BREAST CANCER TREATMENT: A MULTIDISCIPLINARY APPROACH
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson, MD, FACP, is an Associate Professor of Internal Medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Liz Fredrickson, PharmD, BCPS
Liz Fredrickson is an Associate Professor of Pharmacy Practice and Pharmaceutical Sciences at the Northeast Ohio Medical University (NEOMED) College of Pharmacy.
Topic Overview
Breast cancer remains one of the most prevalent cancers affecting women worldwide, necessitating a thorough understanding of its epidemiology, risk factors, and management strategies. Healthcare professionals must have essential knowledge of breast cancer care, including the latest treatment strategies and the importance of interdisciplinary management. Within this activity, learners will gain insight into key epidemiological data and risk factors associated with breast cancer, enabling them to identify high-risk individuals and implement preventive measures effectively. The presentation will also cover the various screening and diagnostic tools available for early detection and accurate breast cancer diagnosis. Evidence-based treatment strategies will also be described, as will the roles of interdisciplinary team members.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-147-H01-P
Pharmacy Technician 0669-0000-24-148-H01-T
Credits: 2 contact hour(s) (0.2 CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $6.99
Estimated time to complete activity: 2 contact hour(s) (0.2 CEU(s)), including Course Test and course evaluation
Release Date: October 14, 2024 Expiration Date: October 14, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
How to Earn Credit: From October 14, 2024, through October 14, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Identify key epidemiological data and risk factors associated with breast cancer
Evaluate the various screening and diagnostic tools available for early detection and diagnosis of breast cancer
Describe evidence-based strategies for the treatment of breast cancer
Describe the roles of members of the interdisciplinary team in the management of breast cancer
Disclosures
The following individuals were involved in developing this activity: L. Austin Fredrickson, MD, FACP, Liz Fredrickson, PharmD, BCPS, and Pamela Sardo, PharmD, BS. Pamela Sardo, L. Austin Fredrickson, MD, FACP, and Liz Fredrickson, PharmD, BCPS, have no conflicts of interest or financial relationships regarding the subject matter. There are no financial relationships or commercial or financial support relevant to this activity to report or disclose by RxCe.com or any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Breast Cancer Treatment: A Multidisciplinary Approach Introduction
Breast cancer is a major cause of cancer deaths in women. Patients with breast cancer face numerous challenges, and the management of this disease requires a comprehensive understanding of important risk factors, screening recommendations, treatment modalities, and an interdisciplinary approach to care. As advancements in breast cancer care continue to evolve, healthcare professionals must stay informed about the latest diagnostic and treatment guidelines and the roles of various team members to optimize patient outcomes.
Within this continuing education activity, learners will gain insight into key epidemiological data and risk factors associated with breast cancer, enabling them to identify high-risk individuals and implement preventive measures effectively. This course will cover the various screening and diagnostic tools available for early detection and accurate breast cancer diagnosis. Evidence-based treatment strategies will also be described, as will the roles of interdisciplinary team members.
Etiology and Epidemiology
Breast cancer is the most diagnosed cancer in women worldwide. 1 In 2023, 43,700 women died from breast cancer. 1,2 This is second only to lung cancer deaths.1,2 Breast cancer is a heterogeneous disease influenced by an array of genetic, hormonal, and environmental factors.3
Breast cancer continues to persist as a significant health challenge.1 The lifetime risk for a woman developing breast cancer is approximately one in eight, and incidence rates vary significantly by region.2 Rates are higher in developed countries in part due to differences in reproductive behaviors, lifestyle factors, and the availability of screening programs.1,2,4
The incidence of breast cancer increases with age, particularly after the age of 50, with a median age of diagnosis at 62 years of age.2,3 The incidence of breast cancer has increased at a rate of ~0.3% per year since 2004.2 In 2023, a staggering 300,000 new cases and more than 43,000 deaths due to invasive breast cancer were estimated to have occurred.1
Geographical and racial disparities impact both the incidence of breast cancer incidence and its outcomes.2 For instance, between 2012 and 2016, the annual age-adjusted incidence rate was 130.8 cases per 100,000 for non- Hispanic White women, 126.7 cases for non-Hispanic Black women, and 93.7 cases for Hispanic women.2 Despite a lower incidence, non-Hispanic Black women have higher mortality rates, often attributed to factors such as stage at diagnosis, access to care, comorbidities, and treatments.2
The etiology of breast cancer involves numerous risk factors, including both modifiable and non-modifiable factors.3,4 Non-modifiable factors include age, gender, family history, and germline mutations, particularly in the BRCA1 and BRCA2 genes, which significantly increase the risk of developing breast cancer–as well as ovarian cancer.2 Women with these mutations have a 70% probability of developing BC by age 80.2 Mutations in other genes, such as TP53, PTEN, and CHEK2, also contribute to breast cancer risk but to a lesser extent.2
