A REVIEW OF BENIGN PROSTATIC HYPERPLASIA
L. Austin Fredrickson, MD, FACP
L. Austin Fredrickson is an assistant professor of internal medicine at Northeast Ohio Medical University, where he serves as core faculty and teaches diagnostics, therapeutics, clinical skills, and health humanities. He is board-certified in general internal medicine and practices rural primary care.
Topic Overview
Within the realm of men’s health conditions, benign prostatic hyperplasia (BPH) is a disorder with major public health consequences. Benign prostatic hyperplasia is a histological diagnosis and refers to a benign growth of prostate tissue. It is a common cause of lower urinary tract symptoms (LUTS) which often progress in prevalence and severity as men age. Patients with BPH require a patient-centered, holistic approach to care that involves improving symptoms and quality of life, preventing disease progression, and minimizing medication side effects. All healthcare providers can play an important role in identifying patients requiring BPH treatment, recommending referrals, and helping the care team with BPH medication management. Further, pharmacists can provide crucial counseling on the appropriate use of BPH medications and help patients to mitigate side effects and avoid harmful drug interactions.
Accreditation Statement:

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number: The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-23-044-H01-P
Pharmacy Technician 0669-0000-23-045-H01-T
Credits: 1 hour of continuing education credit
Type of Activity: Continuing education
Media: Internet/Home Study Fee Information: $4.99
Estimated time to complete activity: 1 hour, including Course Test and course evaluation
Release Date: March 18, 2023 Expiration Date: March 18, 2026
Target Audience: This educational activity is for pharmacists.
How to Earn Credit: From March 18, 2023, through March 18, 2026, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “educational activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives: Upon completion of this educational activity, participants should be able to:
Describe the underlying causes of benign prostatic hyperplasia
Compare and contrast treatment options for BPH
Recall indications, contraindications, side effect profiles, and monitoring parameters for BPH treatments
Disclosures
The following individuals were involved in the development of this activity:
L. Austin Fredrickson, MD, FACP, and Susan DePasquale, MSN, PMHNP-BC. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
ⓒ RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Introduction
Within the realm of men’s health conditions, benign prostatic hyperplasia (BPH) is a disorder with major public health consequences. This course will review the etiology and pathophysiology of BPH and describe available treatment options in detail, including appropriate administration, mechanisms of action, side effects, and contraindications. Each member’s role within the interdisciplinary team caring for patients with BPH is essential. Clinicians must evaluate the patient, consider a differential diagnosis, and provide the patient with a treatment plan that will provide the patient with the best outcome.
BPH: An Overview
Benign prostatic hyperplasia is a histological diagnosis and refers to the benign growth of prostate tissue.1 It is a common cause of lower urinary tract symptoms (LUTS) which often progress in prevalence and severity as men age.1,2 Benign prostatic hyperplasia is associated with significant healthcare costs.2
Patients with BPH require a patient-centered, holistic approach to care that involves improving symptoms and quality of life, preventing disease progression, and minimizing medication side effects. All healthcare providers can play an important role in identifying men requiring BPH treatment, recommending referrals, and helping the entire care team with BPH medication management. Further, clinicians can provide crucial counseling on the appropriate use of BPH medications and help patients to mitigate side effects and avoid harmful drug interactions.
Epidemiology
An estimated 80% of older men will develop histological evidence of BPH, and the clinical incidence of BPH has been estimated at 78% for men aged 80 years old and 60% for men 60 years old.1,2 One study estimated 90% of men aged 45 to 80 will experience some form of LUTS.3 The highest
incidence of BPH occurs around age 65.1 Approximately half of the patients who develop BPH will require treatment for their symptoms.1
Pathophysiology
The prostate is a chestnut-sized gland that is located below the bladder and anterior to the rectum (Figure 1).2,4,5 It surrounds the urethra, which carries urine from the bladder out through the penis.2 The purpose of the prostate is to make fluid for semen, with prostatic fluids comprising between
20 and 40% of ejaculate volume.2 Within the prostate, testosterone is converted by 5-alpha reductase to dihydrotestosterone (DHT), which is a potent stimulator of prostate growth and contributor to BPH pathogenesis.2 Prostate cells have androgen receptors (ARs), and prostate enlargement occurs via androgen stimulation of epithelial ARs and estrogen stimulation of stromal ARs.2
Figure 1. Normal versus Enlarged Prostate
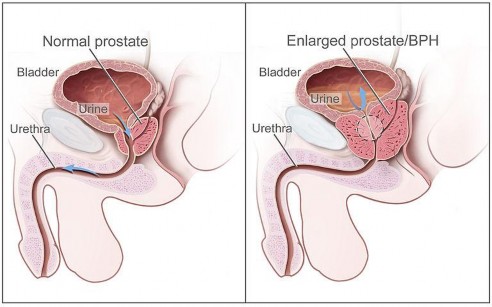
Figure 1 taken from Wikicommons.5
A normal prostate gland weighs between 15 and 20 grams, or about one ounce, in an adult male.2 As part of normal development, the prostate doubles in its initial size during puberty and resumes growing around age 25.2 Patients who develop BPH have an enlarged prostate gland, which can block the bladder outlet and obstruct full urinary flow.2 The larger the prostate grows, the more it squeezes the urethra.2 As the prostate grows, circumferential growth in the outer region may continue for quite some time before it would impede surrounding structures, including vessels and the rectum.2 However, as the urethra is a small-diameter tube, a very small amount of inward growth at that level can cause functional stenosis, or tightening, much sooner than other organs would be affected outside of the prostate.2 This stenosis, over time, can impair urinary excretion, which can cause the bladder wall to thicken and the bladder musculature to become weaker. Urine can then remain in the bladder, leading to the development of LUTS. If the bladder is already partially full after micturition (urination), there is less volume available to fill with urine before the urge to urinate recurs.2 Essentially, the ‘tank’ is never fully emptied, meaning patients must return to urinate more frequently than if they were able to fully empty the bladder, as occurs in healthy urinary systems and normal-sized prostates.
