A NEW SPIN ON MIXOLOGY: MECHANISMS AND CONSEQUENCES OF DRUG-ALCOHOL INTERACTIONS
KELSEY GIARA, PharmD, RPh
Kelsey Giara is a pharmacist and freelance medical writer based in New Hampshire. She writes about a variety of healthcare topics for various publications and has significant experience in continuing medical education, needs assessments, grant writing, and medical communications.
Topic Overview
Alcohol has the potential to interact with many medications through various mechanisms, including raising blood alcohol levels, altering other drugs’ metabolism, interfering with medication effectiveness, or exacerbating adverse effects. Though some occur only among those who drink heavily (i.e., 3 or more drinks per occasion), many can still occur with lower alcohol consumption. Alcohol interacts with drugs in two major ways: pharmacokinetics (altering the body’s effects on the drug) and pharmacodynamics (altering the drug’s effects on the body). Effects of these interactions range from mild dizziness or drowsiness to severe or fatal consequences. Communicating to patients when to avoid alcohol and how alcohol interacts with their medication therapies is critical to ensuring safe and effective treatment of medical conditions and prevention of adverse effects.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-062-H01-P
Pharmacy Technician 0669-0000-24-063-H01-T
Credits: 1.5 contact hour(s) (0.15 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $5.99
Estimated time to complete activity: 1.5 contact hour(s) (0.15 CEU(s)), including Course Test and course evaluation
Release Date: May 26, 2024 Expiration Date: May 26, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians
How to Earn Credit: From May 26, 2024, through May 26, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives:
Upon completion of this educational activity, participants should be able to:
Describe alcohol consumption’s effects on the body
Recognize major pharmacokinetic and pharmacodynamic alcohol- drug interactions
Review best practices for discussing alcohol-drug interactions with patients
Disclosures
The following individuals were involved in developing this activity: Kelsey Giara, PharmD, RPh, and Pamela Sardo, PharmD, BS. Pamela Sardo and Kelsey Giara have no conflicts of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
A New Spin on Mixology: Mechanisms and Consequences of Drug- Alcohol Interactions
Introduction
Ethanol—the type of alcohol commonly consumed in alcoholic beverages—is widely considered a lifestyle choice rather than a drug. However, this substance has the potential to interfere with a myriad of medications used for various conditions. The effects of these interactions range from mild to severe or even fatal. Knowing which medications have the potential to affect safe medication use is critical to ensure that patients are educated on when to avoid alcohol, what effects consuming alcohol will have on the treatment of other disease states, and when to report suspected alcohol-drug interactions to a provider. Given the vast number of drug-alcohol interactions, pharmacy teams should screen patients for alcohol use regularly.
Alcohol and the Body
The dangers of excessive alcohol consumption are well understood. Whether consumed in copious amounts on a single occasion or over time, alcohol interferes with many of the body’s organs and functions, which include the following:1
Brain: hinders communication pathways, changes mood and behavior, makes it harder to think clearly, and disrupts coordination
Heart: can cause cardiomyopathy (stretching of heart muscle), arrhythmias (irregular heartbeat), high blood pressure, and stroke
Liver: leads to a variety of problems and liver inflammations, including steatosis (fatty liver), alcoholic hepatitis, fibrosis, and cirrhosis
Pancreas: causes release of toxic substances that eventually lead to pancreatitis, a dangerous inflammation of the pancreas that causes swelling and pain and impairs the organ’s ability to make enzymes and hormones for proper digestion
Immune system: weakens the immune system, making the body a much easier target for disease
When a person ingests alcohol, a small amount (about 10%) is metabolized by the stomach. The remaining alcohol is absorbed into the bloodstream via the gastrointestinal (GI) tract, primarily the stomach and upper small intestine.2 Once absorbed, alcohol transports to the liver. A portion of the alcohol is metabolized during this first trip through the liver, while the remainder leaves the liver, enters the systemic circulation, and distributes throughout the body’s tissues. The first round of metabolism through the GI tract and liver is called “first-pass metabolism.” As a person ingests more alcohol, the amount eliminated via first-pass metabolism becomes an even smaller fraction.2
The liver is the primary site of alcohol metabolism. As shown in the Figure below, several enzymes contribute to the process, but the most important are alcohol dehydrogenase (ADH) and cytochrome P450 (CYP).2
Figure
Alcohol Metabolism in the Liver
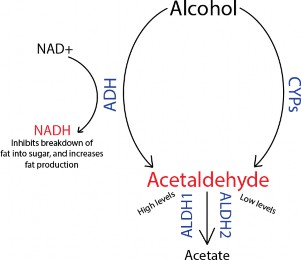

ADH, alcohol dehydrogenase; ALDH, aldehyde dehydrogenase; CYP, cytochrome P450; NAD+, nicotinamide adenine dinucleotide; NADH, reduced nicotinamide adenine dinucleotide.