Modifiable risk factors include lifestyle-related factors such as obesity, physical inactivity, and alcohol consumption.2 Hormonal factors, including early menarche (before age 11), late menopause (at 55 years of age or later), and nulliparity, also play a significant role in increasing breast cancer risk.2,4
Risk factors are presented in Table 1 below, and lifestyle impacts are expounded on in Table 2.2,4
Table 1
Risk Factors for the Development of Breast Cancer2,4
| Non-Modifiable Factors | Modifiable Factors |
| Female sex | Hormonal replacement therapy |
| Older age | Diethylstilbestrol |
| Family history (of breast or ovarian cancer) | Physical activity |
| Genetic mutations | Overweight/obesity |
| Race/ethnicity | Alcohol intake |
| Pregnancy and breastfeeding | Smoking |
| Menstrual period and menopause | Insufficient vitamin supplementation |
| Density of breast tissue | Excessive exposure to artificial light |
| Previous history of breast cancer | Intake of processed food |
| Non-cancerous breast diseases | Exposure to chemicals |
| Previous radiation therapy | Other drugs |
Table 2
Environmental and Lifestyle Impacts on Breast Cancer Development2
| Factor | Comments |
| Elevated Risk | |
Alcohol consumption | Consumption before the first pregnancy may affect the risk 20% higher risk for women who have 2-3 alcoholic drinks per day compared to non-drinkers |
Tobacco | Slightly increased risk (in long-term) Heavy smokers who started smoking before their first pregnancy |
| Radiation exposure | Especially if exposure was before 10-30 years of age |
| Factor | Comments |
| Reduced Risk | |
| Diet: Fruit and vegetable intake |
May decrease risk, but there is limited evidence |
| Physical activity | Has a protective effect independent of a patient’s BMI |
| No Association | |
| Diet: Fat intake | No association based on recent data |
| Mixed Data | |
| Diet: Soy | Reduced risk in Asian women |
| Excess body weight/weig ht gain | Reduced risk in premenopausal women Elevated risk in postmenopausal women |
Preventive measures are critical in managing breast cancer risk. The National Cancer Institute's (NCI) Breast Cancer Risk Assessment Tool provides an estimate of a woman's risk of developing breast cancer within the next five years, assisting healthcare providers in identifying high-risk individuals and implementing appropriate preventive strategies.2,5 Notably, this calculator has not been validated for patients with a history of invasive breast cancer or those with genetic factors.2,5
Screening and Detection
The early detection of breast cancer significantly improves survival rates, making screening an essential component of breast cancer management (Table 3).2,6,7 Risk-reducing strategies should be implemented to both identify and minimize the risk of developing breast cancer.2 Mammography remains the gold standard for breast cancer screening, capable
of detecting tumors at an early stage when they are most treatable.2,6 The
U.S. Preventive Services Task Force (USPSTF) recommends biennial screening mammography for women aged 40 to 74 years, noting a moderate net benefit.7 They note recommendations do not apply to patients with genetic markers including BRCA1 or BRCA2 with a high risk of breast cancer.7 Still, they offer a separate recommendation on risk assessment and genetic counseling for these individuals.7 Per the USPSTF, more research is needed to determine screening harms and benefits for women 75 years of age and older and to determine ways to reduce the risk of overdiagnosing and, therefore, overtreating breast lesions found through screenings.7
Table 3
USPSTF Screening Recommendations7
| Population | Recommendation |
Women aged 40 to 74 years | The USPSTF recommends biennial screening mammography for women aged 40 to 74 years. |
| Women 75 years or older | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening mammography in women 75 years or older. |
| Women with dense breasts | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of supplemental screening for breast cancer using breast ultrasonography or magnetic resonance imaging (MRI) in women identified to have dense breasts on an otherwise negative screening mammogram. See the "Practice Considerations" section for more information on the patient population to whom this recommendation applies and on screening mammography modalities. |
The American Cancer Society (ACS) recommends women at average risk aged 40 to 44 may opt to begin annual mammograms.6 Women aged 45 to 54 are advised to undergo mammograms every year.6 Starting at age 55, the ACS suggests women can either continue with yearly mammograms or switch
to screening every other year, depending on their health status and life expectancy of at least ten more years.6 They note all women need to understand the benefits and limitations of mammograms in breast cancer detection. Additionally, clinical breast exams are not recommended for breast cancer screening in average-risk women at any age.6
Different specialty societies have varied recommendations on initiation and intervals of screenings, which are updated individually and can cause discrepancy and controversy. Beyond mammography, other screening methods may include digital mammography, digital breast tomosynthesis (tomosynthesis or three-dimensional mammography), ultrasonography, and magnetic resonance imaging (MRI), though recommendations for these methods vary.2
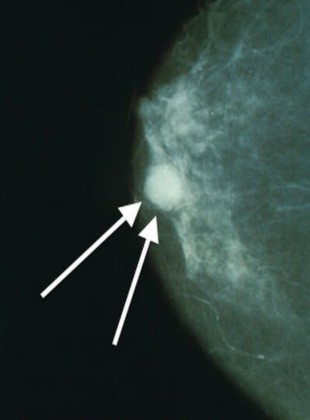
Breast cancer imaging examples are provided in Figures 1 and 2 below.