The development of BPH is thought to involve both intraprostatic DHT and Type 2 5-alpha reductase.2 Further, excessive alpha-adrenergic tone of the stromal component of the prostate gland and bladder neck causes the prostate gland to contract around the urethra.2 Benign prostatic hyperplasia is thought to develop in three major and successive stages, which include BPH, benign prostatic enlargement (BPE), and benign prostatic obstruction (BPO).2 In this sequence, histological changes predate tissue enlargement which ultimately can cause urinary obstruction as it grows.
Etiology
Benign prostatic hyperplasia is associated with two risk factor categories, non-modifiable and modifiable.4 These are detailed in Table 1.4
Table 1. Risk Factors for BPH
| Non-modifiable | Modifiable |
| Age | Testosterone |
| Genetics | Dihydrotestosterone |
| Estrogen | |
| Metabolic syndrome | |
| Obesity | |
| Diabetes | |
| Diet | |
| Physical activity | |
| Inflammation |
Table 1 taken from Patel and Parsons (2014)4
Several lifestyle-related factors may contribute to the development of BPH, including poor diet and lack of exercise, metabolic syndrome, and diabetes.4 In one study, men who were diagnosed with metabolic syndrome were 80% more likely to have LUTS compared to those with no metabolic syndrome components.7 Obesity is likely directly correlated with prostate growth, as higher adiposity leads to increased prostate volume.4 Patients who increase physical activity have lower risks of BPH and BPH-related surgeries.4 Studies indicate engaging in moderate-to-vigorous exercise may reduce the risk of BPH by 25% compared to sedentary lifestyles.8
Diagnosis
The American Urological Association (AUA) Management of Benign Prostatic Hyperplasia/ Lower Urinary Tract Symptoms guidelines were last updated in 2021 and offer clinicians assistance in the diagnosis and treatment of BPH.1 Men with BPH most commonly present either as an incidental finding during a rectal examination or radiology test or present symptomatically with LUTS, which are categorized as obstructive or irritative.2 Table 2 lists these symptoms.2 A patient’s symptoms can assist clinicians in determining the cause of BPH.9
Table 2. Lower Urinary Tract Symptoms
| Obstructive Symptoms | Irritative Symptoms |
| Urine hesitancy | Urinary frequency |
| Straining | Nocturia |
| Weak flow | Dysuria |
| Prolonged voiding | Decreased void volume |
| Partial or complete urinary retention | |
| Urinary incontinence |
Table 2 taken from Lee and Sharifi, Benign Prostatic Hyperplasia (2020)2
Prior to diagnosing BPH, clinicians conduct a thorough patient evaluation, including obtaining a medical and medication history and medication history.1,2 Physical examination, including a digital rectal examination, should also be completed.1,2 Clinicians should note the size of the prostate gland does not always correspond to symptoms, and a patient’s perception of symptom severity should be used to guide treatment.2 As detailed above, if the prostate grows on its exterior surface just a few millimeters, the examination may not reveal a very enlarged prostate; however, if the prostate grows inward a few millimeters, it may completely obstruct the urethra.1,2 The AUA Symptom Score is frequently used to evaluate symptoms (Figure 2).9,10 Within this scoring system, a patient evaluates their perception of how bothersome symptoms are based on how they interfere with daily activities or cause embarrassment.9 The AUA guidelines recommend the use of the International Prostate Symptom Score (IPSS). The IPSS is the international version of the AUA Symptom Score which adds a single question assessing the patient’s quality of life based on the patient’s perception of the problem (Figure 3).1 Voiding diaries, in which patients document the number and volume of voids each day, are useful to evaluate symptom severity.2
Figure 2. AUA Symptom Score
| Symptom score point scale |
| Use the following point scale to answer the questions. |
| 0 points means you answered "never" to the question. |
| 1 point means you answered "less than 1 out of 5 times" to the question. |
| 2 points means you answered "less than half of the time" to the question. | ||
| 3 points means you answered "about half of the time" to the question. | ||
| 4 points means you answered "more than half of the time" to the question. | ||
| 5 points means you answered "almost always" to the question. | ||
| Symptom score questions | ||
| 1. Over the past month, how often have you had the feeling of not completely emptying your bladder after you finished urinating? | ||
| 2. Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating? | ||
| 3. Over the past month, how often have you found that you stopped and started again several times when you urinated? | ||
| 4. Over the past month, how often have you found it hard to hold your urine? | ||
| 5. Over the past month, how often have you had a weak urine stream? | ||
| 6. Over the past month, how often have you had to push or strain to begin urination? | ||
| 7. Over the past month, have you had to get up to urinate during the night? Give a score to the number of times. | ||
| 0 means you did not get up at all. | ||
| 1 means you got up 1 time. | ||
| 2 means you got up 2 times. | ||
| 3 means you got up 3 times. | ||
| 4 means you got up 4 times. | ||
| 5 means you got up 5 times or more. | ||
| Score and severity of problem | ||
| Score | Severity | |
| 0 to 7 | Mild | |
| 8 to 19 | Moderate | |
| 20 to 35 | Severe | |
Figure 2 taken from Farrant and Page, Androgens and Benign Prostatic Hyperplasia (2018)10
