlying causes of ED and managing these to optimize the overall health of the patient.9 Medications should be reviewed, and contributory agents changed or modified if possible. Prior to initiating pharmacologic ED therapy, it is useful for patients to first attempt lifestyle modifications, including optimizing diet and exercise regimens, as well as stress management.1,9 It is
recommended men engage in regular exercise, lose weight if overweight or obese, maintain good control of diabetes and blood pressure, and consume a healthy diet.9 The use of statins may improve IIEF-5 scores, which can be a helpful motivating tool when treating or preventing co-occurring atherosclerotic cardiovascular disease.13 Smoking cessation should also be encouraged, given the risk of ED increases by more than 50% in smokers and 20% in ex-smokers.4
Pharmacologic treatments, including phosphodiesterase-5 inhibitors (PDE5is), prostaglandin E1s, and testosterone can be considered on a patient- specific basis. These pharmacologic agents are described in more detail below. Broadly, an optimal treatment will be convenient, effective, have a fast onset, low incidence of side effects, avoid drug interactions, and be cost-effective for the patient.2
Phosphodiesterase-5 Inhibitors
Phosphodiesterase-5 inhibitors were not initially developed to manage ED. Sildenafil was the first to be studied for use in coronary heart disease, and it was through these trials that sildenafil was discovered to have beneficial effects on penile erections.14 Viagra®, the brand name of sildenafil, was FDA- approved for the treatment of ED in 1998.14 Within the next 14 years, three other agents—Cialis® (tadalafil), Levitra® (vardenafil), and Stendra® (avanafil)—would be approved.14 Sildenafil became the first generic PDE5 inhibitor in 2017.14
Mechanism of Action and Pharmacokinetics
Phosphodiesterase-5 inhibitors affect the response to sexual stimulation rather than directly causing penile erections.14 They exert their effects by inhibiting the phosphodiesterase 5 enzyme from breaking down cGMP.15 When sexual stimulation causes the release of NO, this inhibition of PDE-5 leads to increased levels of cGMP in the corpus cavernosum, smooth muscle relaxation, and inflow of blood to the corpus cavernosum.15 Notably, PDE5is do not have
an effect in the absence of sexual stimulation at recommended doses.15 They also may not be effective in men with severe ED.4
Dosing for PDE5is is detailed in Table 3. Pharmacists should note higher doses of the PDE5is generally do not produce clinically significant benefits for ED but often lead to increased adverse reactions.9 Because of this, it is suggested men use the lowest dose that produces acceptable outcomes.9 Doses should be titrated up or down depending on patient response and occurrence of side effects until an optimal dose is achieved.9 Dose reductions or medication weaning can be considered in men with ED of psychogenic origin once related issues have been resolved.9 Generic versions of sildenafil can also be found in the 20mg tablets historically for pulmonary hypertension dosing, but using these for ED may not only be more affordable but allow for greater flexibility with titration.
Table 3. Dosing of Phosphodiesterase-5 Inhibitors
| Generic (Brand) | Initial Dose | Max Dose | Dose Reductiona |
| Sildenafilb (Viagra) | 50 mg once daily as needed 1 hour before sexual activity | 100 mg | 25 mg |
| Avanafil (Stendra) | 100 mg 15 minutes before sexual activity | 200 mg | 50 mg 30 minutes prior to sexual activity |
| Tadalafil (Cialis)c | 10 mg 30 minutes or more before sexual activity | 20 mg | 5 mg |
| Tadalafild (Cialis) | 2.5 mg daily | 5 mg | --- |
| Vardenafil (Staxyn)e | 10 mg 1 hour before sexual activity | 10 mg per day | --- |
| Vardenafil (Levitra) | 10 mg 1 hour before sexual activity | 20 mg per day | 5 mg |
aIf needed due to side effects
bTitrate to a dose that causes an erection for no longer than 1 hour
cAs needed dosing
dDaily dosing
eDo not substitute Stayxn for Levitra
Table 3 compiled from Lexicomp UpToDate (2023) for Sildenafil,15 Avanafil,16 Tadalafil,17 Varenafil18
While all PDE5is are similarly efficacious, they vary in their onsets, potencies, and durations of action (Table 4).14 For example, tadalafil has a longer half-life and thus may be taken up to 12 hours before sex, or even daily, at a low dose.14 Pharmacists should recognize important differences between PDE5is to select the best agent, especially advising patients on the expected onset of action.