Figure 18
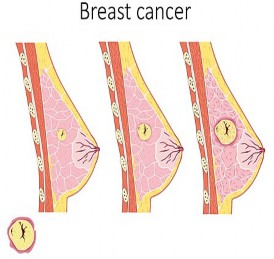
Figure 29
Care Team Timeout
Primary care providers (PCPs) and pharmacists should be familiar with breast cancer risk factors because early identification and intervention can significantly impact patient outcomes.
During wellness or acute visits, PCPs are crucial in assessing a patient’s risk factors, conducting screenings, and guiding patients on preventive measures. They are often a patient’s first point of contact and can initiate referrals to specialists when necessary.
Pharmacists in both community and institutional settings are accessible healthcare professionals who can educate patients about risk factors, encourage adherence to screening recommendations, and support managing medications that may be used for prevention or treatment.
Together, PCPs and pharmacists ensure a comprehensive approach to breast cancer prevention and care, enhancing patient awareness and facilitating timely interventions.
Clinical Presentation and Diagnosis
Breast cancer can present with a variety of clinical manifestations, depending on the stage and subtype of the disease. Patients are often asymptomatic, and breast cancer is commonly detected through routine mammography screening.2 When symptoms occur, the most common is a painless, palpable lump.2 Less commonly, patients may experience pain, nipple discharge, retraction or dimpling, and skin changes such as edema, redness, or warmth.2 In more advanced stages, breast cancer may present with symptoms related to metastasis, such as bone pain, shortness of breath, jaundice, or neurological symptoms, depending on the site of metastatic spread.2 Approximately 20-30% of women with early-stage breast cancer will eventually develop metastatic breast cancer.2 Accurate and early diagnosis of breast cancer is essential for effective treatment and improved survival outcomes.
The diagnostic approach may involve a combination of a patient’s history, physical examination, imaging, biopsy, and molecular testing.2 Biopsies are vital for confirming a breast cancer diagnosis. Depending on the clinical scenario, it can be performed using fine-needle aspiration, core needle biopsy, or excisional biopsy.2
Molecular testing of biopsy samples is crucial for determining hormone receptor status, which guides treatment decisions.2 Hormone receptor status includes estrogen receptor and progesterone receptor (ER/PR), as well as HER2 expression. Genetic testing for BRCA mutations and other hereditary cancer syndromes may also be indicated in patients with a strong family history or early-onset breast cancer.2 Diagnostic approaches are summarized in Table 4 below.2
Table 4
Diagnostic Approaches for Breast Cancer Detection2,10
| Diagnostic Tool | Description |
| Mammography | Gold standard for breast cancer screening, capable of detecting tumors at an early stage |
| Ultrasound | Noninvasive Auxiliary tool Guide for biopsy |
| Magnetic Resonance Imaging (MRI) | Assess for the breast symmetry and the possible changes in the parenchymal tissue; changes might indicate the presence of lesions that can be malignant |
| Biopsy | A definitive diagnosis is made through a biopsy, which can be performed via fine-needle aspiration, core needle biopsy, or excisional biopsy |
| Molecular Testing | Hormone receptor status (ER/PR) and HER2 expression are assessed to guide treatment decisions Genetic testing for BRCA mutations may be indicated in patients with a strong family history |
In terms of laboratory findings in patients with metastatic breast cancer, tumor markers such as cancer antigen 15-3 (CA 15-3) and carcinoembryonic antigen (CEA) may be elevated.2 Additionally, elevated levels of alkaline phosphatase or abnormal liver function test results can also indicate the presence of metastatic disease.2
Care Team Timeout
PCPs should be knowledgeable regarding factors that may affect the accuracy of mammography, such as breast density, which can vary with age, menopausal status, and hormone replacement therapy use
For women with dense breasts or specific conditions, alternative imaging methods like ultrasonography, MRI, digital mammography, and tomosynthesis may be considered
Once a diagnosis is confirmed, the PCP collaborates with oncologists, surgeons, and other specialists to develop a comprehensive treatment plan
PCPS need to discuss expectations with patients and approach care plan development in a patient-centric manner
While pharmacists are unable to diagnose breast cancer, they can refer patients in need of screening or with alarm symptoms to their PCPs
Breast Cancer Staging and Prognosis
Breast cancer confined to a localized breast lesion is often referred to as early, primary, localized, or curable.2 When the cancer spreads to local– regional lymph nodes, it is still considered an early stage.2 However, breast cancer cells can spread through lymph channels or the bloodstream to distant sites, leading to advanced or metastatic breast cancer.2 Common sites for distant metastases include lymph nodes beyond the local–regional area, skin, bone, liver, lungs, and brain.2 Symptoms such as bone pain, difficulty breathing, abdominal enlargement, jaundice, and mental status changes may indicate the presence of metastatic breast cancer.2 Some women may present with distant metastases at their initial appointment, often due to a neglected breast mass.2 Additionally, 20% to 30% of patients with early-stage breast cancer will eventually develop metastatic disease.2 The staging of breast cancer is summarized in Table 5.2