Alcohol is considered a pro-drug, meaning the body breaks it down into smaller pieces (metabolites) that exert action on the body.03@ One of these metabolites is acetaldehyde. Alcohol dehydrogenase helps to break down alcohol to acetaldehyde in the liver. Acetaldehyde is a toxic substance that contributes to many of alcohol’s adverse effects. The liver removes acetaldehyde by further metabolizing it with aldehyde dehydrogenase (ALDH) to acetate.2,3 Two forms of the enzyme exist—ALDH1 and ALDH2—located in different liver cell regions. ALDH1 is only active when acetaldehyde levels are high, while ALDH2 requires only low acetaldehyde levels to become activated.2
Many liver enzymes rely on the liver’s “redox state,” which refers to the concentrations of nicotinamide adenine dinucleotide (NAD+) and reduced NAD+ (NADH).2 Alcohol metabolism via ADH also causes NAD+ to convert to NADH, thereby increasing concentrations of NADH. Elevated NADH levels stimulate fat generation and interfere with other enzymes’ ability to break down fat into sugar molecules (gluconeogenesis). These metabolic changes can greatly impact the body’s general metabolism and functioning following alcohol consumption.2 This impact increases with age as a person’s metabolism changes and slows.4
Alcohol and Medications
Alcohol interacts with drugs in two major ways: pharmacokinetics and pharmacodynamics.2 Pharmacokinetics refers to the body’s effects on a drug, including the processes of absorption, distribution, metabolism, and excretion. Pharmacodynamics refers to a drug’s effects on the body. This includes how drugs interact with the body at a molecular and cellular level, leading to the observed physiological and therapeutic effects.
The most common way that alcohol interacts with drugs through pharmacokinetics is by altering metabolism. These interactions can alter the metabolism or activity of the medication and/or alcohol metabolism, resulting in potentially serious medical consequences. Pharmacodynamic interactions, on the other hand, refer to the additive effects of alcohol and certain medications, particularly in the central nervous system (CNS).2
Pharmacokinetic Drug-Alcohol Interactions
Pharmacokinetic drug-alcohol interactions manifest mainly because medications encounter delays in their breakdown and elimination processes because they need to compete with alcohol for processing by liver enzymes, including ADH and CYP enzymes.
Drugs Affecting Alcohol Metabolism
Research suggests that some medications can block first-pass metabolism, resulting in blood alcohol levels (BALs) higher than normal for a given amount of alcohol consumption.2 Examples include drugs that can inhibit ADH activity, including aspirin and histamine H2 receptor antagonists used to treat ulcers and heartburn (e.g., cimetidine, ranitidine). Medications that accelerate gastric emptying can also reduce first-pass metabolism in the stomach, including metoclopramide, a medication used to treat nausea.2
Several medications are known to inhibit ALDH, which induces a flushing reaction upon consuming alcohol.2 One of those medications is disulfiram, a medication given to individuals with alcohol use disorder to deter drinking.2 If someone consumes alcohol while taking disulfiram, they experience a severe flushing reaction accompanied by potentially serious consequences like dilation (widening) of the blood vessels, low blood pressure, and rapid heartbeat. Other commonly used medications can also cause disulfiram-like reactions upon ingestion of even small amounts of alcohol, including second- generation cephalosporins, sulfamethoxazole-trimethoprim, isoniazid, and the antifungal metronidazole.2,5
Verapamil—a calcium channel blocker used to treat arrhythmia (irregular heartbeat), high blood pressure, and angina—is known to inhibit alcohol metabolism significantly.6 This leads alcohol to stay in the bloodstream longer than usual, causing prolonged elevated blood alcohol concentrations when individuals consume these together.