Table 4. Pharmacokinetic Properties of PDE5 Inhibitors
| Generic (Brand) | Onset | Duration | Metabolism | Effect of food intake |
| Sildenafil (Viagra) | 30-60 mins | Up to 12 hours | Hepatic via CYP3A4 and CYP2C9 | High-fat meals decrease efficacy |
| Avanafil (Strendra) | 15-30 min | Up to 6 hours | Hepatic via CYP3A4 and CYP2C9 | Not affected |
| Tadalafil (Cialis) | 1-2 hours | Up to 36 hours | Hepatic via CYP3A4 | Not affected |
| Vardenafil | 30-60 mins | Up to 10 hours | Hepatic via CYP3A4 and CYP2C9 | High-fat meals decrease efficacy |
Table 4 compiled from Lexicomp UpToDate (2023) for Sildenafil,15 Avanafil,16 Tadalafil,17 Varenafil18
Renal and Hepatic Dosing Considerations
Patients with a creatinine clearance (CrCl) under 30 mL/min or those with severe hepatic impairment should begin sildenafil at a dose of 25 mg.15 Vardenafil (Levitra) does not require dose adjustment for those with decreased creatinine clearance, but patients with modest hepatic impairment should start with the 5 mg dose, and those with severe hepatic impairment should avoid use of vardenafil.18 Vardenafil (Staxyn) does not require dose adjustment for either impaired renal function or mild impaired hepatic function.18 It should not be used in those with severe hepatic impairment, however.18
Tadalafil should be started at 10 mg every 48 hours in patients with a CrCl between 30 and 50 mL/min and 5 mg every 72 hours in those with CrCl less than 30 mL/min.17 Patients with mild-moderate hepatic impairment should start tadalafil at 10 mg every 24 hours, and use should be avoided in cases of severe hepatic impairment.17 Avanafil does not require dose adjustments for mild-moderate hepatic impairment or for a CrCl between 30 and 90 mL/min.16 It is not recommended in those with a CrCl under 30 mL/min or if the patient has severe hepatic disease.16
Geriatric Dosing Considerations
For patients older than 65 years, it is recommended to start sildenafil at a dose of 25 mg.15 Vardenafil (Levitra) should be started at a dose of 5 mg in patients older than 65 years of age.18 Vardenafil (Staxyn) and tadalafil do not require dose adjustments for patient 65 years or older.18
Adverse Effects
Use of PDE5is generally results in mild-to-moderate adverse effects.15 Frequently, these include dyspepsia, headache, flushing, back pain, myalgia, and dizziness.15 While rates of dyspepsia and dizziness are similar among these medications, sildenafil and vardenafil are associated with higher rates of headache and flushing.9 Use of daily dosing of tadalafil is associated with lower rates of adverse effects compared to on-demand use.9 Men who are post-radical prostatectomy and post-radiation therapy may experience higher rates of adverse effects than those in the general ED population.9
More serious adverse effects of PDE5is included prolonged erection (erections lasting longer than 4 hours), priapism (prolonged, painful erections), and nonarteritic anterior ischemic optic neuropathy (NAION).15 NAION is a rare condition in which vision loss in one eye occurs suddenly. Risk factors include men older than 50, small optic discs with low cup-to-disc ration, and Caucasian ethnicity.15 The absolute risk is small (3 cases per 100,000 men 50 years or older), but patients should be counseled on NAION.9,15
Drug and Food Interactions
Various drug and food interactions have been noted for PDE5is. Most notably, men prescribed regular use of nitrates should not use PDE5is.15-18 This is because combining PDE5is with nitrate-containing medications may result in large drops in blood pressure.15-18 If sublingual nitroglycerin is used for angina, PDE5i use should be avoided for 24 hours and longer for tadalafil. Other longer-acting nitrate agents (isosorbide mononitrate/dinitrate, etc.) should similarly be avoided.