Table 5
Breast Cancer Staging2
| TX | Primary tumor cannot be assessed | |||||
| T0 | No evidence of primary tumor | |||||
| Tis (DCIS) | Ductal carcinoma in situ | |||||
| Tis (Paget) | Paget’s disease of the nipple carcinoma or carcinoma in situ | NOT | associated | with | invasive | |
| T1 | Tumor ≤2 cm in greatest dimension | |||||
| T1mi | <0.1 cm; microinvasion | |||||
| T1a | >0.1 cm ≤0.5 cm | |||||
| T1b | >0.5 cm ≤1 cm | |||||
| T1c | >1 cm ≤2 cm | |||||
| T2 | Tumor >2 cm ≤5 cm | |||||
| T3 | Tumor >5 | cm | ||||
| T4 | Tumor of any size with direct extension to the chest wall and/or to the skin | |||||
| T4a | Extension to the chest wall; invasion or adherence to pectoralis muscle in the absence of invasion of chest wall structures | |||||
| T4b | Ulceration and/or ipsilateral macroscopic satellite nodules and/or edema (including peau d’orange) of the skin that does not meet the criteria of inflammatory carcinoma | |
| T4c | Both T4a and T4b present | |
| T4d | Inflammatory carcinoma | |
| Regional Lymph Nodes: Clinical (cN) | ||
| cNX | Regional lymph nodes cannot be assessed | |
| cN0 | No regional lymph node metastases | |
| cN1 | Metastases to movable ipsilateral level 1, II axillary lymph node(s) | |
| cN1mi | Micrometastases (approximately 200 cells, >0.02 cm <0.2 cm) | |
| cN2 | Metastases in ipsilateral level I, II axillary lymph nodes that are clinically fixed or matted; or in ipsilateral internal mammary nodes in the absence of axillary lymph node metastases | |
| cN2a | Metastases in ipsilateral level I, II axillary lymph nodes fixed to one another (matted) or to other structures | |
| cN2b | Metastases only in ipsilateral internal mammary nodes in the absence of axillary lymph node metastases | |
| cN3 | Metastases in ipsilateral infraclavicular (level III axillary) lymph node(s) with or without level I, II axillary lymph node involvement; or in ipsilateral internal mammary lymph node(s) with level I, II axillary lymph node metastases; or metastases in ipsilateral supraclavicular lymph node(s) with or without axillary or internal mammary lymph node involvement | |
| cN3a | Metastases in ipsilateral infraclavicular lymph node(s) | |
| cN3b | Metastases in ipsilateral internal mammary lymph node(s) and axillary lymph node(s) | |
| cN3c | Metastases in ipsilateral supraclavicular lymph node(s) | |
| Regional Lymph Nodes: Pathologic (pN) | ||
| pNX | Regional lymph nodes cannot be assessed | |
| pN0 | No regional lymph node metastasis identified or Isolated tumor cells (ITCs) only | |
| pN0(i+) | ITCs only, no larger than 0.02 cm in regional lymph nodes | |
| pN0(mo l+) | Positive molecular findings by reverse transcriptase polymerase chain reaction; no ITCs detected | |
| pN1 | Micrometastases; or metastases in 1-3 axillary lymph nodes; and/or clinically negative internal mammary nodes with micrometastases or macrometastases by sentinel lymph node biopsy | |
| pN1mi | Micrometastases, (approximately 200 cells, >0.02 cm <0.2 cm) | |
| pN1a | Metastases in ipsilateral internal mammary sentinel nodes, excluding ITCs | |
| pN1c | pN1a and pN1b combined | |
| pN2 | Metastases in 4-9 axillary lymph nodes; or positive ipsilateral internal mammary lymph nodes by imaging in the absence of axillary lymph node metastases | |
| pN2a | Metastases in 4-9 lymph nodes (at least one deposit >0.2 cm) | |
| pN2b | Metastases in clinically detected internal mammary lymph nodes with or without microscopic confirmation; with pathologically negative axillary nodes | |
| pN3 | Metastases ≥10 or more axillary lymph nodes; or in infraclavicular (level III axillary) lymph nodes; or positive ipsilateral internal mammary lymph nodes by imaging in the presence ≥1 positive level I, II axillary lymph nodes; or in >3 axillary lymph nodes and micrometastases or macrometastases by sentinel lymph node biopsy in clinically negative ipsilateral internal mammary lymph nodes; or in ipsilateral mammary lymph nodes | |
| pN3a | Metastases in ≥10 axillary lymph nodes (at least one tumor deposit >0.2 cm) or metastases to infraclavicular (level III axillary lymph) nodes | |
| pN3b | pN1a or pN2a in the presence of cN2b (positive internal mammary nodes by imaging) or pN2a in presence of pN1b | |
| pN3c | Metastases in ipsilateral supraclavicular lymph nodes | |
| Distant Metastasis (M) | ||
| M0 | No clinical or radiographic evidence of distant metastases | |
| cM0(i+) | No clinical or radiographic evidence of distant metastases in the presence of tumor cells or deposits <0.02 cm detected microscopically or by molecular techniques in circulating blood, bone marrow, or other nonregional nodal tissue in a patient without symptoms or signs of metastases | |
| cM1 | Distant metastases detected by clinical and radiographic means | |
