ALZHEIMER’S DISEASE MANAGEMENT AND CAREGIVER CARE
ASHLEY WALSH, PharmD
Ashley Walsh is a graduate of the University of Connecticut, School of Pharmacy. She received her Doctor of Pharmacy in 2013. Ashley Walsh had previously a Bachelor of Science in Pharmacy Studies and a Bachelor of Science in Molecular and Cell Biology from the University of Connecticut. She has practiced as a pharmacist since 2013.
Topic Overview:
The factors causing Alzheimer’s disease are not fully known but likely include age, brain changes, family history, and lifestyle. Growing scientific evidence shows healthy lifestyle habits reduce peoples’ risk for Alzheimer’s. Clinicians understand that early diagnosis and intervention are imperative to assist patients with Alzheimer’s disease. Early diagnosis preserves daily function, slows cognitive decline, and delays disease progression. Memory problems are often the first symptom of cognitive decline. Although there is no cure for Alzheimer’s disease, treatment aims to manage symptoms and maintain brain health. Ongoing clinical trials are focusing on more treatments for preclinical and early stages. Caregivers are essential to the provision of patient medication management. Burdened with maintaining or improving the quality of life of a loved one and tasked with caring for patients with a progressive disease, caregivers face their own challenges. Counseling caregivers offer the education and support necessary to optimize patient care and well-being.
Accreditation Statement

RxCe.com LLC is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Universal Activity Number (UAN): The ACPE Universal Activity Number assigned to this activity is
Pharmacist 0669-0000-24-013-H01-P
Pharmacy Technician 0669-0000-24-014-H01-T
Credits: 1.5 contact hour(s) (0.1 5CEU(s)) of continuing education credit
Type of Activity: Knowledge
Media: Internet/Home study Fee Information: $5.99
Estimated time to complete activity: 1.5 contact hour(s) (0.15 CEU(s)), including Course Test and course evaluation
Release Date: February 8, 2024 Expiration Date: February 8, 2027
Target Audience: This educational activity is for pharmacists and pharmacy technicians.
How to Earn Credit: From February 8, 2024, through February 8, 2027, participants must:
Read the “learning objectives” and “author and planning team disclosures;”
Study the section entitled “Educational Activity;” and
Complete the Course Test and Evaluation form. The Course Test will be graded automatically. Following successful completion of the Course Test with a score of 70% or higher, a statement of participation will be made available immediately. (No partial credit will be given.)
Credit for this course will be uploaded to CPE Monitor®.
Learning Objectives:
Upon completion of this educational activity, participants should be able to:
Recognize early symptoms of Alzheimer’s disease
Describe the difference between Alzheimer’s and age-related changes
List Alzheimer’s risk factors
Summarize medications used for Alzheimer’s symptom management and disease treatment
Identify resources and education to provide caregivers during counseling
Disclosures
The following individuals were involved in developing this activity: Ashley Walsh, PharmD, and Pamela Sardo, PharmD, BS. Pamela Sardo was an employee of Rhythm Pharmaceuticals until March 2022 and has no conflicts of interest or relationships regarding the subject matter discussed. There are no financial relationships relevant to this activity to report or disclose by any of the individuals involved in the development of this activity.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.
Educational Activity
Alzheimer's Disease Management and Caregiver Care Introduction
Alzheimer’s disease is a progressive disease that involves cognitive decline, memory loss, and personality changes that lead to a patient’s inability to perform simple daily tasks. There are pharmacological treatments that can manage the symptoms of Alzheimer’s disease, but the patient will invariably need attention and care from a daily caregiver. This course will generally describe pharmacotherapy, patient and caregiver characteristics, counseling and support opportunities, and the need to provide respite care to the caregiver. Treatment plans for Alzheimer’s patients involve a patient- pharmacy team interaction. Pharmacy staff can connect with other healthcare team members and provide resources and assistance to caregivers as they help manage a patient’s condition and medications.