Figure 3. IPSS Additional Quality of Life Question to AUA Score
| Quality of Life Additional Question |
| If you were to spend the rest of your life with your urinary condition just the way it is now, how would you feel about that? |
| Delighted |
| Pleased |
| Mostly satisfied |
| Mixed |
| Mostly dissatisfied |
| Unhappy |
| Terrible |
Figure 3 taken from American Urological Association Symptom Index 11
Patients are classified as having mild BPH if they are asymptomatic or have only mildly bothersome symptoms, which correlates to a score of 7 or less on the AUA Symptom index.1 Moderate (AUA score of 8-19) and severe (20-35) BPH are differentiated by advancing symptomatology.14
Differential Diagnosis
Urinalysis can be used to rule out conditions such as infections or urolithiasis, as well as many other urological conditions.2 Prostate-specific antigen (PSA) tests can be used to screen for prostate cancer in patients but also can be elevated in patients with larger prostate glands or a history of prostate injury, inflammation, or infection.2 In patients with BPH, the PSA result could be normal or abnormal, and abnormal results do not always imply prostate cancer.12 Clinicians can determine a patient’s peak and average urinary flow in the clinical setting via a uroflowmeter.13 A low urinary flow rate found on uroflowmetry is less than 10-12 mL/s and this indicates bladder emptying may be impacted due to obstruction or functional disorders (including neuromuscular bladder dysfunction).2 A post-void residual (PVR) volume can also be obtained (the normal level is 0 mL).2,13 This is measured via ultrasound, placing the probe suprapubically to evaluate how much urine remains after urination concludes.13 If the PVR volume is 25-50 mL or higher, the bladder is failing to empty adequately.2
Lower urinary tract symptoms can have many causes and benign prostatic hyperplasia is just one of them.9 The patient’s medical history should be evaluated to determine possible causes of lower urinary tract dysfunction and then determine an appropriate treatment.9
A patient could present with obstructive voiding symptoms but not have an enlarged prostate. The cause is likely increased alpha-adrenergic tone.2 Stressful events can also heighten the symptoms of BPH, with a-adrenergic tone causing contraction of prostatic stromal tissue.2
Obstructive urinary symptoms can arise from conditions such as urethral stricture disease or neurogenic voiding dysfunction.9 Urinary urgency and frequency can be due to detrusor overactivity, which may be secondary to BPH; however, neurologic disease, malignancy, initiation of diuretic therapy, high fluid intake, or consumption of bladder irritants such as caffeine, alcohol, and spicy foods can also lead to urological voiding symptoms.9
Urinary frequency may be the result of undiagnosed or poorly controlled diabetes mellitus. Diabetes mellitus may arise because of glucosuria and polyuria.9
Nocturia may be caused by a nonurologic condition.9 It could be from high fluid intake in the evening. Medical conditions may also lead to nocturia. For example, heart failure can cause excess extravascular fluid to shift into intravascular space when the patient lies down, leading to excessive urination.9
Patients with BPH could have hematuria - bleeding from congested prostatic or bladder neck vessels- but there could also be an underlying malignancy or urolithiasis causing urinary obstruction and hematuria. Further evaluation through a urologic workup should be completed.9 The broad differential diagnosis for the different lower urinary tract symptoms highlights the importance of obtaining a thorough history.9
Medications that Exacerbate BPH
Clinicians should be able to recognize medications that exacerbate the symptoms of BPH and should thus be avoided in these patients. Alpha- adrenergic agonists, such as pseudoephedrine and phenylephrine, stimulate alpha-adrenergic receptors in the prostate, leading to muscle contraction.2 Beta-adrenergic agonists, including terbutaline, cause bladder detrusor muscle relaxation, which prevents bladder emptying.2 Anticholinergic agents, antihistamines, phenothiazines, and tricyclic antidepressants can also decrease the contractility of the bladder detrusor muscle.2 Use of these medications can result in urinary retention in patients with a narrowed urethral lumen.2
Polyuria may be unintentionally caused by the use of hypoglycemic agents canagliflozin and dapagliflozin. Canagliflozin and dapagliflozin are used to control glycemic levels by blocking renal glucose reabsorption, thereby inducing urinary glucose loss.9
Management of BPH
The updated AUA guidelines offer treatment suggestions but notably do not clearly define the sequence of treatments for BPH.1 Instead, treatment approaches should be individualized based on a patient’s symptoms (whether obstructive or overactive) and prostate size, and the potential side effects of medication therapy, as well as patient goals.1 Use of the IPSS is recommended to monitor the progress of the patient’s therapy, but there is a lack of evidence to support this recommendation.1
In treating BPH, the central goals are to control and minimize symptoms. This can be objectively measured by at least a 3-point decrease in the AUA symptom index.1 Preventing the progression of BPH and reducing the need for surgical intervention should also be considered when therapeutic options are discussed.2 Patients should be initially counseled on lifestyle modifications, pharmacologic therapies, and potential referrals to discuss surgical options.