How breast cancer progresses is incredibly patient-specific. Some patients may experience a rapidly advancing and aggressive form of the disease, while others have a slower course.2 In determining strategic, personalized treatment plans for patients, clinicians need to be able to predict prognoses accurately.2 Prognostic factors are characteristics or measurements that become available at diagnosis or during surgery and are associated with outcomes like recurrence or survival rates independent of any additional systemic therapy.2 Predictive factors, on the other hand, help determine the likelihood of a patient’s response to specific treatments.2 These factors encompass a range of categories, including patient characteristics such as age, cancer-specific features like tumor size and histologic type, biomarkers such as hormone-receptor status, and genetic variables.2
Prognostic and predictive factors for breast cancer outcomes include both patient and cancer characteristics as well as biomarkers.2 Younger age (under 35) and African American race are associated with a worse prognosis. Key cancer characteristics influencing prognosis are tumor size, lymph node involvement, lymphovascular invasion, nuclear grade (with grade 3 being the most aggressive), and histologic subtype, particularly invasive ductal carcinoma.2 Biomarkers also play a significant role, with estrogen and progesterone receptor positivity (ER/PR) being favorable, while HER2 positivity is generally associated with a poorer prognosis.2
Treatment Modalities
The treatment of breast cancer is multidisciplinary and may involve surgery, radiation therapy, systemic therapy, and supportive care. The treatment approach depends on the disease stage and patient factors, including age, comorbidities, and preferences. The goal of treatment varies by stage: in early-stage breast cancer, the primary objective is curative, while in
Any histologically proven metastases in distant organs; or if in nonregional nodes, metastases >0.02 cm
pM1
advanced metastatic breast cancer, the focus may shift toward palliation and quality of life. Early-stage or curative breast cancer often involves the use of various treatment strategies, including surgery, radiation, and systemic medication therapies.2
Care Team Timeout
Once a diagnosis is made, PCPs continue to be involved in coordinating care, managing comorbid conditions, and addressing the overall health of the patient
They provide essential support in monitoring treatment side effects, managing chronic conditions, and ensuring patients adhere to prescribed therapies
Throughout treatment, PCPs remain key advocates for the patient, ensuring continuity of care and addressing the full spectrum of their health needs
In working with the care team to select and monitor treatments,
pharmacists can medications, and
review
the patient's comorbidities, current
treatment history to identify potential drug
interactions and the need for dose adjustments
Pharmacists can assess a patient's readiness to follow the treatment plan and manage any side effects or complications from prior therapies
The management of metastatic breast cancer promotes disease regression and optimizes a patient’s quality of life.2 The approach is personalized based on a tumor’s characteristics, prior treatments, and the patient's overall health and preferences.2
Surgery
The management of early invasive breast cancer treatment may include breast-conserving surgery (BCS) followed by radiotherapy (RT) and mastectomy with or without reconstruction.1 BCS involves removing part of the breast with cancer and surrounding margins, while mastectomy involves the removal of the entire breast.11 BCS combined with RT offers similar local
recurrence rates (LRR) and survival outcomes compared to mastectomy, particularly for estrogen receptor (ER) positive and HER2-positive breast cancers.1 It is often preferred due to better cosmetic and patient satisfaction outcomes.1 BCS may not be appropriate for patients with extensive micro- calcifications or those unable to achieve negative margins.1 Neoadjuvant chemotherapy (NAC) may be used to shrink the tumor and facilitate BCS for patients with large tumors.1 The management of axillary lymph nodes varies based on the initial status and the use of neoadjuvant therapy, with sentinel lymph node (SLN) biopsy often sufficient for clinically node-negative patients.1 Surgery is also crucial in managing local-regional recurrences, with mastectomy or wide resection being standard, depending on previous treatments.1
Chemotherapy
The use of chemotherapy in breast cancer includes neoadjuvant (NAC), adjuvant (AC), and salvage therapies, which may significantly reduce the risk of recurrence.1 NAC is given before surgery to shrink a tumor’s size and increase the effectiveness of the surgery.1 AC is given after surgery to kill the remaining cancer cells and prevent the recurrence of the cancer.1 Salvage therapy is used once other treatments have failed.1 NAC is particularly beneficial for downstaging tumors, making them operable, or facilitating breast conservation surgery.1 It is recommended for large tumors, multiple lymph node involvement, and aggressive subtypes like triple-negative and HER2-positive cancers.1 NAC allows for the assessment of treatment response and guides subsequent therapies.1