History and Overview of Alzheimer's Disease
Over a century ago, in 1906, Dr. Alois Alzheimer discovered a link between a patient’s cognitive and personality changes and changes within the patient’s brain.1 The patient’s autopsy displayed shrinkage and abnormal deposits in and around the patient’s nerve cells.1 Four years later, Emil Kraepelin, a German psychiatrist who had worked with Dr. Alois Alzheimer, named this condition “Alzheimer’s disease,” after his colleague.1
An estimated 5.8 million Americans were living with Alzheimer’s disease (AD) in 2020. By 2060, researchers expect this estimate to triple to 13.9 million Americans aged 65 years and older who will be living with an AD diagnosis.2
Alzheimer’s is a progressive disease that begins with mild memory loss and leads to a patient’s inability to complete simple daily tasks. Currently, there is no cure. Available interventions temporarily manage symptoms or
slow disease progression. Unfortunately, these medications are ineffective for some patients. Patients responding to treatment will eventually experience decreasing efficacy over time.3 The Alzheimer’s disease drug development pipeline is small and has demonstrated modest success.4 Ongoing clinical trials are researching medications and nonpharmacological interventions addressing the underlying biology.5
Mostly, family members care for patients with AD at home.3,6,7 Family members willingly commit to becoming caregivers for a few reasons. Caregivers may find personal fulfillment and satisfaction from helping a relative. Caregivers can develop new skills and competencies and improve family relationships.7,8 Despite these positives, caregiving is challenging as patients become more dependent on supervision and personal care.3 Caregiving demands may limit the caregivers’ ability to take care of themselves. Neglecting their own health increases the risk of anxiety, depression, and lower quality of life.9
Pathophysiology of Alzheimer's Disease
Scientists lack a complete understanding of AD’s underlying biology. It is a progressive brain disease occurring when abnormal proteins accumulate in the brain (e.g., beta-amyloid and phosphorylated tau) and neurons degenerate.10 Expectantly, as people age, they lose neurons from the brain. However, patients with AD experience far greater neuron loss.11 This loss is not a normal part of aging.3 Other disease hallmarks include brain tissue damage, inflammation, and brain atrophy.10
Alzheimer’s disease’s clinical trajectory includes a preclinical stage, followed by mild cognitive impairment (MCI) and progression to dementia.12 The first brain areas affected by AD are the entorhinal cortex and hippocampus, involved in memory. Later, the disease affects areas in the cerebral cortex responsible for language, reasoning, and social behavior.13,14 This progression is presented in the Figure below.13,14 Importantly, patients with AD pathology may not all progress to clinical phases.12
Figure. Brain Anatomy13
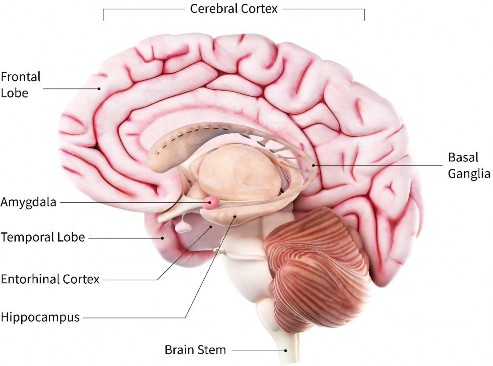
Source: National Institute on Aging, National Institutes of Health
Dementia or Alzheimer's Disease
Dementia is an umbrella term for characteristic difficulties with memory, language, problem-solving, and other thinking skills.10 The most common type of dementia is AD.3 In AD, dementia involves changes in behavior, reasoning, remembering, and thinking.5,10 People can also have dementia-like symptoms without having AD.
Causes for dementia-like symptoms include the following:10
Depression
Delirium
Excessive alcohol consumption
Lyme disease
Medication side effects
Thyroid problems
Untreated sleep apnea
Often, treatment can reverse these conditions. People concerned about dementia should seek medical advice because the differences between normal age-related cognitive changes, medication-induced changes, and AD’s warning signs are subtle.10
Warning Signs and Risk Factors of Alzheimer's Disease
Age, family history, and genetics are risk factors for AD. The greatest risk factor—age—is insufficient on its own to cause AD. Only 5% of people ages 65 to 74 have AD compared to 13.1% of people ages 75 to 84 and 33.3% of people ages 85 or older.10
Family history plays a role in developing AD. People with a first-degree relative (parent or sibling) diagnosed with AD are more likely to develop the disease. People with more than one first-degree relative with AD have an even higher risk.10
Many genes increase AD’s risk, but the apolipoprotein E (APOE) gene has the strongest impact.12 People with the e4 allele are more likely to have beta-amyloid accumulation and AD at a younger age than those with the e2 or e3 allele. Studies suggest geographical background and genetic ancestry alter the extent APOE-e4 contributes to cognitive decline. Additionally, patients with Down Syndrome have an increased risk of developing AD. Scientists believe this is related to having three copies of chromosome 21 (trisomy 21). The gene encoding production of the amyloid precursor protein (APP) is located on chromosome 21. In patients with AD, an enzyme cuts APP into beta-amyloid fragments, and they accumulate into plaques in the brain.10 Also, an estimated 1% of people have a rare genetic mutation causing AD. Inheriting this mutation, called dominantly inherited AD, guarantees disease development within a normal lifespan. Researchers are conducting studies to understand better genetics’ role in developing AD.10
Table 1 lists ten early warning signs identified by the Alzheimer’s Association.16
Table 1
| 10 Early Signs of Alzheimer’s Disease15 | ||
| Signs | Alzheimer’s Disease Examples | Age-related Changes |
| Memory loss disrupting daily life | Forgetting recently learned information | Forgetting appointments, but remembering later |
Challenges with planning or solving problems | Difficulty following a familiar recipe | Occasional errors when managing household bills |
Difficulty completing familiar tasks | Unable to remember rules of a favorite game | Sometimes needing help with recording a TV show |
| Confusion with time or place | Trouble understanding something not happening immediately | Confusion about day of the week but figuring it out later |