Watchful Waiting
Watchful waiting is usually the initial management option for patients with mild BPH.14 This involves regularly reassessing the patient every 6 to 12 months.2 At appointments, patients complete the IPSS or other scoring tool, and objective signs of BPH are assessed or are queried directly as to their symptomatology and quality of life.2 Even though patients are not taking medication at this point, they should be educated on ways to avoid worsening their symptoms.2 Nonpharmacologic methods include minimizing caffeine and alcohol, emptying the bladder frequently when awake, avoiding large amounts of fluids prior to bedtime, and avoiding medications that can worsen symptoms.2
Pharmacologic Treatment
Pharmacologic therapies are indicated for patients with moderate- severe symptoms and those who perceive symptoms to be bothersome.1,2 For these patients, watchful waiting has been associated with untoward outcomes, including increased PVR urine volumes and voiding symptoms.15,16 There are many pharmacologic agents available for treating BPH, including alpha1 adrenergic antagonists, 5 alpha-reductase inhibitors, phosphodiesterase inhibitors, anticholinergic agents, and mirabegron. These medications are described in detail below.
Alpha-1 Adrenergic Antagonists
The AUA guidelines suggest that clinicians offer alpha-1 adrenergic antagonists as a treatment option to patients with bothersome, moderate-to- severe LUTS/BPH.1 This is a moderate recommendation, supported by Grade A evidence.1 The FDA-approved alpha-1 adrenergic antagonists, hereafter referred to as “alpha-blockers” include alfuzosin, doxazosin, tamsulosin, terazosin, and silodosin.17–21
Mechanism of Action and Dosing
Alpha-blockers are used in the management of BPH and can be remembered as they end in the suffix “osin.”22 These medications block the alpha-1 adrenoreceptors in the lower urinary tract.17-21 Smooth muscle tone is facilitated via sympathetic nervous stimulation of alpha-1- adrenoreceptors.17-21 These types of receptors are abundant in the prostate, prostatic urethra, and bladder neck.17-21 When these receptors are blocked, smooth muscle in the bladder and prostate relaxes, improving urinary flow rate and BPH symptoms.17-21 Alpha-blocker dosing is detailed in Table 1.17-21 The choice of an alpha-blocker will depend on the patient’s age, comorbidities, and the side effect profile of the agent selected.22 All alpha-blocking agents are comparable in terms of efficacy and begin to work a few hours or even days after administration.22
Table 3. Alpha-Blocker Dosing
| Generic (Brand) | Dosing |
| Alfuzosin (Uroxatral) | 10 mg once daily |
| Doxazosin (Cardura) | IRa: 1 mg once daily. Titrate by doubling the dose up to 8 mg/day |
| ERb: 4 mg once daily in morning. Titrate up to 8 mg once daily | |
| Silodosin (Rapaflo) | 8 mg once daily with a meal |
| Tamsulosin (Flomax) | 0.4 mg once daily 30 minutes before next meal. Can increase to 0.8 mg once daily |
| Terazosin | 1 mg once daily at bedtime. Titrate slowly every few weeks to a usual dose of 10 mg once daily. Max dose is 20 mg once daily. |
a: Immediate-release b: Extended-release
Table 3 taken from Djavan and Marberger (1999),17 Lexicomp Online (2023)18-21
Administration
Administration varies among the alpha-blockers. Alfuzosin, tamsulosin, and silodosin should be taken within or right after the same meal each day.22
These capsules should never be crushed, chewed, or opened.22 Silodosin can be mixed with applesauce, and doxazosin and terazosin can be taken with or without food.22 After taking any alpha-blocker, patients should be cautioned to not stand or move suddenly given the risk of orthostatic hypotension.17-21
Side Effects and Warnings
Common side effects of alpha-blockers include asthenia (abnormal lack of energy), dizziness, fatigue, lassitude, orthostatic hypotension, palpitations, and peripheral edema.17-22 Patients may also experience nausea, impotence, drowsiness, and vertigo.17-22 The development of ejaculatory disorders is not uncommon.17-21
Contraindications to alpha-blocker therapy include hypersensitivity to these agents; moreover, prostatic carcinoma should be ruled out prior to beginning treatment with an alpha-blocker to not mask symptoms of progressive prostate cancer that need evaluation and management.17-21 Clinicians should be aware of the many precautions associated with alpha- blocker use. This class of medications may cause CNS depression, impairing physical and mental abilities, and patients should be cautioned to not operate machinery or perform tasks that require mental alertness.17-21 Another considerable risk is the development of floppy iris syndrome. This may occur in patients who undergo cataract surgery and who currently take or previously took alpha-blockers.17-22 Floppy iris syndrome involves poor pupil dilation and sudden constriction of the pupils.22 It is recommended that patients stop alpha blockers prior to surgery and then resume treatment once the surgery is complete.22
Alpha-blockers can also cause orthostatic hypotension or syncope to occur.22 This is especially common following the first dose and within the first few days of therapy.22 Increasing the dose of an alpha-blocker and taking an alpha-blocker concurrently with other antihypertensive drugs may also result in orthostatic hypotension.22 These effects are more common with doxazosin and terazosin compared to alfuzosin, tamsulosin, and silodosin.22 Finally,
these agents have the potential to cause priapism (prolonged, painful erection) though the risk is rare.17-21
Alpha-blocker Efficacy
Alpha-blockers have similar efficacy in the treatment of BPH and LUTS and their use for these indications is supported by a plethora of randomized controlled trials and systematic reviews.23-24 Within these studies, no one patient group has been shown to benefit more from alpha-blockers than another.1,23,24 If the use of an alpha-blocker does not improve a patient’s symptoms, it is unlikely another agent will, given their similarities.1 However, it is prudent to change alpha blockers based on side effects.1 Tamsulosin, alfuzosin, and silodosin are less likely to cause orthostatic hypotension.1 However, tamsulosin and silodosin are more likely to cause ejaculatory disorders.1