Interactions between CYP3A4 inhibitors (ketoconazole and erythromycin) and the PDE5is may occur.15-18 Table 5 details dosing when CYP3A4 inhibitors and PDE5is are taken concurrently.
Table 5. PDE5i Drug Dosing with CYP3A4 Inhibitors
| Agent | Modified Dose |
| Sildenafil | 25 mg |
| Vardenafil | 2.5 mg every 24 hours |
| Vardenafil (Staxyn) | Avoid use |
| Tadalafil (on demand) | 10 mg every 72 hours |
| Tadalafil (daily) | 2.5 mg |
| Avanafil | Avoid use with potent inhibitors. Limit dose to 50 mg every 24 hours with moderate inhibitors. |
Table 5 compiled from Lexicomp UpToDate (2023) for Sildenafil,15 Avanafil,16 Tadalafil,17 Varenafil18
Patients should be counseled that taking sildenafil with high-fat foods can decrease absorption.15 Patients should also avoid concurrent use of grapefruit juice.14 Vardenafil (Levitra) should be avoided with concurrent use of Type1A or Type 3 antiarrhythmics.18 Hypertension may result if PDE5is are administered concomitantly with antihypertensive agents or alcohol.15-18 Finally, vardenafil is not recommended if patients have congenital prolonged QT intervals.18
Patient Monitoring
Clinicians can assess the efficacy of PDE5i therapy following a trial of several weeks using one agent.9 The degree of satisfaction with any agent is patient-specific, so patients must be highly involved in shared decision- making. If patients have not seen improvement in the quality and quantity of erections, the dose can be increased (up to the maximum tolerated dose) or the patient can be switched to a different drug.9 Other treatment modalities may also be explored.9
General monitoring parameters for PDE5is include monitoring blood pressure and heart rate in those concurrently using antihypertensive agents and monitoring for pulmonary edema.15-18
PDE5i Efficacy
The PDE5is have been studied extensively, with research including men in the general ED population and those with comorbidities such as diabetes, benign prostatic hyperplasia, and post-spinal cord injury.9 Within the literature, the IIEF is commonly used to evaluate efficacy, and the magnitude of changes from pre-treatment to post-treatment scores is similar among all agents.9 There is notably limited data comparing these agents to each other. A 2013 review of 118 trials found PDE5is were superior to placebo in improving ED.19 Avanafil was less effective compared to tadalafil and vardenafil for question one on the Global Assessment Questionnaire.19 Within the erectile function domain of the IIEF, tadalafil was found to be more effective than vardenafil.19 No major differences were noted for the agents in terms of safety.19 Within this review, tadalafil was found to be the most effective PDE5i.19 Comparisons within this review were determined to be of low-grade evidence due to poor original reporting and indirect comparisons.14
In a 2017 meta-analysis, tadalafil and sildenafil were directly compared for use in the treatment of ED.20 Sixteen trials included in the analysis found tadalafil and sildenafil were similarly efficacious and had the same rate of side effects.20 Tadalafil was associated with lower rates of flushing, but higher rates
of back pain and myalgia compared to sildenafil.20 Tadalafil improved psychological outcomes over sildenafil and patients also preferred tadalafil over sildenafil.20 There were no differences in adherence rates between the two medications.20 This analysis suggests tadalafil may be a preferred choice for patients, but the choice should be patient-driven.