Trouble understanding visual images and spatial relationships | Difficulty reading | Cataracts causing vision changes |
New problems with words in speaking or writing | Uses wrong names for familiar objects | Difficulty finding the right word |
| Misplacing things and losing ability to retrace steps | Placing belongings in unusual places | Misplacing belongings sometimes, but able to retrace steps to find them |
| Poor judgment | Paying less attention to grooming | Neglecting to change car oil |
| Withdrawal from work or social activities | Changes in ability to hold or follow conversations | Sometimes feeling uninterested in social obligations |
| Changes in mood and personality | Easily upset, confused, suspicious, depressed, fearful, anxious | Becoming irritable when a routine is disrupted |
*adapted from the Alzheimer's Association
Modifiable Risk Factors of Alzheimer's Disease
Thankfully, growing evidence suggests healthy behaviors may reduce the risk of cognitive decline.3 Patients can improve brain health by10,17
Drinking in moderation
Getting enough sleep
Increasing physical activity
Maintaining a healthy weight
Managing blood sugar
Preventing and managing hypertension and hypercholesterolemia
Quitting smoking
Staying engaged
Early Detection of Alzheimer's Disease
Early diagnosis of AD provides medical, emotional, and social benefits10,18 Patients diagnosed early have the best chance to benefit from treatment. Earlier access to treatment results in reduced cognitive and functional decline. Treatments to address the symptoms may help with decreasing memory loss and confusion. Also, patients have an opportunity to participate in clinical trials to advance research. Early detection gives patients time to prioritize their health. Optimizing and controlling modifiable risk factors may preserve cognition.18 Patients who benefit from early detection also have more time to plan their futures and confront their lives complicated by AD.10,18
Receiving an early AD diagnosis validates the observed symptoms and may reduce anxiety for patients. Family and loved ones have an opportunity to maximize time together. Planning for the future may reduce family burden and prevent disagreements. Patients can review legal documents, discuss finances, and identify care preferences. Families can address safety issues, such as driving or wandering, which are problems associated with later stages.18
Dementia is one of the costliest conditions in society.19 Early detection can save healthcare systems costs with proactive interventions.10,18 The Alzheimer’s Association studied early diagnosis’ impact on potential cost savings. They reported that the United States economy could save an estimated $7 trillion in medical and long-term care costs for patients with AD.10,20 These large cost savings result from a smaller spike in costs immediately before and after diagnosis (during the MCI phase) and lower
medical and long-term costs for people diagnosed and managing MCI and dementia.10
Pharmacists in the community, hospitals, and other settings can refer patients at risk for AD to available inpatient or outpatient services. Easy-open caps or pill organizers may be recommended. Importantly, pharmacists can educate the public about risk factors and prevention measures and encourage early intervention.21 A convenient way to accomplish this is to provide pamphlets in the pharmacy with information about AD. Simplify communication with short sentences and avoid lengthy explanations. Give the person plenty of time (possibly 20 seconds) to respond to questions.
Question:
Would you want to know your Alzheimer’s diagnosis?
Why or why not?
Counseling Caregivers of Patients with Alzheimer's Disease
Inevitably, as the population ages, the number of caregivers grows. Scientists advocate for home-based care because it benefits patients with AD. Family members providing informal care at home can increase patients’ lifespan and delay disease progression.22
Family caregivers focus on the patient, so may be less likely than the general population to practice self-care and preventative healthcare. Caregivers report sleep disturbances, poor eating habits, lack of exercise, failure to rest when ill, and postponing or avoiding scheduling medical appointments for themselves. Also, family caregivers have an increased risk for depression and are more likely to have a chronic illness (e.g., hypercholesteremia, hypertension, obesity, or overweight).23
Frequent interactions and informal conversations with pharmacy teams can lower barriers while building upon existing relationships.10 Pharmacy technicians can recognize caregivers of patients suffering from AD. Since most caregivers are family members, technicians may notice when caregivers pick up medications for others.3 Pharmacy technicians may answer questions about the location of patient care items or safety equipment and should refer identified caregivers to the pharmacist for consultation.
Community pharmacists are easily accessible to caregivers, and they can improve clinical outcomes and quality of life for patients with AD. Throughout AD’s progression, pharmacists are available to assist with managing the disease.21 They can also educate caregivers to enhance their understanding of AD. Caregivers can gently be informed that symptomatic treatment cannot slow or stop the cognitive decline expected in AD. However, available treatments may delay challenging behavior onset and loss of independence. Pharmacists can also counsel and educate, which may ease caregiver burden and delay more intensive care or institutionalism.21
Caregiver Support with Respite Care
On an airplane, the crew advises passengers to put their oxygen masks on before helping others. Only when caregivers prioritize themselves can they effectively help aid the individual under their care.23 Caregiving is often rewarding, but it can become stressful and tiresome.24 One option for caregivers is to maintain their health. This may occur through short breaks. Research demonstrates a few hours per week of respite, or consistent breaks away from caregiving responsibilities, can improve a caregiver’s well- being.24,25 Adult daycare or short-term nursing home care services offer respite care. Family, friends, government agencies, or volunteers can also provide respite care.24,26 Patients with AD may show difficulty adjusting to new environments. Pharmacists may reassure caregivers that regular stays with other care services can make the overall adjustment easier for the patient.26 Some services are available at low or no cost.24