Alcohol Affecting Drug Metabolism
Alcohol can interfere with a drug’s intended medical purpose and mechanism of action. Alcohol can affect the metabolism of other drugs through two major pathways:2
Affecting CYP enzymes in the liver responsible for metabolizing other drugs
Changing the liver’s ability to eliminate various substances from the body
The CYP enzyme most commonly implicated in drug-alcohol interactions is CYP2E1, but CYP3A4 and CYP1A2 may also be involved.2 In this case, drugs must compete with alcohol for breakdown by these CYP enzymes, leading to altered drug concentrations and potential efficacy changes or adverse effects.
If individuals drink alcohol heavily over time, the body may compensate by increasing the activity of these CYP enzymes. In this case, if alcohol is no longer present to compete for these CYPs, their increased activity results in drugs being eliminated from the body much faster.2 A classic example of this phenomenon is acetaminophen, the most widely used over-the-counter analgesic. Acetaminophen is partially metabolized by CYP2E1, which forms a metabolite called N-acetyl-p-benzo-quinone imine (NAPQI), which is toxic to the liver.7 When patients take acetaminophen alone following chronic alcohol use, NAPQI formation increases, thereby increasing the risk of liver damage. Another example here is warfarin, an anticoagulant drug used to thin the blood to prevent blood clots and associated heart attack or stroke. People who chronically drink alcohol experience changes in the CYP system, causing warfarin to break down slower or faster depending upon the person’s drinking patterns.2 This leads to either dangerously high or insufficient warfarin activity, causing bleeding events or blood clots, respectively.
As discussed, when ADH breaks down alcohol into acetaldehyde, NADH levels are elevated as a byproduct. Elevated NADH can prevent the liver from generating UDP-glucuronic acid, a substance that various medications must bind to before they can be excreted from the body.2
Heavy alcohol consumption also reduces liver levels of glutathione, an antioxidant that prevents reactive oxygen species from damaging cells.2 Reduced glutathione levels increase the liver’s susceptibility to damage caused by toxic metabolites of some medications, including acetaminophen and isoniazid.
Additionally, alcohol may adversely affect the pharmacokinetics of erythromycin (a macrolide antibiotic).8 Research shows that acute alcohol consumption causes a delay in gastric emptying, resulting in delayed erythromycin absorption, lower peak concentrations, and faster elimination of the drug. It is unclear whether these pharmacokinetic changes lead to decreased erythromycin effectiveness.8 While acute alcohol intake appears not to affect doxycycline (a tetracycline antibiotic), chronic alcohol use appears to shorten the drug’s half-life, leading to subtherapeutic concentrations and decreased efficacy.8
Alcohol consumption is also shown to increase plasma levels of the beta blocker propranolol, which is used to treat hypertension and other cardiovascular conditions.6 Increased propranolol levels can exacerbate the drug’s intended and adverse effects, including dizziness, lightheadedness, fainting, and decreased heart rate.