In the treatment of early-stage cancer, chemotherapy regimens can be anthracycline-based or non-anthracycline-based.1 The anthracycline-based regimen typically involves doxorubicin and cyclophosphamide administered every 2-3 weeks for four cycles, followed by a taxane, such as weekly paclitaxel for 12 weeks or docetaxel every three weeks for four cycles.1 The non-anthracycline option includes docetaxel and cyclophosphamide every three weeks for four cycles.1
Adjuvant chemotherapy is typically administered within three months post-surgery, with dose-dense regimens (every 14 days) showing better outcomes than traditional schedules.1 Emerging evidence supports specific regimens, such as adding platinum for triple-negative breast cancer or using capecitabine maintenance therapy for improved survival.1
Radiotherapy
Radiotherapy (RT) remains a cornerstone of treatment after breast- conserving surgery (BCS), particularly with whole breast irradiation (WBI) or hypofractionated WBI for early-stage breast cancer.1 For selected low-risk patients, partial breast irradiation (PBI) or accelerated PBI may be viable alternatives, offering similar outcomes with reduced toxicity.1 Postmastectomy RT (PMRT) is standard for patients with four or more positive axillary lymph nodes, although its benefit in those with one to three nodes is still under study.1 Regional nodal irradiation, including the chest wall and supraclavicular areas, improves disease-free survival, especially involving internal mammary nodes (IMNs).1 However, the latter remains controversial due to potential increased toxicity.1
Endocrine Therapy
Endocrine therapy is a standard adjuvant treatment for hormone receptor-positive (HR+) breast cancer, and the duration of endocrine therapy is typically 5 to 10 years.1 In premenopausal women, tamoxifen 20 mg per day is commonly used, with extended treatment of up to 10 years showing further reductions in recurrence and mortality.1 For high-risk patients, combining ovarian suppression with an aromatase inhibitor (AI) and tamoxifen improves outcomes, though with higher toxicity.1 In postmenopausal women, AIs are often preferred due to better efficacy, particularly in high-risk cases, though they are associated with higher bone-related side effects.1 The duration and combination of endocrine therapies may be guided by multigene assays, particularly in endocrine-resistant cases, where CDK inhibitors may be added for better outcomes.1
Targeted Therapy
Targeted therapy, particularly for HER2-positive breast cancer, has revolutionized treatment, with trastuzumab (an anti-HER2 drug) being the cornerstone.1 Combining trastuzumab with chemotherapy significantly reduces recurrences and improves survival, making it a standard in neoadjuvant and adjuvant settings.1 Additional anti-HER2 agents like pertuzumab and lapatinib have shown benefits in increasing pathological complete response (pCR) rates and improving outcomes in HER2-positive cancers.1 Early use of anti-HER2 therapies such as docetaxel with trastuzumab and pertuzumab is recommended for metastatic disease, with newer agents like trastuzumab emtansine (TDM-1) offering benefits in previously treated patients.1
Immunotherapy
Breast cancer's ability to evade immune responses is partly due to inhibitory interactions between T-cell receptors (such as PD-1, TIM-3, LAG3, TIGIT, and CTLA4) and their ligands on cancer cells, leading to T-cell exhaustion and reduced therapy responsiveness.1 Single-agent immune checkpoint inhibitors (ICIs) have shown limited effectiveness in advanced breast cancer, particularly in metastatic triple-negative breast cancer (TNBC), with modest response rates observed in trials like KEYNOTE-012, KEYNOTE- 086, and JAVELIN.1 However, combining ICIs with chemotherapy has yielded better outcomes, as seen in trials like IMpassion130 and KEYNOTE-522, leading to FDA approval of atezolizumab and pembrolizumab for first-line treatment in PD-L1 positive metastatic TNBC.1 In early-stage breast cancer, the addition of ICIs to neoadjuvant chemotherapy has shown promise, especially in TNBC, though further research is needed to confirm long-term efficacy.1
Gene Therapy
Gene therapy is an emerging approach in breast cancer treatment involving the delivery of genetic material to target cells to modify gene
expression.1 Early trials have demonstrated safety and targeted gene expression in breast cancer, particularly in HER2-positive cases.1 Strategies include gene editing, microRNA therapy, and DNA/RNA vaccination.1 Although still in the experimental phase, gene therapy holds promise for the future, with ongoing trials exploring its potential in treating breast cancer
Care Team Timeout
In the follow-up care of breast cancer patients, PCPs monitor for signs of recurrence, manage any long-term side effects of treatment, and coordinate care with other specialists as needed
They also play a crucial role in providing psychosocial support and addressing the emotional and psychological needs of breast cancer patients, which is an essential aspect of holistic care.