Pharmacists can encourage caregivers to recuperate while emphasizing that their patients are receiving care in a safe environment. Caregivers can use their time away to run errands, catch up with friends and family, or just relax.26 Caregivers may feel guilty about needing outside help or enjoying the time provided by respite.23,26 Pharmacists can remind caregivers that seeking help also benefits their patients. Within a respite setting, the patient interacts with others who have similar experiences, spends time in a safe and supportive environment, and participates in activities matching personal abilities and needs.26
Tips pharmacists can give to caregivers to help alleviate their burnout or guilt include the following:27
Advise caregivers that taking a break can recharge them as they continue to cope
Encourage caregivers to make new connections and speak with other caregivers who have used respite
Propose that caregivers inform others of their request for time away
Support and remind caregivers that their caregiving tasks are helpful
Pharmacists can provide education to caregivers about ways to request help from family and friends. Importantly, caregivers should make their limits and needs known. Suggestions to offer caregivers include the following:24
Being ready to answer when someone asks the caregiver, “What can I do to help?” the caregiver should name a time block or task they need help with
Be empathetic and remind the caregiver to ask for future assistance if someone is unable to help at a specific time
E-mail, text, or call friends and family when help is needed, if caregivers are reluctant to ask directly
Set up a shared online calendar for others to sign up and share tasks or provide regular respite
Developing a Care Plan
Besides prearranged breaks, caregivers can also use respite care in unexpected situations. Emergencies, unplanned circumstances, or unexpected trips necessitate immediate care by an alternative caregiver.26 On these occasions, caregivers should have a written care plan that is easily accessible.24,26
Care plans summarize a patient’s medical conditions and specific care needs. Care plans should include medication doses and administration schedules. Health insurance information, identity of healthcare providers and contact information, and a list of emergency contacts are recommended to include. Care plans improve overall medical management for patients, and caregivers should update them regularly to keep content up to date.9
Tip:
Caregivers can use the comprehensive care plan template provided by the CDC at the following link: cdc.gov/aging/caregiving/pdf/Complete-Care-Plan-Form-508.pdf
Resources for Caregivers
Online support groups offer an opportunity for caregivers to share experiences, get support, and find new resources. The Centers for Disease Control and Prevention (CDC) recommend the following two support groups:24
Family Alliance on Caregiving offers an opportunity to discuss caregivers’ stresses, challenges, and rewards. The link to its website is caregiver.org/connecting-caregivers/support-groups
Caring.com Resource Center provides key resources to better navigate and access online support groups. The link to its website is caring.com/caregivers/
Caregivers can find additional resources and respite care services in
Table 2.24,26,28-35
Table 2
| Services for Caregivers23,25,27-34 | ||
| Information | Organization | Website |
| Respite care | Area Agencies on Aging | eldercare.acl.gov/Public/Index.aspx |
| Alzheimer’s Association | communityresourcefinder.org | |
| Medicare’s PACE program | medicare.gov/health-drug-plans/health- plans/your-coverage-options/other- medicare-health-plans/PACE | |
| National Respite Locator | archrespite.org/caregiver- resources/respitelocator | |
National Volunteer Caregiving Network | nvcnetwork.org/wp/index.php/program- map-2 | |
| U.S. Department of Veterans Affairs | va.gov/GERIATRICS/pages/Respite_Care.as p socialwork.va.gov/Social_Work_Leaders.as p | |
| Additional resources | Family Caregiver Alliance | caregiver.org/caregiver-resources/caring- for-yourself/ |
Powerful Tools for Caregivers (Iowa State University) | powerfultoolsforcaregivers.org/caregivers | |
| PACE = Program of All-inclusive Care for the Elderly | ||
Since caregiving can lead to burnout, prevention is crucial to avoid depression.36 Burnout symptoms include the following:27
Difficulty coping with daily demands
Exhaustion
Frustration
Impatience
Overwhelming feelings
Pharmacists can play a key role in helping caregivers identify and recognize warning signs of frustration in themselves. This can help alert caregivers that they need to take immediate action to calm down. Common warning signs include the following:37
Chest pains
Compulsive eating
Desire to strike out
Excessive alcohol consumption
Headache
Increased smoking
Knot in throat
Lack of patience
Shortness of breath
Stomach cramps
There are a variety of ways for caregivers to calm themselves. It may seem overly simplistic, but caregivers can slowly count to ten and take deep breaths. They can take a walk or relocate to another room to collect their thoughts. Caregivers can also talk with a friend, listen to music, meditate, pray, sing, or take a relaxing bath.37
Question:
How could your pharmacy offer information about respite care services available in your community?
Managing Medications
Approximately 77% of caregivers report a need to ask for advice about medications.23 Pharmacists can provide support and information to increase caregiver knowledge about treatments’ adverse effects, administration or adherence issues, and drug interactions.21 Pharmacists can screen patient
profiles for inappropriate medications and recommend discontinuation to the prescriber. Occasionally, a pharmacist may engage in shared decision-making with a caregiver and prescriber.