Patient Monitoring
An evaluation score (AUA or IPSS) should be taken at baseline and then 4-12 weeks after the start of treatment.17-21 Additionally, both objective and subjective signs of BPH and LUTS should be monitored throughout therapy. If alpha-blocker therapy is discontinued, this should be done in a tapered manner with close monitoring of blood pressure.17-21
5-alpha Reductase Inhibitors
5-alpha reductase inhibitors (5ARIs) include dutasteride (Avodart) and finasteride (Proscar).22,25,26 AUA guidelines recommend 5-ARI monotherapy as a treatment option in patients with LUTS/BPH with prostatic enlargement (moderate recommendation, Grade B evidence level).1 Use of dutasteride and finasteride is reserved for patients with prostate volumes >30 mL, PSA >1.5 ng/dL, or palpable prostate enlargement on an exam.1 5-ARIs are the only currently available hormonal therapies able to reduce the influence of androgenic steroids on prostate growth with an acceptable risk/benefit ratio.1 These agents can be used alone or in combination with alpha-blockers to
prevent the progression of LUTs/BPH and to reduce the risk of urinary retention and the need for future surgery.1
Mechanism of Action and Dosing
Dutasteride is an analog of testosterone and competitively and selectively inhibits 5AR types 1 and 2, blocking the conversion of testosterone to dihydrotestosterone and decreasing serum dihydrotestosterone levels.25 It is dosed at 0.5 mg once daily alone or in combination with an alpha-1- adrenergic antagonist.25 Capsules should be swallowed whole.25 Finasteride competitively inhibits type 2 5-alpha reductase, which blocks the conversion of testosterone to dihydrotestosterone, decreasing dihydrotestosterone levels.26 Finasteride is dosed at 5 mg once daily, either alone or in combination with an alpha-1 adrenergic antagonist.26 Finasteride typically needs to be taken for at least 6-12 months to see symptom improvement.1 In general, the larger a patient’s prostate gland, the larger the reduction in prostate volume will be seen with 5ARI use.1
Pharmacokinetic Considerations
5ARIs differ in their pharmacokinetic properties. Finasteride has a half- life of between 3 and 16 hours and dutasteride’s half-life is 5 weeks.22,25,26 Because of this, the adverse effects of dutasteride can persist even after the patient stops taking the medication.22 Additionally, 5ARIs have slow onsets of action and patients should be counseled to expect slow improvement in symptoms. Both medications can be administered with or without food.22
Side Effects and Warning
Dutasteride use is contraindicated in patients with hypersensitivities to dutasteride.25 It should be used cautiously in patients who have diminished urinary flow and those with hepatic impairment.25 Interactions with CYP3A4 inhibitors (such as ketoconazole and erythromycin) can occur, and these should be used cautiously if at all when patients are taking dutasteride.25
Blood donation should be avoided when patients are taking dutasteride to avoid transfusion to a pregnant recipient.25
Dutasteride use is associated with many side effects. The frequency of side effects is highest in the first few months of therapy and tends to decrease after six months.22,25 Side effects include decreased libido, gynecomastia, increased testosterone levels, and increased thyroid-stimulating hormone levels.25 Impotence and ejaculation disorders are also possible.25
Finasteride may cause various forms of sexual dysfunction, including impotence, decreased libido, ejaculatory disorders, and sexual disorders.26 These side effects may continue even after therapy has been discontinued, and sexual dysfunction side effects can result in anxiety, depression, and suicidal ideation.26 These effects are time and dose-related and typically occur between 6-12 months of therapy.26 Older patients and those taking finasteride for greater than 1 year are at the highest risk.26 Although rare, this post- finasteride syndrome should be counseled when initiating patients on this drug.26 Other adverse reactions associated with finasteride include orthostatic hypotension, breast tenderness, decreased ejaculate volume, and high-grade prostate cancer.26 The AUA guidelines give a moderate recommendation to inform patients of the risks of sexual side effects and low risk of prostate cancer before prescribing a 5ARI.1
Efficacy
A direct comparison of finasteride vs dutasteride use has been conducted in one study. Men were randomized to either therapy for 12 months, and no differences in prostate volume, AUA-SI, and Qmax were noted.27 Alone, finasteride, and dutasteride have demonstrated significant improvements in symptom scores compared to placebo.1
Monitoring Therapy
A baseline PSA level should be obtained before therapy and a new PSA should be done at least 6 months following the start of treatment of a 5 alpha-
reductase inhibitor.25,26 IPSS, urinalysis, and objective and subjective signs of BPH and LUTS should be observed.25,26
Muscarinic Receptor Antagonists
Muscarinic receptor antagonists decrease smooth muscle cell contractions in the bladder by inhibiting the muscarinic receptors.22 Agents in this category include tolterodine (Detrol® and Detrol LA®) and fesoterodine (Toviaz®).28,29 Tolterodine is dosed between 1-2 mg twice daily, Detrol LA at 4 mg daily, and fesoterodine between 4-8 mg daily.28,29 They can be taken with or without food and swallowed whole.28,29 Xerostomia (dry mouth) is a common side effect of these medications.28,29 Muscarinic receptor antagonists are recommended for patients who have BPH with OAB symptoms.22 These are add-on therapies used in combination with alpha-blockers.22