Counseling
Counseling patients on the appropriate use of PDE5is is crucial. It should be emphasized that sexual stimulation is necessary for PDE5is to take effect. Further, more than one trial with the medication is typically needed to see an effect. Patients should understand both the onset and duration of action of their medication. Studies have found men who report a non-response to PDE5is have used them incorrectly, either from a lack of sexual stimulation or taking them with a large meal, and this misuse may account for up to 81% of treatment failures.9
Prostaglandin E1
A second ED treatment option is alprostadil (Caverject, Caverject Impulse, Edex, and Muse).21 Alprostadil is prostaglandin E1 and may be reasonable for men with contraindications to PDE5is and those who prefer to not use oral medications.9 While 60% of men respond well to PDE5is, this responsiveness can decrease as ED progresses and alprostadil may be a useful option in these cases.9
Mechanism of Action and Dosing
Alprostadil causes vasodilation via direct effects on vascular and ductus arteriosus smooth muscle.21 It also relaxes trabecular smooth muscle via dilation of cavernosal arteries when injected along the penile shaft, which allows blood to flow and become entrapped in the lacunar space of the penis.21
Alprostadil can be given via intracavernosal injection (ICI) or the intraurethral (IU) route.21 For treatment of erectile dysfunction, the dose of ICI alprostadil must be titrated carefully and done within a healthcare setting.9,21 If the dose does not elicit a response, the patient can be re-dosed within 1 hour.21 If no response results, a one-day interval should be given before the next dose is given.21 The lowest effective dose should be used.9 Higher doses are often associated with increases in pain and discomfort.9 Doses for Caverject, Caverject Impulse, and Edex are detailed in Table 6.
Table 6. Alprostadil Intracavernosal Dosing
| Etiology | Initial Dose | Titration | Maintenance Dose |
| Vasculogenic, psychogenic, mixed etiology | 2.5 mcg | Partial response: give another 2.5 mcg dose. Can titrate in increments of 5-10 mcg 24 hours apart until adequate reached
No response: give second dose of 7.5 mcg within 1 hour | Once an appropriate dose is reached, the patient can self- administer injections no more than 3 times/week with 24 hours minimally in between doses |
| Neurogenic | 1.25 mcg | Partial response: give another 1.25 mcg dose within 1 hour. Can titrate to another dose of 5 mcg 24 hours later. Repeat as needed until optimal dose reached |
Taken from Lexicomp UpToDate (2023) for Alprostadil21
Administration of alprostadil will vary depending on the product.21 To administer Caverject, the intended side of injection should be wiped with an alcohol swab prior to injection.21 A 1/2 inch, 29- or 30-gauge needle should be used to inject the medication into the dorsolateral aspect of the proximal third of the penis, avoiding visible veins; alternate side of the penis for injections.21 The site of injection should be compressed with an alcohol swab or sterile gauze for 5 minutes after administration.21
Caverject Impulse is supplied as a disposable, single-dose, dual chamber syringe system.21 The intended injection site should be wiped with an alcohol swab prior to injection. After attaching the provided needle assembly, the dose should be selected and injected into the dorsolateral aspect of the proximal third of the penis, avoiding visible veins, and alternate side of the penis should be used for injections.21 The site of injection should be compressed with an alcohol swab or sterile gauze for 5 minutes after administration.21
To administer Edex, the intended injection site should be wiped with an alcohol swab prior to injection. A 1/2 inch, 27- to 30-gauge needle should be used.21 Edex should be injected into the dorsolateral aspect of the proximal third of the penis, avoiding visible veins, and alternating sides of the penis should be used for injections.21 Administration should occur over a 5- to 10- second interval.21 The site of injection should be compressed with an alcohol swab for 5 minutes after administration.21