The Food and Drug Administration (FDA) has approved eight medications for AD (see Table 3).38-47 Six manage symptoms (brexpiprazole, donepezil, galantamine, rivastigmine, memantine, and memantine + donepezil), and two (aducanumab and lecanemab) slow cognitive decline.10,38 After a time, the caregiver may comment that the patient is getting less benefit from the medication. A pharmacist may reply that, unfortunately, as the disease progresses, medications lose their effectiveness.38
Table 3
| Medications Used for Alzheimer’s Disease. 37-46 | |||
| Classification | Medication | Administration and Frequency | Side Effects |
| Atypical antipsychotic | Brexpiprazole | Oral tablet, daily | Common cold symptoms, dizziness, hyperglycemia, hypertension, stroke |
| Cholinesterase inhibitors | Donepezil | Oral tablet, ODT, or solution, daily | Diarrhea, fatigue, insomnia, muscle cramps, nausea, vomiting, weight loss |
| Galantamine | Oral extended-release capsule, daily or oral tablet or solution, twice daily | Decreased appetite, diarrhea, dizziness, headache, nausea, vomiting, weight loss | |
| Rivastigmine | Oral capsule or solution, twice daily or transdermal patch, replaced daily | Anorexia, nausea, decreased appetite, diarrhea, indigestion, muscle weakness, vomiting, weight loss | |
| NDMA antagonist | Memantine | Oral extended-release capsule, tablet, or solution, daily | Confusion, constipation, diarrhea, dizziness, headache |
NDMA antagonist + cholinesterase inhibitor | Memantine + Donepezil | Oral extended-release capsule, daily | Anorexia, diarrhea, dizziness, ecchymosis*, |
headache, nausea, vomiting | |||
| Monoclonal antibodies | Adacanumab | IV, over 1 hour every 4 weeks | ARIA, brain swelling and bleeding, confusion, diarrhea, dizziness, falls, headache |
| Lecanemab | IV, over 1 hour every 2 weeks | ARIA, brain swelling and bleeding, headache, cough, diarrhea, nausea, vomiting, fever, chills, body aches, fatigue, high blood pressure, low blood pressure, and low oxygen | |
ARIA = amyloid related imaging abnormalities Ecchymosis = small bruising from leaking blood vessels IV = intravenous ODT = orally disintegrating tablets | |||
Mild to Moderate Disease
In mild to moderate AD, cholinesterase inhibitors (e.g., donepezil, galantamine, and rivastigmine) are used to reduce cognitive and behavioral symptoms. However, these are not the only medications the patient may be prescribed. Caregivers of individuals with Alzheimer’s may be faced with the reality of multiple physicians and multiple medications. Pharmacist counseling with caregivers may include risks of drug interactions, such as donepezil and galantamine, which have the potential to interfere with anticholinergic medications.41 Patients taking rivastigmine should avoid using beta-blockers, for example, due to the additive risk of bradycardia. Pharmacy teams may discover a patient profile has cholinomimetic and anticholinergic medications (e.g., oxybutynin and tolterodine).46 Pharmacists can check patient profiles and recommend potential changes to caregivers and prescribers.
Pharmacists and pharmacy technicians are ideally positioned to inform caregivers of dosing and administration. Unlike orally administered medications indicated for AD, lecanemab and aducanumab’s administration route is intravenous (IV).39,40
A caregiver may share the frustration that they must take the patient for ‘scans.’ This is an opportunity to share, in simpler terms, that prior to initiating treatment, positron emission tomography (PET) scans or cerebrospinal fluid must confirm amyloid beta pathology.38-40 Intracerebral hemorrhage has been reported in patients also taking antithrombotics, antiplatelets, or anticoagulants.39,40 Exercising caution, pharmacists can screen and counsel patients and caregivers to avoid potentially risky concurrent therapy. To monitor this potential risk of intracerebral hemorrhage, lecanemab, and aducanumab require routine magnetic resonance imaging (MRI).38-40
Caregivers may tell the pharmacist that they are confused because the provider talked about ‘an area’ and they wonder what that means. Pharmacists can help the caregiver, in lay terms, understand that they heard ‘area,’ but the prescriber was stating ‘ARIA.’ Lecanemab and aducanumab have a boxed warning for amyloid-related imaging abnormalities (ARIA).39,40 Typically, ARIA resolves over time, and patients with temporary, localized brain swelling are asymptomatic. Amyloid-related imaging abnormalities can be signals of serious and life-threatening events. Symptoms associated with ARIA include headache, confusion, visual changes, dizziness, nausea, and difficulty walking.48 Shared decision-making can determine whether a treatment’s potential benefits outweigh its risks.39,40
Moderate to Severe Disease
Caregivers may read about memantine and ask questions. It can decrease symptoms, potentially enabling patients to maintain independent daily functioning longer. Since memantine works differently than cholinesterase inhibitors, using a combination is acceptable (e.g., donepezil + memantine).38 Patients taking memantine, alone or in combination with donepezil, should avoid concurrently taking NMDA antagonists (e.g., ketamine, dextromethorphan) and medications that make urine alkaline (e.g., carbonic anhydrase inhibitors and sodium chloride).44,45 Clinicians should not confuse NMDAs with NDMA antagonists that are used to treat Alzheimer’s
disease. Donepezil’s drug interactions mentioned earlier also apply to the combination medication.41,46
Pharmacists are optimally positioned to ask a caregiver to share the patient's symptoms with them. Brexpiprazole, for example, treats agitation associated with AD but has a boxed warning for increased mortality in elderly patients with dementia-related psychosis.42
Managing Behavioral Symptoms
Aggression, agitation, anxiety, depression, restlessness, sleeplessness, and wandering are common AD symptoms that a caregiver may discuss with the pharmacy team. Treating these symptoms may provide patients with dignity and independence for a longer time and relieve caregiver stress.