Pharmacodynamic Drug-Alcohol Interactions
Pharmacodynamic drug-alcohol interactions do not affect drug metabolism through enzyme inhibition or activation. Instead, they involve the additive or synergistic effects of alcohol and certain drugs. Additive interactions refer to those where the combined effect of the drug and alcohol is equal to the sum of each independently. Synergistic interactions are even
more dangerous, resulting in a combined effect greater than the sum of each independently.2
Respiratory Suppression and Overdose
Concomitant alcohol use is implicated in about one in five overdose deaths every year associated with prescription opioids (22.1%) and benzodiazepines (21.4%).9 Combining alcohol with opioids or benzodiazepines (e.g., alprazolam, clonazepam, diazepam, lorazepam, temazepam) causes synergistic effects on brain circuits involved in vital physiologic functions, particularly those controlling the respiratory system.10,11
Alcohol, opioids, or benzodiazepines suppress activity in respiratory circuits in the brainstem through various receptor systems. Opioids—including prescription (e.g., codeine, fentanyl, hydrocodone, morphine, oxycodone) and illicit (e.g., heroin)—work by binding to and activating opioid receptors on nerve cells in the brain, spinal cord, and other parts of the body. Opioid receptors are a type of protein called G protein-coupled receptors. When opioids bind these receptors, they block pain signals to the brain while simultaneously causing respiratory depression.12 A study found that taking even one tablet of oxycodone with a modest amount of alcohol can increase the risk of respiratory depression, causing breathing to become extremely shallow or stop altogether.13 This risk is so significant that prescription opioid labeling includes Boxed Warnings advising against mixing them with alcohol.14
Benzodiazepines work on the inhibitory transmitter GABA to reduce overactivity in the CNS and create a calming effect for individuals with many conditions, including anxiety, seizure disorders, and insomnia, among others.15 These drugs bind to GABA receptors and alter their shape to make it easier for GABA to bind and exert its inhibitory effects. Alcohol also uses GABA receptors as a primary site of action. It modifies the membrane surrounding the GABA receptor to improve GABA’s ability to bind.15 Benzodiazepines alone carry a low risk of acute toxicity, but their toxic effects are significantly enhanced, and the risk of overdose is heightened when they are combined with alcohol.15
Combining alcohol with opioids or benzodiazepines can cause the breathing rate to become so depressed that the brain no longer receives enough oxygen. This can lead to organ failure, brain complications, coma, or death.
Additive Risks of Adverse Effects
No medication comes without the risk of adverse effects, whether benign or serious. Despite exerting action through entirely different mechanisms, in many cases, concomitant alcohol use can exacerbate a medication’s already- established adverse effects. In older adults, the risk for adverse drug reactions is exacerbated by age-related changes in alcohol and medication absorption and metabolism.4
Combining benzodiazepines with alcohol also increases the risk of other CNS-related adverse effects. For example, benzodiazepines have significant effects on individuals operating a motor vehicle, including the following:16
increased reaction times
decreased control over the vehicle’s lateral position
affected speed maintenance
impaired visual attention
increased effort in driving
Ingesting benzodiazepines and alcohol exacerbates these issues, creating detrimental effects on driving beyond those seen with either substance alone.16
Barbiturates—a medication class similar to benzodiazepines—cause similar additive adverse effects when combined with alcohol. Barbiturates are sedative or hypnotic (sleep-inducing) medications frequently used for anesthesia but also used in the community (e.g., phenobarbital for seizure disorders).2 Phenobarbital activates some of the same CNS molecules as alcohol, producing synergistic enhancements in the medication’s adverse
effects. Pharmacists should warn patients taking barbiturates not to perform tasks requiring alertness, particularly after simultaneous alcohol use.
“Z-drugs” for insomnia (e.g., eszopiclone, zaleplon, zolpidem) also produce CNS-related effects that are exacerbated by alcohol consumption.6 For example, zolpidem is known to impair motor coordination and increase fall risk, cause memory impairments, including blackouts, and promote dangerous behaviors during sleep that patients do not recall. Combining the drug with alcohol significantly increases these risks. Additionally, zolpidem overdose is most commonly associated with alcohol consumption and usually warrants intensive care in the emergency department to treat.6
Antidepressants exert their effects on the CNS to treat depression. Several antidepressant classes exist—including tricyclic antidepressants, selective serotonin reuptake inhibitors, monoamine oxidase inhibitors, and atypical antidepressants—which differ in their mechanisms of action and effects on different brain chemicals.6 These medications do share a common thread; they all have some sedative as well as some stimulating activity. Alcohol can increase antidepressant adverse effects on the CNS, including drowsiness and dizziness. It may also decrease patient response to antidepressant therapy, as well as impact treatment adherence. Monoamine oxidase inhibitors can cause a dangerous increase in blood pressure when mixed with an amino acid called tyramine, found in beer and wine, particularly red wine.6
Another CNS-associated adverse effect exacerbated by alcohol is seizure risk. Bupropion—an antidepressant and smoking cessation aid—can lower the threshold for seizures (i.e., make it easier for a seizure to be triggered in a patient’s body).6 Alcohol can lower this threshold even further, greatly increasing seizure risk in patients combining these substances.