Intraurethral alprostadil (Muse) involves inserting a delivery catheter into the meatus and depositing a pellet of alprostadil in the urethra.9,21 Initial dosing of IU alprostadil is between 125 mcg and 250 mcg, and this dose can be increased or decreased in a stepwise fashion until sufficient erection for intercourse is achieved.21 Maintenance doses are given as needed to achieve an erection.21 No more than two systems should be used within 24 hours.21 Administration should occur immediately after urination.21 To place the product, it should first be removed from the foil pouch and protective cover. The penis should be slowly stretched to its full length, with gentle compression from the top to bottom of the glans.21 The Muse stem should be slowly inserted
into the urethra up to the collar.21 Next, the button at the top should be gently pressed until it stops and the applicator left in place for 5 seconds.21 The applicator should be gently rocked side to side and then removed while the penis is kept upright.21 If residual medication remains at the end of the applicator, the process should be repeated.21 Once the applicator is successfully removed, the penis should be held upright and stretched to its full length, and then rolled firmly between hands for 10 seconds. Erections may be increased by standing or walking for 10 minutes after administration to increase blood flow.21
Adverse Reactions
Adverse reactions associated with intracavernosal injections include penile pain, hypertension, dizziness, headache, prolonged erection (lasting more than 4 hours), and injection site hemorrhage.21 The risk of priapism is 0.4%.21 Patients with sickle cell disease, multiple myeloma, severe coagulopathy, poor manual dexterity, severe venous incompetence, severe cardiovascular disease, or Peyronie’s disease should not use alprostadil intracavernosal injection.21
Intraurethral side effects include penile pain and urethral burning, dizziness, headache, testicular pain, leg pain, perineal pain, and tachycardia.21
Patient Monitoring
For both formulations of alprostadil, the lowest effective dose should be used in older adult patients.21 There are no dose adjustments required for those with altered kidney or hepatic function.21 Monitoring of alprostadil includes blood pressure, respiratory rate, heart rate, temperature, penile pain, duration of erection, signs of infection, and signs of penile fibrosis.21
Alprostadil Efficacy
Studies have found the efficacy of IU alprostadil (noted by successful intercourse) ranges from 29-78% and efficacy rates for the ICI approach are
between 53 and 100%.9 Intraurethral alprostadil has demonstrated greater efficacy compared to placebo in two placebo-controlled studies.9 In studies comparing IU and ICI alprostadil, success rates were higher in the ICI group, and in general IU alprostadil is less effective than ICI alprostadil.9
Testosterone
By age 70, approximately 30% of men have low testosterone levels, and men with low testosterone (levels less than 300 ng/dL) are more likely to have ED than men with normal testosterone levels.22 Per the AUA, testosterone should not be prescribed to men with ED who have normal testosterone levels, and routine monitoring of testosterone is controversial.4,9 A number of randomized control trials have found when testosterone is given to men with low testosterone, improvements in ED are seen and many studies have found testosterone levels and erectile function are positively correlated.22 However, the AUA guidelines advised testosterone is not effective as monotherapy for ED.9 The guidelines do suggest men with total testosterone levels < 300 ng/mL who are considering PDE5i treatment should be counseled that testosterone therapy in combination with a PDE5i may be more effective than a PDE5i alone.9 Within trials, men who received combination therapy reported better erectile function scores than those who used either a PDE5i or testosterone alone.9
Dosing and Administration
Testosterone dosing for various dosage forms is detailed in Table 7.2,23
Table 7. Testosterone Dosing
| Agent | Brand Name | Dose | Dose Adjustments |
| Testosterone buccal system | Striant | 30 mg Q12H | None |
Testosterone cypionate intramuscular injection | Depo- Testosterone | 200-400 mg every 2-4 weeks | None |
Testosterone enanthate intramuscular injection | Delatestryl | 200-400 mg every 2-4 weeks | None |
| Testosterone undecanoate intramuscular injection | Aveed | 750 mg single dose | None
Contraindicated in patients with serious renal and hepatic disease |
| Testosterone patch | Androderm | 4 mg as single dose at bedtime | None |
| Testosterone gel | AndroGel 1% and Testim 1% | 5-10 g of gel (equivalent to 50-100 mg testosterone) as single morning dose | None |
| Testosterone transdermal spray | Fortesa 2% (10 mg/actuation) | 4 sprays (equal to 40 mg testosterone) every morning | None |