Caregivers of a patient with Alzheimer’s may approach the pharmacy counter with over-the-counter sleep aids for the patient and complain that they are not sleeping because the patient is not sleeping. A pharmacy technician should refer this issue to the pharmacist. Sleep aids can make a patient with AD more confused and more likely to fall.38 The pharmacist can educate the caregiver that AD often changes sleeping patterns, but caregivers can take steps to keep their patients safe overnight. Caregivers can ensure the floor is clutter-free, lock away medications, attach grab bars in the bathroom, and place a gate across any stairways.49
Question:
What questions would you anticipate from caregivers related to Alzheimer’s disease medications?
Future Studies
The National Institute on Aging is currently supporting over 400 clinical trials on AD and related dementias. Trials in Phase II/III have an anticipated completion date within the next three years. Beyond symptom management, disease-modifying drugs and other studied targets hold promise to treat AD effectively in the future.50
Summary
Alzheimer’s is a progressive disease that begins with mild memory loss and leads to a patient’s inability to complete simple daily tasks. Currently, there is no cure. Available interventions temporarily manage symptoms or slow disease progression for some patients.
Scientists lack a complete understanding of AD’s underlying biology. It is a progressive brain disease occurring when abnormal proteins accumulate in the brain and neurons degenerate. Age, family history, and genetics are risk factors for AD. Many genes increase AD’s risk. The APOE gene has the strongest impact.
Early diagnosis of AD provides medical, emotional, and social benefits. Patients diagnosed early have the best chance to benefit from treatment. Dementia is one of the costliest conditions in society. Early detection helps reduce these costs.
Family caregivers are less likely than the general population to practice self-care and preventative healthcare. Caregivers report sleep disturbances, poor eating habits, lack of exercise, failure to rest when ill, and postponing or avoiding scheduling medical appointments for themselves. Also, family caregivers have an increased risk for depression and are more likely to have a chronic illness.
Pharmacists can encourage caregivers to take time for themselves, suggesting respite and other self-care and recuperation. Caregivers can use
their time away to run errands, catch up with friends and family, or just relax. Pharmacy technicians may answer questions about the location of patient care items or safety equipment and should refer identified caregivers to the pharmacist for consultation.
Approximately 77% of caregivers report a need to ask for advice about medications. Pharmacists can provide support and information to increase caregiver knowledge about treatments’ adverse effects, administration or adherence issues, and drug interactions. Pharmacists can screen patient profiles for inappropriate medications and recommend discontinuation to the prescriber. Occasionally, a pharmacist may engage in shared decision-making with a caregiver and prescriber.
Course Test
Which of the following is an early sign of Alzheimer’s disease?
Difficulty completing familiar tasks like the rules of a favorite game
Becoming irritable when a routine is disrupted, such as bedtime
Misplaces belongings but is able to retrace steps to find them
Sometimes needs help recording a favorite television show
Which risk factors for Alzheimer’s disease are modifiable?
Smoking cessation and genetics
Genetics and getting enough sleep
Smoking cessation and engaging in exercise
Genetics and drinking alcohol
Which of the following is an early warning sign of Alzheimer’s disease?
Patient develops cataracts that cause vision changes
Patient pays less attention to personal grooming
The patient makes an occasional error with paying bills
Patient neglects to change the oil in their car
Which resource would you recommend caregivers use to locate respite care?
National Institute on Aging
Centers for Disease Control
Federal Drug Administration
Area Agencies on Aging
A caregiver is concerned about the overnight behaviors of a patient with Alzheimer’s disease. What might be one recommendation?
Start patient on zolpidem
Gate stairways in the patient’s residence
Initiate patient on zaleplon
Have the patient sleep during the day
Which medications slow mild cognitive impairment in Alzheimer’s disease?
Letamine and dextromethorphan
Donepezil and rivastigmine
Galantamine and memantine
Lecanemab and aducanumab
Which of the following statements about Alzheimer’s disease is TRUE?
Family history is the biggest risk factor for developing Alzheimer’s.
People with a first-degree relative are more likely to be diagnosed.
Withdrawal from social activities is an age-related change.
Challenges with solving problems are age-related changes.
A patient with Alzheimer’s has a prescription for rivastigmine. Which medication would you recommend the prescriber discontinue?
Sodium chloride
Propranolol
Clopidogrel
Ibuprofen
What statement is TRUE about medications for symptom management in Alzheimer’s?
Anticonvulsants and benzodiazepines are most effective
Galantamine is available as a transdermal patch
Brexpiprazole side effects include common cold symptoms
Adacanumab and lecanemab are administered orally
A caregiver for an Alzheimer’s patient approaches you for advice about how to stop her feeling a knot in her throat and her lack of patience with the patient. One suggestion to the caregiver after discussion and screening with open-ended questions from the pharmacist is
to start memantine in the patient.
to monitor for ARIA in the patient.
to avoid meditation.
to consider respite care.
References
Alzheimer’s Association. Milestones. Updated 2023. https://www.alz.org/alzheimers- dementia/research_progress/milestones. Accessed October 21, 2023.