Increased risk of bleeding is another adverse effect potentiated by alcohol. Anticoagulants (blood thinners) are especially risky with concomitant alcohol use. Both acute and long-term alcohol consumption (discussed previously) can affect the warfarin’s ability to work properly. Acute ingestion
of even a small amount of alcohol can increase the drug’s anti-clotting effects to stronger levels than necessary for medical purposes, thereby increasing the risk of significant bleeding.2 Other cardiovascular medications, like antihypertensives used to treat hypertension, can also be problematic with acute alcohol consumption. In some individuals, alcohol ingestion causes an initial drop in blood pressure, which could add to the blood pressure-lowering effects of antihypertensives.6
Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs)— including aspirin, ibuprofen, and naproxen—are associated with an increased risk of GI bleeding due to their effects on the lining of the GI tract.6 Combining these medications with alcohol increases this risk, as alcohol induces damage to the mucosa of the GI lining and can also cause GI bleeds alone.17 About one in five people hospitalized for GI bleeds is a heavy alcohol drinker, but studies show that consuming even a modest amount of alcohol is risky; one drink per day increases the risk of GI bleeding associated with NSAID use by about 37%.16,17
Liver toxicity is another concern associated with alcohol-drug combinations, given alcohol’s metabolism in the liver and the substance’s propensity to cause liver damage. Many medications are known to cause liver toxicity, so individuals should avoid concomitant alcohol use to prevent the additive potential for this effect. Examples include some antimicrobials— ketoconazole, griseofulvin, isoniazid, and rifampin, among others—and duloxetine, an antidepressant.6
Increased risk of accidents and injuries are also a concern with alcohol- drug combinations. Antihistamines used for allergies and cold symptoms, for example, can cause adverse effects like drowsiness, sedation, and low blood pressure.2 Older individuals are especially prone to experiencing these effects. Alcohol can substantially enhance the sedating effects of antihistamines, which increases the risk of falling. This can lead to significant injuries, especially in older adults.
Practice Pointer: A medication’s prescribing label should note whether and how alcohol affects its safety and effectiveness. This information can be found on the DailyMed website, the NIH’s National Library of Medicine, or Drugs@FDA.
Engaging the Pharmacy Team
Given the vast number of drug-alcohol interactions noted, it is crucial to screen patients for alcohol use regularly. Reframing alcohol as a drug and using non-stigmatizing language are critical to this process. Pharmacists and pharmacy technicians must be prepared to identify potential drug-alcohol interactions in all practice settings and be confident intervening respectfully.
Reframing Alcohol as a Drug
Alcohol use often feels like a difficult topic to broach with patients, creating a blind spot in patient care. Individuals often misperceive alcohol as a benign or inert substance with no pharmacologic effects. Others observe alcohol use as a lifestyle choice rather than considering its ability to affect medical status or health. Reframing the conversation is important to shift the conversation from an “alcohol problem” to “problems caused by alcohol.” Pharmacists are often quick to educate rather than discuss, which can come across as contentious or paternalistic. It is important to integrate alcohol into the medication review instead as another drug directly linked to the patient’s health conditions and other medications rather than a separate “healthy living” issue.
Eliminating Stigma from the Conversation
Using non-stigmatizing language when discussing alcohol use is crucial as it helps reduce shame and encourages individuals to be forthcoming without fear of judgment.18 Using respectful and non-judgmental language like those in the Table below fosters a more supportive and understanding
environment and helps encourage patients to consider alcohol as a drug, rather than a lifestyle choice.
Table
Non-Stigmatizing Language for Discussing Alcohol Use18
| DON’T Say | DO Say |
Substance abuser Alcoholic Addict User/abuser Drunk | A person with a substance use disorder |
| Abuse Problem | Use/misuse Risky, unhealthy, or heavy use |
| Clean | Person in recovery Abstinent Not drinking |
Identifying Potential Sources of Alcohol
Just as it is important to address intentional alcohol consumption, some alcohol sources may be unintentional. For example, many prescription and over-the-counter drugs contain alcohol. Pharmacists and pharmacy technicians can help patients identify products containing alcohol that may interact with their prescription medications, including many liquid medications to treat cough and cold symptoms, mouthwash, and other oral health preparations.