| Testosterone transdermal solution | Axiron (30 mg/actuation) | One pump spray equal to 30 mg testosterone to left or right axilla daily | None |
| Testosterone subcutaneous implant pellet | Testopel | 150-450 mg (equal to 2-6 pellets) as single dose every 3-6 months | None |
Table 7 compiled from Pharmacotherapy: A Pathophysiologic Approach, 11th ed.,2 and Lexicomp UpToDate (2023) for Testosterone23
Buccal testosterone should be timed so the buccal system is removed prior to brushing teeth in both the morning and evening.2 The buccal system should be placed just above the incisor tooth in the mouth and then held in place for 30 seconds to allow it to adhere.2 To remove the system, it should be slid down toward the tooth.2 The site of administration should be rotated with each dose to the alternate side of the mouth. If the tablet becomes
detached during eating, it should be discarded and replaced with a new buccal system. It should not be chewed or swallowed.2
Testosterone implant pellets come in a sterile implanter kit and should only be administered by trained healthcare professionals. The dose is administered by making an incision in the forearm and implanting the dose subcutaneously under local anesthesia.2 The onset of clinical improvement is between 3 and 4 months.2
Testosterone transdermal solutions should only be applied to the axilla. Antiperspirant should be applied prior to applying Axiron.2 Patients should avoid activities such as swimming, washing, showering, or washing the site of administration for a minimum of 2 hours after application.2 Axiron requires a Risk Evaluation and Mitigation Strategy (REMS) assessment to be submitted to the Food and Drug Administration (FDA).2
Testosterone transdermal spray is applied by first priming the pump by pushing it down three times.2 The medication can only be applied to either the front or inner thighs.2 The site of application should be covered to order transferring the medication to others. As with the solution, patients should avoid swimming, showering, or washing the administration site for 2 hours after administration of the spray. REMS assessment should be submitted to the FDA.2
The administration of the gel is similar to the spray in that the area of application should be covered and should not be allowed to get wet for 2 hours after administration.2 Patients should follow the product labeling regarding sites of application. Androgel can be applied to the shoulders, upper arms, or abdomen, and Testim to the shoulder or upper arms only.2 The gels are available in pre-measured dose packs and a pump dispenser. REMS assessments need to be submitted to the FDA.2
Patient Counseling
Patients should be cautioned that use of injection products can result in supraphysiological serum levels of testosterone produced during the dosing interval and these have been linked to changes in mood.9 Patients using topical testosterone products, should be counseled that women and children should avoid contact with unwashed or unclothed application sites, and patients should thoroughly wash their hands following administration of the product.2
The Role of the Pharmacist
Pharmacists are accessible care providers who can play an important role in treating patients with ED. Pharmacists can assess patients and refer them to primary care providers for further treatment. They can also provide education on ED medications, including appropriate use, how to recognize and mitigate side effects, and avoidance of drug-drug interactions. Further, research suggests there may be a role in the future for community pharmacies to serve as a hub for men to complete initial ED evaluations and consultations to determine suitability of treatment.24 In this scenario, men would be referred out for treatment of the underlying causes of their ED.24 Online pharmacies can also serve as user-initiated ED evaluation sites, in which visitors would complete a questionnaire electronically to determine suitability and those identified as having ED would then be directed to an appropriate health care provider for follow-up.24 This has obvious regulatory concerns but can greatly expand accessibility of care for men who suffer with ED.24 Regardless of site or mechanism of contact, pharmacists can screen, empathize, and discuss honestly this common condition with professionalism and sensitivity. This is one area where pharmacologic counseling and treatment can make an immediate and significant improvement in patient lives.