Phosphodiesterase-5 Inhibitor (PDE-5)
The AUA guidelines now recommend tadalafil, a PDE-5 inhibitor, for patients with LUTS/BPH, without consideration of comorbid erectile dysfunction.1 This is a newer recommendation within these guidelines. Tadalafil likely mediates a reduction in smooth muscle and endothelial cell proliferation and decreases nerve activity and increased smooth muscle relaxation of the prostate and bladder.1 Tadalafil is dosed at 5 mg once daily.30 If a patient is also taking finasteride, the duration of tadalafil treatment should be limited to 26 weeks.30
Side effects of tadalafil include potential hearing loss (with tinnitus and dizziness) that can occur within 12-24 hours of taking the drug.30 Hypotension may also occur, with reductions in blood pressure of up to 7 mmHg systolic and 5 mmHg diastolic seen.30 This is more likely when tadalafil is used with concurrent antihypertensives, alcohol, and in patients who are fluid-depleted or have autonomic dysfunction.30 Priapism has been reported with tadalafil use, though this is rare.30 It typically occurs within 24 hours of use.30 Finally, visual disturbances (NAION) are possible. The mechanism is not clear, and the onset can vary.30 Risk factors include age >50 years, coronary artery
disease, diabetes, hypertension, hyperlipidemia, and smoking.30 Most cases of NAION are transient, but permanent vision loss if possible.30 Less serious adverse reactions include flushing, dyspepsia, nausea, and headache.30
Mirabegron
Mirabegron (Myrbetriq®) is a beta-3 agonist.31 It activates the beta-3 adrenergic receptors in the bladder, which causes relaxation of the detrusor smooth muscle during the urine storage phase.31 This leads to an increase in bladder capacity.31 Mirabegron is approved for the treatment of overactive bladder symptoms and offers patients a treatment option with a lower rate of anticholinergic side effects.31,32 Mirabegron may be useful for treating OAB in men with BPH that are taking tamsulosin.32 A 2020 meta-analysis of a randomized controlled trial of 1217 BPH patients assessed the efficacy and safety of using mirabegron to treat OAB in men taking tamsulosin therapy.32 Mirabegron was found to significantly decrease the mean number of micturitions per day, the number of urgency episodes per day, the total OAB Symptom score, and the mean volume voided.32 Overall, it was found to be both safe and efficacious in this patient cohort though it may increase the risk of increased post-void residual urine volume.32 For the treatment of OAB, mirabegron is dosed at 25 mg once daily.31 It may be increased to 50 mg once daily after 4-8 weeks if needed based on response and tolerability.31
Combination Therapy
The AUA guidelines provide different recommendations for combination therapy. First, 5-ARIs can be combined with alpha-blockers as a treatment option for patients with LUTS that are associated with prostatic enlargement judged by prostate volume > 30 mL on imaging, a PSA >1.5 ng/dL or palpable prostate enlargement.1 Second, anticholinergic medications can be used in combination with an alpha-blocker for patients with moderate-to-severe predominant storage LUTS.1 Beta-3 agonists can be combined with an alpha- blocker for patients with moderate-to-severe predominate storage LUTS.1 The guidelines note low dose tadalafil should not be combined with alpha-blockers
for the treatment of LUTS/BPH because this combination offers no advantage in the improvement of symptoms versus the use of either medication alone.1
A combination product of dutasteride and tamsulosin) is available.33 Dosing for dutasteride-tamsulosin is 0.5 mg/0.4 mg once daily.33 This combination may help increase adherence versus taking both medications separately.22 This combination has shown considerable efficacy as compared to monotherapy of either agent in improving symptoms and decreasing the progression of BPH.22 Adverse events mimic those seen in monotherapy and may be more pronounced.22,33
Nutraceuticals
Some clinical trial data has found different plant-based and herbal medications demonstrate efficacy in the treatment of LUTS. Current AUA guidelines do not offer extensive guidance on the use of nutraceutical and herbal products.1 Agents such as saw palmetto, stinging nettle, zinc, selenium, and others have been studied and demonstrated efficacy to an extent.1,22 However, these trials suffer from various limitations, including single-center studies, short durations, and poor methodology.22 Two double-blind, placebo- controlled studies evaluated the use of saw palmetto vs placebo in terms of symptoms, bother, quality of life, flowrate recordings, serum PSA, and other measurable parameters.34,35 Both trials found no benefit of saw palmetto over placebo.34,35
Surgical Interventions
If patients are experiencing serious complications because of BPH, surgical corrections should be offered.1,2 Drug therapy in these cases will only delay the worsening of BPH complications.2 Per AUA guidelines, surgery is recommended for patients with renal insufficiency secondary to BPH, refractory urinary retention secondary to BPH, recurrent urinary tract infections (UTIs), recurrent bladder stones or gross hematuria due to BPH, and/or with LUTS/BPH refractory to or unwilling to use other therapies.1 While evaluation for the presence of bladder outlet obstruction can be considered,
clinicians should not perform surgery solely due to the presence of asymptomatic bladder diverticulum.1
The Role of the Clinician
Given the complexity and sensitivity of BPH and LUTS, clinicians must be skilled in addressing them. As mentioned above, the role of the interdisciplinary team in caring for patients with BPH is essential. Clinicians must evaluate the patient, consider a differential diagnosis, and provide the patient with a treatment plan that will provide the patient with the best outcome.