Nonaqueous solutions, typically available by prescription only, also contain alcohol:19
Elixirs: clear, sweetened, hydroalcoholic liquids intended for oral use (5% to 40% alcohol)
Spirits or essences: alcoholic or hydroalcoholic solutions of volatile substances (usually volatile oils) commonly used as flavoring agents (62% to 85% alcohol)
Tinctures: alcoholic or hydroalcoholic solutions prepared from vegetable or chemical substances (up to 50% alcohol)
Preservatives: pharmaceutical products must contain at least 15% alcohol to preserve the product from microbial growth if no other preservative agents are present
Summary
Alcohol interacts with drugs through pharmacokinetics and pharmacodynamics. Pharmacokinetically, drug-alcohol interactions can alter the metabolism or activity of the medication and/or alcohol metabolism. Pharmacodynamic interactions, on the other hand, refer to the additive effects of alcohol and certain medications, particularly in the CNS. Concomitant alcohol use can also exacerbate a medication’s already-established adverse effects and interfere with a drug’s intended mechanism of action.
When in doubt, pharmacy teams should consult reliable interaction checkers to identify potential alcohol-drug interactions. The medication's prescribing label should note whether and how alcohol affects its safety and effectiveness. The label can be found on the DailyMed website, the NIH’s National Library of Medicine, or from Drugs@FDA.
Course Test
Where is the primary site of alcohol metabolism?
Central nervous system
Liver
Kidneys
Pancreas
Which of the following is a toxic metabolite of alcohol?
Acetaldehyde
NAPQI
NAD+
Acetate
Which of the following occurs in the body following alcohol consumption?
Increased generation of sugar
Increased breakdown of sugar into fat
Increased breakdown of fat into sugar
Increased basal metabolic rate
Which of the following drugs can produce a flushing reaction when combined with alcohol?
Metronidazole
Acetaminophen
Clonazepam
Ketoconazole
Which of the following BEST describes the risk associated with combining alcohol and opioids?
Severe gastrointestinal bleeding
Dangerously elevated heart rate
Reduced glutathione levels in the liver
Potentially fatal respiratory depression
Which of the following is an expected adverse effect of combining verapamil and alcohol?
Increased blood pressure
Elevated blood alcohol concentrations
Severe flushing and vasodilation
Potentially fatal pancreatitis
Which of the following is expected following acute alcohol consumption for a patient taking warfarin?
Increased risk of bleeding
Increased risk of stroke
Increased risk of liver toxicity
Nothing, only chronic alcohol use affects warfarin
Which of the following is TRUE about combining NSAIDs with alcohol?
It is safer than combining alcohol with acetaminophen
It can cause acute liver toxicity
It increases blood alcohol concentrations
It increases the risk of gastrointestinal bleeding
Which of the following happens when pharmacy teams consider alcohol as another drug rather than a lifestyle choice?
Patients feel stigmatized and judged
Patients consider alcohol safer and consume it more often
Patients are more likely to consider its effects on health
Patients think pharmacists are know-it-alls
Which of the following is an appropriate phrase for discussing alcohol consumption with patients?
Alcohol abuse
Alcohol use
Alcoholic
Alcohol problem
References
National Institute on Alcohol Abuse and Alcoholism. Alcohol's Effects on Health: Research-based information on drinking and its impact. https://www.niaaa.nih.gov/alcohols-effects-health/alcohols-effects- body. Accessed May 23, 2024.
Weathermon R, Crabb DW. Alcohol and medication interactions. Alcohol Res Health. 1999;23(1):40-54.
Deehan GA Jr, Brodie MS, Rodd ZA. What is in that drink: the biological actions of ethanol, acetaldehyde, and salsolinol. Curr Top Behav Neurosci. 2013;13:163-184. doi:10.1007/7854_2011_198
Zanjani F, Allen H, Schoenberg N, Martin C, Clayton R. Acceptability of intervention materials to decrease risk for alcohol and medication interactions among older adults. Eval Program Plann. 2018;67:160-166. doi:10.1016/j.evalprogplan.2017.12.010
Noureldin M, Krause J, Jin L, Ng V, Tran M. Drug-Alcohol Interactions: A Review of Three Therapeutic Classes. US Pharm. 2010;35(11):29-
40. https://www.uspharmacist.com/article/drug-alcohol-interactions-a-
review-of-three-therapeutic-classes. Accessed May 23, 2024.