Summary
Erectile dysfunction is the inability to maintain or achieve an erection satisfactory for intercourse.1 Patients with ED require a patient-centered,
holistic approach to care that involves treating underlying conditions and improving the quality and number of erections while avoiding medication side effects. Further, ED is too frequently not prioritized over other health issues. This is concerning from a public health perspective, given ED often results from serious underlying conditions, including metabolic syndrome and cardiovascular disease.
As accessible healthcare providers, pharmacists play an important role in identifying men requiring ED treatment, making referrals, and helping the care team to address medication-related causes of ED. Further, pharmacists can provide crucial counseling on the appropriate use of ED medications and help patients to mitigate side effects and avoid harmful drug interactions.
Course Test
What percentage of men are estimated to experience erectile dysfunction (ED) at some point in their life?
10%
25%
50%
100%
Which of the following conditions should be considered as a possible cause of erectile dysfunction?
Depression
Rosacea
Tinnitus
Allergic rhinitis
Which of the following classes of medications is most likely to cause or worsen ED?
Antifungals
Selective serotonin reuptake inhibitors (SSRIs)
GLP-1 agonists
Proton pump inhibitors
Which class of medications is contraindicated to co-administer with sildenafil?
Nitrates, including sublingual nitroglycerine or isosorbide mono/di- nitrate
Beta-blockers, including propranolol or atenolol
Insulin, including long- and short-acting formulations
Steroids, including solumedrol and prednisone
Which PDE5 inhibitor has the longest half-life?
Sildenafil
Vardenafil
Tadalafil
Avanafil
Which PDE5 inhibitor can be dosed on an as-needed or daily basis?
Sildenafil
Vardenafil
Tadalafil
Avanafil
Which of the following considerations is most accurate regarding PDE5i dosing?
Higher initial doses should be considered for geriatric patients
Sildenafil should be started at a dose of 25 mg for patients with a CrCL < 80 mL/min
Tadalafil does not require dose adjustment for mild-moderate hepatic impairment
Concurrent use of CYP3A4 inhibitors may necessitate alternative PDE5i drug dosing
Which of the following medications is an injectable prostaglandin E1?
Alprostadil
Sildenafil
Tadalafil
Testosterone
Use of alprostadil is associated with which of the following adverse reactions?
Hypotension
Penile pain
Maculopapular rash
Nystagmus
A 55-year-old patient returns to care with concerns that his medication is ineffective. He took 50mg of sildenafil 5 minutes before his sexual encounter and did not see any immediate results which angered him. Which of the following steps is most reasonable?
Decrease the dose of sildenafil to 25mg
Advise the patient on the expected time lapse between taking a dose and seeing a response
Change from sildenafil to injectable alprostadil
Begin testosterone replacement therapy
References
McVary KT. Sexual Dysfunction. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson J. eds. Harrison's Principles of Internal Medicine, 21e. McGraw Hill; 2022.
Lee M, Sharifi R. Erectile Dysfunction. In: DiPiro JT, Yee GC, Posey L, Haines ST, Nolin TD, Ellingrod V. eds. Pharmacotherapy: A Pathophysiologic Approach, 11th ed. McGraw Hill; 2020.
Sanchez E, Pastuszak AW, Khera M. Erectile dysfunction, metabolic syndrome, and cardiovascular risks: facts and controversies. Transl Androl Urol. 2017;6(1):28-36. doi:10.21037/tau.2016.10.01
Rew K and Heidelbaugh J. Erectile dysfunction. Am Fam Physician. 2016;94(10):820-827
Snoga J, Williams B, Courtney L. Erectile dysfunction overview and treatment considerations in special populations. US Pharm. 2022;47(6):18-22.
Male reproductive system. WikiCommons. 2023. https://en.wikipedia.org/wiki/Male_reproductive_system. Accessed February 8, 2023.