Matthews KA, Xu W, Gaglioti AH, et al. Racial and ethnic estimates of Alzheimer's disease and related dementias in the United States (2015- 2060) in adults aged ≥65 years. Alzheimers Dement. 2019;15(1):17-
24. doi:10.1016/j.jalz.2018.06.3063
alzheimers.html. Accessed October 16, 2023.
Cummings JL, Morstorf T, Zhong K. Alzheimer's disease drug- development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37. Published 2014 Jul 3. doi:10.1186/alzrt269
National Institutes on Aging at the National Institutes of Health. What is Alzheimer’s disease? Alzheimers.gov. https://www.alzheimers.gov/alzheimers-dementias/alzheimers-disease. Accessed October 16, 2023.
Centers for Disease Control and Prevention. Caregiving for a person with Alzheimer’s disease or a related dementia. Alzheimer’s disease and healthy aging. Updated June 30, 2023. https://www.cdc.gov/aging/caregiving/alzheimer.htm. Accessed October 16, 2023.
Centers for Disease Control and Prevention and the Kimberly-Clark Corporation. Assuring Healthy Caregivers, A Public Health Approach to Translating Research into Practice: The RE-AIM Framework. Neenah, WI: Kimberly-Clark Corporation; 2008.
Family Caregiver Alliance (2006a). Caregiver assessment: Principles, guidelines and strategies for change. Report from a National Consensus Development Conference. Volume I. San Francisco, CA: Family Caregiver Alliance.
Centers for Disease Control and Prevention. Maintaining a care plan. Alzheimer’s disease and healthy aging. Updated October 28, 2022. https://www.cdc.gov/aging/publications/features/caregivers- month.html. Accessed October 16, 2023.
2023 Alzheimer's disease facts and figures. Alzheimers Dement. 2023;19(4):1598-1695. doi:10.1002/alz.13016
National Institutes of Health. Understanding different types of dementia. nia.nih.gov.
https://www.nia.nih.gov/health/infographics/understanding-different- types-dementia. Accessed October 16, 2023.
Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):280-
292. doi:10.1016/j.jalz.2011.03.003
National Institutes of Health. Scientific images. nia.nih.gov. https://www.nia.nih.gov/news/aging-alzheimers-resources- multimedia#scientific. Accessed October 21, 2023.
National Institutes of Health. What happens to the brain in Alzheimer's disease? nia.nih.gov. Updated May 16, 2017. https://www.nia.nih.gov/health/what-happens-brain-alzheimers- disease. Accessed October 16, 2023.
Blanchard JW, Akay LA, Davila-Velderrain J, et al. APOE4 impairs myelination via cholesterol dysregulation in oligodendrocytes. Nature. 2022;611(7937):769-779. doi: 10.1038/s41586-022-05439-w
Alzheimer’s Association. 10 early signs and symptoms of Alzheimer's and dementia. alz.org. Updated 2023. https://www.alz.org/alzheimers- dementia/10_signs. Accessed October 16, 2023.
Centers for Disease Control and Prevention. Healthy body, healthier brain. Alzheimer’s disease and healthy aging. Updated May 29, 2020. https://www.cdc.gov/aging/publications/features/healthy-body- brain.html. Accessed October 16, 2023.
Alzheimer’s Association. Why get checked? alz.org. Updated 2023. https://www.alz.org/alzheimers-dementia/diagnosis/why-get-checked. Accessed October 16, 2023.
Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of dementia in the United States. N Engl J Med. 2013; 368: 1326- 1334.
2018 Alzheimer's disease facts and figures. Alzheimers Dement.
2018;14(3):408-411.
Zerafa N, Scerri C. Knowledge and pharmacological management of Alzheimer's disease by managing community pharmacists: a nationwide study. Int J Clin Pharm. 2016;38(6):1416-1424. doi:10.1007/s11096- 016-0380-8
Hellis E, Mukaetova-Ladinska EB. Informal Caregiving and Alzheimer's Disease: The Psychological Effect. Medicina (Kaunas). 2022;59(1):48. Published 2022 Dec 27. doi:10.3390/medicina59010048
Family Caregiver Alliance. Taking care of you: self-care for family caregivers. caregiver.org. Updated 2023. https://www.caregiver.org/resource/taking-care-you-self-care-family- caregivers/. Accessed October 18, 2023.
Centers for Disease Control and Prevention. Caring for yourself when caring for another. Alzheimer’s disease and healthy aging. Updated June
30, 2023. https://www.cdc.gov/aging/publications/features/caring-for-
yourself.html. Accessed October 16, 2023.
Zarit SH, Whetzel CA, Kim K, et al. Daily stressors and adult day service use by family caregivers: effects on depressive symptoms, positive mood, and dehydroepiandrosterone-sulfate. Am J Geriatr Psychiatry. 2014;22(12):1592-1602. doi:10.1016/j.jagp.2014.01.013
Alzheimer’s Association. Respite care. alz.org. Updated 2023. https://www.alz.org/help-support/caregiving/care-options/respite-care. Accessed October 16, 2023.
Family Caregiver Alliance. Respite tips: taking a break from giving care to someone in need. caregiver.org. Updated 2023. https://www.caregiver.org/resource/respite-tips-taking-break-giving- care-someone-need/?via=caregiver-resources,caring-for- yourself,stress. Accessed October 16, 2023.