When considering treatment options, clinicians must be aware not only of the indications for pharmacologic treatment, but also of the potential for interactions, adverse events, and cost. Because many of these medications are not fully effective instantaneously, monitoring the progress in patient symptomatology and satisfaction is important and can be completed in an ambulatory clinical setting by trained clinicians via the screening tools listed above or a detailed medical interview. Due to the potential for interactions and adverse events, screening the medication list and performing appropriate medication reconciliation are also critical when prescribing these BPH agents. By remaining patient-centered in conversations with patients on this sensitive topic, clinicians can improve patient care and experience regarding this ubiquitous condition that too often is overlooked and undertreated. Armed with the above knowledge, clinicians can partner with their patients to drastically improve their quality of life and sense of well-being.
Summary
Benign prostatic hyperplasia is a histological diagnosis and refers to the benign growth of prostate tissue. It is a common cause of LUTS which often progress in prevalence and severity as men age. Benign prostatic hyperplasia is associated with significant healthcare costs.
The role of the interdisciplinary team in caring for patients with BPH is essential. Clinicians must evaluate the patient, consider a differential diagnosis, and provide the patient with a treatment plan that will provide the patient with the best outcome.
Treatment approaches should be individualized based on a patient’s symptoms (whether obstructive or overactive) and prostate size, the potential side effects of medication therapy, and the patient’s goals. The use of the IPSS is recommended to monitor the progress of the patient’s therapy, but there is a lack of evidence to support this recommendation.
Course Test
Which of the following statements best describes the relationship between testosterone (T), dihydrotestosterone (DHT), 5-alpha reductase (5AR), and benign prostatic hypertrophy (BPH)?
5AR converts DHT to T in the prostate which leads to BPH
5AR converts T to DHT in the prostate which leads to BPH
There is no relationship between T, DHT, and BPH
BPH causes 5AR to interconvert T and DHT
Which of the following modifiable lifestyle factors has been related to an increased prevalence of LUTS?
Moderate to vigorous exercise
Normal body mass index (BMI)
Metabolic syndrome
Advanced age
Which of the following describes the three major and sequential stages of BPH development?
Benign prostatic hyperplasia (BPH) -> benign prostatic enlargement (BPE) -> benign prostatic obstruction (BPO)
BPH -> BPO -> BPE
BPO -> BPH -> BPE
BPE -> BPH -> BPO
A 55-year-old male patient is referred to a urology clinic with a diagnosis of BPH. Which of the following tools would best stratify the severity of BPH symptoms?
The American Urology Association (AUA) Symptom Score or International Prostate Symptom Score (IPSS)
Prostate-specific antigen level
Urinalysis
Uroflowmetry
When would watchful waiting be most appropriate as a treatment strategy?
When the patient has severe BPH symptoms
When the patient has mild BPH symptoms
When the patient desires to take medications and/or receive surgical intervention
When the patient has moderate BPH and symptoms have become burdensome
Which of the following is most accurate regarding alpha-blocker medications?
They upregulate the alpha-1 adrenoreceptors in the lower urinary tract which results in smooth muscle contraction in the prostate and urethra
Alpha-blockers can be started prior to ruling out prostatic adenocarcinoma
Hypertension frequently occurs so patients are advised to take concurrent beta-blockers
CNS depression or low energy can occur and should be cautioned against
Which of the following is most accurate regarding 5-alpha reductase inhibitors?
They include tamsulosin and doxazosin
They increase conversion of testosterone to DHT
They do not have side effects
Adverse events of dutasteride can persist even after discontinuation due to its long half-life
What is post-finasteride syndrome?
A condition of sexual and/or psychologic adverse events which can continue even after discontinuation
Orthostatic hypotension when used with alpha-blockers
When blood from a patient taking finasteride is given to a pregnant recipient
Nothing that patients need counseling on because of its low incidence
Which of the following correctly relates the medication to its mechanism of action?
Mirabegron is an alpha-1 agonist
Tadalafil is a phosphodiesterase-5 inhibitor
Tamsulosin is a muscarinic receptor antagonist
Dutasteride is a nutraceutical
Which of the following options is most reasonable to recommend, assuming no contraindications?
Brachytherapy (radiation seeds) to the prostate
Low dose tadalafil
Saw palmetto, zinc, and selenium
Combination therapy with either a 5-ARI, anticholinergic agent, or Beta-3 agonist depending on patient factors, goals, and affordability.
References
Lerner LB, McVary, KT, Barry MJ et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline part I, initial work-up and medical management. J Urol. 2021;206:806.