Pharmacists utilize their expertise in drug interactions and adverse effects management to optimize patient outcomes following the initiation of therapies
They work closely with the care team to recommend therapeutic changes as needed and monitor a patient’s adherence to therapy
Pharmacists in community settings can provide cancer education, leading to better patient attitudes toward the disease, improved adherence to treatment, and more effective pain management
Care team barriers to interprofessional collaborative practice include communication gaps, time constraints, keeping up with rapidly evolving treatments, limited patient adherence to treatment plans, navigating complex insurance and financial issues, and managing side effects and complications. These barriers, challenges, and solutions are described in Table 6 below.
Table 6
Care Team Barriers
| Barrier | Challenges | Solutions |
| Communication Gaps | Fragmented care due to poor interdisciplinary communication | - Regular interdisciplinary meetings or case conferences - Integrated electronic health records (EHR) systems for seamless information sharing |
| Time Constraints | Limited time for thorough patient evaluation and management | Delegate non-clinical tasks to support staff Use automated systems for routine processes Prioritize care activities based on patient acuity |
| Keeping Up with Rapidly Evolving Treatments | Difficulty staying current with new drugs and therapies | - Access to continuing education (online courses, webinars, conferences) - Decision support tools within EHRs for evidence- based recommendations |
| Limited Patient Adherence to Treatment | Non-adherence due to side effects, financial constraints, or lack of understanding | - Enhance patient education on adherence and side effect management - Identify and address barriers to adherence (e.g., financial assistance) |
| Navigating Complex Insurance and Financial Issues | Complications from insurance limitations and high treatment costs | - Collaborate with financial counselors and patient navigators - Advocate for clear communication with insurance companies |
| Managing Side Effects and Complications | Challenges in managing side effects like cardiotoxicity, neuropathy, and bone marrow suppression | - Establish early identification and management protocols - Use a multidisciplinary approach involving specialists as needed |
Role of the Pharmacy Technician
The role of pharmacy technicians in ambulatory oncology settings has significantly evolved, expanding beyond traditional tasks like compounding to include a variety of advanced functions.12 Pharmacy technicians now support pharmacists by managing medication preparation, distribution, and handling hazardous drugs.12 They are involved in quality improvement initiatives, ensuring compliance with standards like USP chapters 797 and 800, and assisting in inventory management, including the purchasing and tracking of oncology medications.12 Additionally, pharmacy technicians contribute to patient care by conducting medication histories, assisting with medication reconciliation, and supporting patient education on oral anticancer therapies.12 Technicians can also help patients in less clinical ways, such as securing prior authorizations and minimizing medication waste, further optimizing oncology pharmacy operations.12 Through specialized training and adherence to standardized guidelines, pharmacy technicians are integral to delivering high- quality care in the complex ambulatory oncology environment, including the care of patients with breast cancer.12
Guidelines and Resources
| National Comprehensive Cancer Network (NCCN) |
| American Society of Clinical Oncology (ASCO) |
| European Society for Medical Oncology (ESMO) |
| St. Gallen International Expert Consensus |
| United States Preventive Services Task Force (USPSTF) |
| American College of Radiology (ACR) Appropriateness Criteria |
| Society of Surgical Oncology (SSO) |
| San Antonio Breast Cancer Symposium (SABCS) Consensus |
| American College of Surgeons (ACS) Commission on Cancer (CoC) |
Summary
Breast cancer management requires a coordinated multidisciplinary approach to achieve the best patient outcomes. Physicians and pharmacists, along with other healthcare professionals, must work together to provide comprehensive care that addresses the complex needs of breast cancer patients. Through continued education and collaboration, healthcare professionals can contribute to advancing breast cancer care and improving patient survival and quality of life. As treatment strategies continue to evolve, the roles of pharmacists and primary care physicians in the management of breast cancer will remain critical in ensuring that patients receive the best possible care throughout their journey.
Course Test
Which of the following is considered the cornerstone of treatment for early-stage breast cancer before radiotherapy?
Chemotherapy
Targeted therapy
Surgery
Radiotherapy
What is the primary role of neoadjuvant chemotherapy (NAC) in breast cancer treatment?
To eradicate micrometastases
To reduce tumor size before surgery
To replace surgery in early-stage breast cancer
To prevent recurrence after surgery
Which factor significantly impacts the effectiveness of mammography in breast cancer detection?