U.S. Department of Veterans Affairs. Respite care.va.gov. Updated October 18, 2023. https://www.va.gov/GERIATRICS/pages/Respite_Care.asp. Accessed October 18, 2023.
U.S. Administration on Aging. Eldercare locator. eldercare.acl.gov. https://eldercare.acl.gov/Public/Index.aspx. Accessed October 18, 2023.
ARCH National Respite Network. National Respite Locator Service. archrespite.org. Updated 2023. https://archrespite.org/caregiver- resources/respitelocator/. Accessed October 18, 2023.
National Volunteer Caregiving Network. Volunteer Caregiving Around the Nation! nvcnetwork.org. Updated 2023. https://nvcnetwork.org/wp/index.php/program-map-2/. Accessed October 21, 2023.
Medicare.gov. PACE. Medicare.gov. https://www.medicare.gov/health- drug-plans/health-plans/your-coverage-options/other-medicare-health- plans/PACE. Accessed October 16, 2023.
Alzheimer’s Association and AARP. Community resource finder. alz.org and aarp.org. Updated 2023. https://www.communityresourcefinder.org. Accessed October 22, 2023.
Powerful Tools For Caregivers. For caregivers. powerfultoolsforcaregivers.org. Updated 2023. https://www.powerfultoolsforcaregivers.org/. Accessed October 21, 2023.
yourself/. Accessed October 22, 2023.
Pudelewicz A, Talarska D, Bączyk G. Burden of caregivers of patients with Alzheimer's disease. Scand J Caring Sci. 2019;33(2):336-341. doi:10.1111/scs.12626
Family Caregiver Alliance. Dementia, caregiving, and controlling frustration. caregiver.org. Updated 2023. https://www.caregiver.org/resource/dementia-caregiving-and- controlling-frustration/?via=resource,taking-care-you-self-care-family- caregivers. Accessed October 18, 2023.
National Institutes of Health. How is Alzheimer's disease treated? nia.nih.gov. Updated September 12, 2023. https://www.nia.nih.gov/health/how-alzheimers-disease- treated#future. Accessed October 18, 2023.
Aduhelm. Prescribing information. Biogen Inc; 2023.
Leqembi. Prescribing information. Eisai Inc; 2023.
Aricept. Prescribing information. Eisai Inc; 2021.
Rexulti. Prescribing information. Otsuka American Pharmaceutical Inc; 2023.
Razadyne. Prescribing information. Janssen Pharmaceuticals Inc; 2015.
Namzaric. Prescribing information. Allergan, Inc; 2019.
Namenda. Prescribing information. Forest Pharmaceuticals, Inc;2013.
Exelon. Prescribing information. Novartis Pharmaceuticals Corporation; 2018.
Exelon Patch. Prescribing information. Novartis Pharmaceuticals Corporation; 2020.
Hampel H, Elhage A, Cho M, Apostolova LG, Nicoll JAR, Atri A. Amyloid- related imaging abnormalities (ARIA): radiological, biological and clinical characteristics. Brain. 2023;146(11):4414-4424. doi:10.1093/brain/awad188
National Institutes of Health. Alzheimer’s disease and sleep—a special problem. nia.nih.gov. Updated November 03, 2020. https://www.nia.nih.gov/health/good-nights-sleep#alzheimers. Accessed October 21, 2023.
National Institute on Aging. NIA-funded active Alzheimer’s and related dementias clinical trials and studies. nia.nih.gov. Updated March 2023. https://www.nia.nih.gov/research/ongoing-AD-trials#section2. Accessed October 12, 2023.
DISCLAIMER
The information provided in this course is general in nature, and it is solely designed to provide participants with continuing education credit(s). This course and materials are not meant to substitute for the independent, professional judgment of any participant regarding that participant’s professional practice, including but not limited to patient assessment, diagnosis, treatment, and/or health management. Medical and pharmacy practices, rules, and laws vary from state to state, and this course does not cover the laws of each state; therefore, participants must consult the laws of their state as they relate to their professional practice.
Healthcare professionals, including pharmacists and pharmacy technicians, must consult with their employer, healthcare facility, hospital, or other organization, for guidelines, protocols,
and procedures they are to follow. The information provided in this course does not replace those guidelines, protocols, and procedures but is for academic purposes only, and this course’s limited purpose is for the completion of continuing education credits.
Participants are advised and acknowledge that information related to medications, their administration, dosing, contraindications, adverse reactions, interactions, warnings, precautions, or accepted uses are constantly changing, and any person taking this course understands that such person must make an independent review of medication information prior to any patient assessment, diagnosis, treatment and/or health management. Any discussion of off-label use of any medication, device, or procedure is informational only, and such uses are not endorsed hereby.
Nothing contained in this course represents the opinions, views, judgments, or conclusions of RxCe.com LLC. RxCe.com LLC is not liable or responsible to any person for any inaccuracy, error, or omission with respect to this course, or course material.
© RxCe.com LLC 2024: All rights reserved. No reproduction of all or part of any content herein is allowed without the prior, written permission of RxCe.com LLC.