Lee M, Sharifi R. Benign Prostatic Hyperplasia. In: DiPiro JT, Yee GC, Posey L, Haines ST, Nolin TD, Ellingrod V. eds. Pharmacotherapy: A Pathophysiologic Approach, 11e. McGraw Hill; 2020. Accessed February 21, 2023.
Kobayashi S, Tang R, Shapiro E et al. Characterization and localization of prostatic alpha 1 adrenoceptors using radioligand receptor binding on slide-mounted tissue section. J Urol. 1993; 150: 2002.
Patel ND, Parsons JK. Epidemiology and etiology of benign prostatic hyperplasia and bladder outlet obstruction. Indian J Urol. 2014;30(2):170-176. doi:10.4103/0970-1591.126900
Wikicommons. Benign Prostatic Hyperplasia. https://en.wikipedia.org/wiki/Benign_prostatic_hyperplasia#/media/File
:Benign_Prostatic_Hyperplasia_nci-vol-7137-300.jpg. Accessed February 21, 2023.
Roehrborn CG. Benign prostatic hyperplasia: an overview. Rev Urol.
2005;7 Suppl 9(Suppl 9):S3-S14.
Meigs JB, Mohr B, Barry MJ, Collins MM, McKinlay JB. Risk factors for clinical benign prostatic hyperplasia in a community-based population of healthy aging men. J Clin Epidemiol. 2001;54:935–44.
Sarma AV, Parsons JK, McVary K, Wei JT. Diabetes and benign prostatic hyperplasia/lower urinary tract symptoms – What do we know? J
Urol. 2009;182:S32–7.
Unnikrishnan R, Almassi N, Fareed K. Benign prostatic hyperplasia: Evaluation and medical management in primary care. Cleve Clin J Med. 2017;84(1):53-64. doi:10.3949/ccjm.84a.16008
Farrant M, Page ST, Androgens and Benign Prostatic Hyperplasia. Editor(s): Ilpo Huhtaniemi, Luciano Martini. Encyclopedia of Endocrine Diseases (Second Edition), Academic Press, 2018. Pages 775-783. ISBN 9780128122006.
American Urological Association Symptom Index. Kaiser Permanente. https://healthy.kaiserpermanente.org/health-wellness/health- encyclopedia/he.american-urological-association-symptom- index.ug1952. Accessed February 20, 2023.
Angalakuditi M, Seifert RF, Hayes RP, O'Leary MP, Viktrup L. Measurement properties of the benign prostatic hyperplasia impact index in tadalafil studies. Health Qual Life Outcomes. 2010;8:131. Published 2010 Nov 12. doi:10.1186/1477-7525-8-131
Prostate Specific Antigen Test. National Cancer Institute. https://www.cancer.gov/types/prostate/psa-fact- sheet#:~:text=There%20is%20no%20specific%20normal,have%20pro state%20cancer%20(1). Accessed February 20, 2023.
Lepor H. Evaluating men with benign prostatic hyperplasia. Rev Urol.
2004;6 Suppl 1(Suppl 1):S8-S15.
Edwards J. Diagnosis and Management of Benign Prostatic Hyperplasia.
Am Fam Physician. 2008;77(10):1403-1410
Hollingsworth JM, Wilt TJ. Lower urinary tract symptoms in men. BMJ. 2014;349:g4474. Published 2014 Aug 14. doi:10.1136/bmj.g4474
Djavan B, Marberger M. A meta-analysis on the efficacy and tolerability of alpha1-adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic obstruction. Eur
Urol. 1999;36(1):1–13.
Lexicomp Online, Alfuzosin. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Doxazosin. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Tamsulosin. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Terazosin. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Silodosin. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Wu Y, Davidian M, and DeSimmone E. Guidelines for the Treatment of Benign Prostatic Hyperplasia. US Pharm. 2016;41(8):36-40.
Yuan JQ, Mao C, Wong SY et al. Comparative effectiveness and safety of monodrug therapies for lower urinary tract symptoms associated with benign prostatic hyperplasia: a network meta-analysis version 2. Medicine (Baltimore). 2015; 94: 974.
Djavan B, Marberger M. A meta-analysis on the efficacy and tolerability of alpha1-adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic obstruction. Eur Urol. 1999;36:1.
Lexicomp Online, Dutasteride. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Finasteride. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Nickel JC, Gilling P, Tammela TL: Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: the Enlarged Prostate International Comparator Study (EPICS). BJU Int. 2011;108:388.
Lexicomp Online, Detrol. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Toviaz. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Tadalafil. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Lexicomp Online, Mirabegron. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Su S, Lin J, Liang L, Liu L, Chen Z, Gao Y. The efficacy and safety of mirabegron on overactive bladder induced by benign prostatic hyperplasia in men receiving tamsulosin therapy: A systematic review and meta-analysis. Medicine (Baltimore). 2020;99(4):e18802. doi:10.1097/MD.0000000000018802
Lexicomp Online, Jalyn. Waltham, MA: UpToDate, Inc. 2023. https://online.lexi.com. Accessed February 20, 2023.
Bent S, Kane C, Shinohara K et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557.
Barry MJ, Meleth S, Lee JY et al. Complementary and alternative medicine for urological symptoms (CAMUS) study group. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols, and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
ⓒ RxCe.com LLC 2022: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.