Muneer A, Kalsi J, Ralph D. Erectile Dysfunction Part I: pathophysiology and risk factors. Urology News. 2014. https://www.urologynews.uk.com/features/synopsis/post/erectile- dysfunction-part-i-pathophysiology-and-risk-factors. Accessed February 8, 2023.
Sangiorgi G, Cereda A, Benedetto D, et al. Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review. Biomedicines. 2021;9(4):432. Published 2021 Apr 16. doi:10.3390/biomedicines9040432
Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline [published correction appears in J Urol. 2022 Mar;207(3):743]. J Urol. 2018;200(3):633-641. doi:10.1016/j.juro.2018.05.004
Vallejo-Medina P, Saffon JP, Álvarez-Muelas A. Colombian Clinical Validation of the International Index of Erectile Function (IIEF-5). Sex Med. 2022;10(1):100461. doi:10.1016/j.esxm.2021.100461
Roberson DW, Kosko DA. Men living with HIV and experiencing sexual dysfunction: an analysis of treatment options. J Assoc Nurses AIDS Care. 2013;24(1 Suppl):S135-S145. doi:10.1016/j.jana.2012.08.010
The Sexual Health Inventory for Men Questionnaire. The Prostate Cancer Foundation. Undated. https://www.pcf.org/c/the-sexual-health- inventory-for-men-shim-questionnaire/. Accessed February 8, 2023.
Kostis JB, Dobrzynski JM. The effect of statins on erectile dysfunction: a meta-analysis of randomized trials. J Sex Med. 2014;11(7):1626-1635.
Murphy M, Demers J, Ostroff J. Oral PDE5 inhibitors for erectile dysfunction. US Pharm. 2018;43(6):29-33.
Sildenafil. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/sildenafil-drug- information?search=Sildenafil.%20Lexicomp&source=search_result&sel ectedTitle=2~150&usage_type=default&display_rank=2. Accessed February 8 2023.
Avanafil. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/avanafil-drug- information?search=Avanafil%20Lexicomp&source=search_result&selec tedTitle=1~150&usage_type=default&display_rank=1. Accessed February 8 2023.
Tadalafil. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/tadalafil-drug- information?search=Tadalafil%20Lexicomp&source=search_result&sele ctedTitle=1~150&usage_type=default&display_rank=1. Accessed February 8 2023.
Varenafil. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/vardenafil-drug- information?search=Varenafil%20Lexicomp&source=search_result&sele ctedTitle=1~150&usage_type=default&display_rank=1. Accessed February 8 2023.
Yuan J, Zhang R, Yang Z, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. Eur Urol. 2013;63(5):902-912. doi:10.1016/j.eururo.2013.01.012
Gong B, Ma M, Xie W, et al. Direct comparison of tadalafil with sildenafil for the treatment of erectile dysfunction: a systematic review and meta- analysis. Int Urol Nephrol. 2017;49(10):1731-1740. doi:10.1007/s11255-017-1644-5
Alprostadil. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/alprostadil-drug- information?search=Alprostadil%20Lexicomp&source=search_result&sel ectedTitle=1~150&usage_type=default&display_rank=1. Accessed February 8 2023.
Rizk PJ, Kohn TP, Pastuszak AW, Khera M. Testosterone therapy improves erectile function and libido in hypogonadal men. Curr Opin Urol. 2017;27(6):511-515. doi:10.1097/MOU.0000000000000442
Testosterone. Lexicomp. UpToDate. 2023. https://www.uptodate.com/contents/testosterone-drug- information?search=Testosterone%20Lexicomp&source=search_result& selectedTitle=5~150&usage_type=default&display_rank=5. Accessed February 8 2023.
Taylor DG, Giuliano F, Hackett G, et al. The pharmacist's role in improving the treatment of erectile dysfunction and its underlying causes. Res Social Adm Pharm. 2019;15(5):591-599. doi:10.1016/j.sapharm.2018.07.014
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
ⓒ RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.