National Institute on Alcohol Abuse and Alcoholism. Alcohol-Medication Interactions: Potentially Dangerous Mixes. May 6, 2022. https://www.niaaa.nih.gov/health-professionals-communities/core- resource-on-alcohol/alcohol-medication-interactions-potentially- dangerous-mixes. Accessed May 23, 2024.
Rumack B, Heard K, Green J, et al. Effect of therapeutic doses of acetaminophen (up to 4 g/day) on serum alanine aminotransferase levels in subjects consuming ethanol: systematic review and meta- analysis of randomized controlled trials. Pharmacotherapy. 2012;32(9):784-791. doi:10.1002/j.1875-9114.2012.01122.x
Mergenhagen KA, Wattengel BA, Skelly MK, Clark CM, Russo TA. Fact versus Fiction: a Review of the Evidence behind Alcohol and Antibiotic Interactions. Antimicrob Agents Chemother. 2020;64(3):e02167-19. Published 2020 Feb 21. doi:10.1128/AAC.02167-19
Jones CM, Paulozzi LJ, Mack KA; Centers for Disease Control and Prevention (CDC). Alcohol involvement in opioid pain reliever and benzodiazepine drug abuse-related emergency department visits and drug-related deaths - United States, 2010. MMWR Morb Mortal Wkly Rep. 2014;63(40):881-885.
Boon M, Dorp E van, Broens S, Overdyk F. Combining opioids and benzodiazepines: effects on mortality and severe adverse respiratory events. Ann Palliat Med. 2020;9(2):54257-54557. doi:10.21037/apm.2019.12.09
van der Schrier R, Roozekrans M, Olofsen E, et al. Influence of Ethanol on Oxycodone-induced Respiratory Depression. Anesthesiology. 2017;126(3):534-542. doi:10.1097/ALN.0000000000001505
Corder G, Castro DC, Bruchas MR, Scherrer G. Endogenous and Exogenous Opioids in Pain. Annu Rev Neurosci. 2018;41:453-473. doi:10.1146/annurev-neuro-080317-061522
van der Schrier R, Roozekrans M, Olofsen E, et al. Influence of Ethanol on Oxycodone-induced Respiratory Depression: A Dose-escalating Study in Young and Elderly Individuals. Anesthesiology. 2017;126(3):534-542. doi:10.1097/ALN.0000000000001505
U.S. Food and Drug Administration. FDA warns about serious risks and death when combining opioid pain or cough medicines with benzodiazepines; requires its strongest warning. August 31, 2016. https://www.fda.gov/media/99761/download. Accessed May 23, 2024.
Longo LP, Johnson B. Addiction: Part I. Benzodiazepines--side effects, abuse risk and alternatives. Am Fam Physician. 2000;61(7):2121-2128.
Maxwell HG, Dubois S, Weaver B, Bédard M. The additive effects of alcohol and benzodiazepines on driving. Can J Public Health. 2010;101(5):353-357. doi:10.1007/BF03404852
National Institute on Alcohol Abuse and Alcoholism. Medical Complications: Common Alcohol-Related Concerns. May 6, 2022. https://www.niaaa.nih.gov/health-professionals-communities/core- resource-on-alcohol/medical-complications-common-alcohol-related- concerns. Accessed May 23, 2024.
Boston Medical Center. Reducing stigma: Why words about addiction matter. https://www.bmc.org/addiction/reducing-stigma. Accessed May 23, 2024.
UNC Eshelman School of Pharmacy: The Pharmaceutics and Pharmaceutical Compounding Laboratory. Pharmaceutical Solutions II: Nonaqueous Solutions. https://pharmlabs.unc.edu/labexercises/compounding/pharmsol2/. Accessed May 23, 2024.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace
those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.