Patient’s age
Tumor size
Breast density
Family history of breast cancer
Which of the following is an endocrine-related (hormonal) risk factor for the development of breast cancer?
Late menarche (after age 18)
Late menopause (after age 55)
Having four or more children
Early age of first birth (before age 25)
Mutations in which of the following genes significantly increases an individual’s risk of developing breast cancer?
BRCA1 and BRCA2
ABCC8 and ABCC9
TCFL72 and CAPN10
TP53 and CHEK2
Which of the following is considered the gold standard for definitive diagnosis of breast cancer?
Mammography
Ultrasound
Magnetic resonance imaging
Biopsy
According to the American Cancer Society (ACS), at what age and how frequently should women begin receiving mammograms?
Age 45; every other year
Age 40; every year
Age 50; every year
Age 35; every other year
Which of the following is chemotherapy that is initiated once all other treatments have failed?
Salvage therapy
Adjuvant therapy
Neoadjuvant therapy
Standard therapy
Which of the following agents is used as targeted therapy forHER2+ breast cancer?
Trastuzumab
Tamoxifen
Capecitabine
Docetaxel
Which of the following roles of primary care (PCP) teams, as interdisciplinary team members, is not associated with the PCP management of breast cancer?
PCPs are crucial in assessing a patient’s risk factors, conducting screenings, and guiding patients on preventive measures.
PCPs perform ultrasound, radiotherapy, and surgery to remove the T1 tumor while monitoring for signs of recurrence.
PCPs are often a patient’s first point of contact and can initiate referrals to specialists when necessary.
Once a diagnosis is confirmed, PCPs collaborate with oncologists, surgeons, and other specialists to develop a treatment plan.
References
Wang J, Wu SG. Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives. Breast Cancer (Dove Med Press). 2023;15:721-730. Published 2023 Oct 20. doi:10.2147/BCTT.S432526.
Boster B, Patel NK, Kaushik J. Breast Cancer. In: DiPiro JT, Yee GC, Haines ST, Nolin TD, Ellingrod VL, Posey L. eds. DiPiro’s Pharmacotherapy: A Pathophysiologic Approach, 12th Edition. McGraw Hill; 2023.
Testa U, Castelli G, Pelosi E. Breast Cancer: A Molecularly Heterogenous Disease Needing Subtype-Specific Treatments. Med Sci (Basel). 2020;8(1):18. Published 2020 Mar 23. doi:10.3390/medsci8010018
Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, Stanisławek A. Breast Cancer-Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies-An Updated Review. Cancers (Basel). 2021;13(17):4287. Published 2021 Aug 25. doi:10.3390/cancers13174287
National Cancer Institute. Breast Cancer Risk Assessment Tool: Online Calculator (The Gail Model). National Cancer Institute. Undated. https://bcrisktool.cancer.gov/. Accessed October 14, 2024.
American Cancer Society. Recommendations for the Early Detection of Breast Cancer. ACS. December 19, 2023. https://www.cancer.org/cancer/types/breast-cancer/screening-tests- and-early-detection/american-cancer-society-recommendations-for-the- early-detection-of-breast- cancer.html#:~:text=Women%20between%2040%20and%2044,choos e%20to%20continue%20yearly%20mammograms. Accessed October 14, 2024.
US Preventive Services Task Force. Breast Cancer: Screening. USPSTF. April 30, 2024. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation
/breast-cancer- screening#:~:text=What%20is%20the%20Task%20Force,of%20dying
%20from%20this%20disease. Accessed October 14, 2024.
Wikicommons. Breast Cancer. Wikimedia.org. https://commons.wikimedia.org/wiki/File:Breast_cancer_--_Smart- Servier.jpg. Accessed October 14, 2024.
Wikicommons. Mammo Breast Cancer. https://commons.wikimedia.org/wiki/File:Mammo_breast_cancer_wArro ws.jpg. Accessed October 14, 2024.
Basurto-Hurtado JA, Cruz-Albarran IA, Toledano-Ayala M, Ibarra- Manzano MA, Morales-Hernandez LA, Perez-Ramirez CA. Diagnostic Strategies for Breast Cancer Detection: From Image Generation to
Classification Strategies Using Artificial Intelligence Algorithms. Cancers (Basel). 2022;14(14):3442. Published 2022 Jul 15. doi:10.3390/cancers14143442
ACS. Masectomy. December 20, 2023. https://www.cancer.org/cancer/types/breast-cancer/treatment/surgery- for-breast-cancer/mastectomy.html. Accessed October 14, 2024.
ASHP-HOPA Guidelines on the Roles and Responsibilities of the Pharmacy Technician in Ambulatory Oncology Pharmacy. 2018. https://www.ashp.org/-/media/assets/policy- guidelines/docs/guidelines/pharmacy-technician-role-responsibilities- ambulatory-oncology-pharmacy.pdf. Accessed October 14, 2024.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.